- 136 -
KISEP Original Articles J Rhinol 6((((2)))), 1999
Megadose Steroids and Intranasal Optic Nerve Decompression in the Treatment of Traumatic Optic Neuropathy
Sea-Yuong Jeon, M.D., Cheon-Gyu Kim, M.D., Tae-Gee Jung, M.D. and Eui-Gee Hwang, M.D.
ABSTRACT
Background and Objectives:Traumatic optic neuropathy (TON) is a relatively rare complication associated with closed head injury. However, it represents an extremely poor prognosis, and its management remains controversial. We present the treatment results of 15 patients with immediate and complete TON who were treated with megadose steroids (MDS), and, in cases where MDS produced no response, intranasal optic nerve decompression (OND). Patients and Methods:The diagnosis of TON was based on evidence of the following:complete loss of vision, absence of direct pupillary light reflex and intact co- nsensual response. All of the patients underwent high resolution CT scans of the orbit and received a complete neuro-opthalmo- logic examination. MDS was started immediately after the diagnosis. If no response occurred by 48 hours, an intranasal OND was conducted. Results:Two of the 15 patients exhibited improved vision after treatment with MDS, and six of the remaining 13 patients who were unresponsive to MDS demonstrated improved vision after OND. Overall, eight out of the 15 patients exp- erienced improved vision. Conclusion:This study is uncontrolled, but suggests that our protocol of MDS and, in cases where this produced no response, OND may be an effective and valid treatment modality for patients with immediate complete TON, which is generally believed to represent an extremely poor prognosis regardless of treatment.
KEY WORDS:Traumatic optic neuropathy·Megadose steroids·Optic nerve decompression.
INTRODUCTION
Traumatic optic neuropathy (TON) is defined as tra- umatic loss of vision without evidence of injury to the eye or optic nerve.1) The condition is a relatively rare co- mplication associated with closed head injury,2) but it represents an extremely poor prognosis when the blind- ness is immediate and complete.3) Moreover, the mana- gement of TON is controversial. The rarity and severity of TON makes the performance of a controlled treatment study impossible, so some clinicians choose not to treat the condition,5) while others may use corticosteroids6) or surgical decompression.7) Of the latter group, some prefer early surgical decompression in combination with cort- icosteroids4) and others reserve the surgical treatment for cases unresponsive to corticosteroids.3)8)9) A recent meta-
analysis of the treatment of TON concludes that admin- istering corticosteroids, conducting surgical decompression, or both, is better than no treatment, although no signif- icant difference was found between the two treatment modalities.10)
We have been treating patients with TON with meg- adose steroids (MDS) and, in cases where this produced no response, intranasal optic nerve decompression, (OND) since 1994. We present the results of these modalities in 15 patients with immediate and complete TON.
PATIENTS AND METHODS
Patients with TON were referred to our department following a diagnosis based on evidence of loss of vision, absence of direct pupillary light reflex and intact cons- ensual response. All of the patients underwent high re- solution CT scans of the orbit with soft tissue and bone window settings and received a complete neuro-opthal- mologic examination. Patients indicating light perception abilities or eyeball trauma or some other form of ocular lesion were excluded.
Fifteen patients varying in age from 14 to 62 years were diagnosed with immediate complete TON following Department of Otorhinolaryngology, GyeongSang National Un-
iversity, Hospital, Chinju, Korea
Address correspondences and reprint requests to Sea-Yuong Jeon, MD, Department of Otorhinolaryngology, GyeongSang National University Hospital, Chilamdong 92 Chinju, 660-702, Korea
Tel:82-591-750-8174, Fax:82-591-759-0613 E-mail:[email protected]
Accepted for publication on August 15, 1999
Jeon et al:Treatment of Traumatic Optic Neuropathy / 137
head injury. Some of the patients indicated maxillofacial fractures, such as a blowout fracture, a frontal sinus fr- acture or a tripod fracture, confirmed by preoperative CT scans (Table 1).
MDS was administered at an initial dose of 3/4 mg dexamethasone/Kg and then at 1/4 mg/Kg every six hours for the next 48 hours. If no response was observed by 48 hours, an intranasal OND was conducted. Patients demonstrating improved vision during the course of the MDS were not treated with OND. That is, we performed
the procedure only on patients with immediate complete TON unresponsive to MDS (Fig. 1).
The OND was conducted under general anesthesia via the intranasal approach with an operating microscope. In general, we followed the surgical technique of microsc- opic intranasal decompression of the optic nerve descr- ibed by Takahashi.11) One modification we made was to cover the exposed optic nerve with autologous septal mucosa supported with Gelform soaked with a broad sp- ectrum antibiotic solution. A postoperative antibiotic was applied for two weeks following. Follow-up neuro-opt- halmologic examinations were conducted daily for a week after OND, then weekly for a month thereafter.
RESULTS
The interval between injury and treatment varied, ra- nging from 12 hours to five days. Of the 15 patients in our series, two patients recovered the ability to perceive light after MDS, but the remaining 13 patients were fo- und to be unresponsive and subsequently underwent OND.
Six of the 13 patients were able to perceive light one to six days after OND. In total, eight out of the 15 patients eventually demonstrated improved vision (Table 2). In general the recovery of the vision was partial and limited to finger counting, but one patient recovered serviceable vision and was able to perceive color information. Fol- low-ups ranged in duration from three to 40 months (Ta-
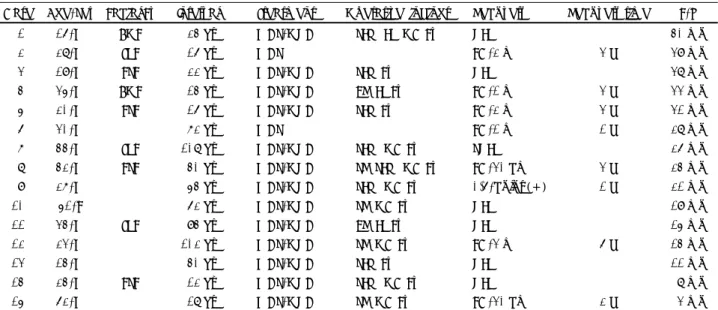
Table 1. Summary of 15 patients treated with megadose steroids and intranasal optic nerve decompression
Case Age/Sex Facial Fx Interval Treatment Operative findings Recovery Recovery time F/U
1 16/M BOF 24 hr MDS/OND SLW, LP, OC Fx NLP 40 mo
2 28/M TPF 16 hr MDS FC/2 m 3 d 39 mo
3 19/M FSF 22 hr MDS/OND SLW Fx NLP 38 mo
4 35/M BOF 14 hr MDS/OND ER, LP Fx FC/1 m 3 d 33 mo
5 20/M FSF 16 hr MDS/OND SLW Fx FC/2 m 3 d 31 mo
6 30/M 72 hr MDS FC/1 m 1 d 28 mo
7 44/M TPF 108 hr MDS/OND SLW, OC Fx SNLP 26 mo
8 42/M FSF 40 hr MDS/OND SR, SLW, OC Fx FC/30 cm 3 d 24 mo 9 27/M 54 hr MDS/OND SLW, OC Fx 0.6/color (+) 1 d 21 mo
10 51/F 62 hr MDS/OND SR, OC Fx NLP 19 mo
11 34/M TPF 94 hr MDS/OND ER, LP Fx NLP 15 mo
12 23/M 102 hr MDS/OND SR, OC Fx FC/3 m 6 d 14 mo
13 14/M 40 hr MDS/OND SLW Fx NLP 11 mo
14 24/M FSF 12 hr MDS/OND SLW, OC Fx NLP 8 mo
15 62/M 18 hr MDS/OND SR, OC Fx FC/30 cm 2 d 3 mo
BOF:blowout fracture, ER:ethmoid roof, FC:finger count, FSF:frontal sinus fracture, Fx:fracture, TPF:tripod fracture, LP:lamina papyracea, MDS:megadose steroids, NLP:no light perception, OND:optic nerve decompression, SLW:sphenoid lateral wall, OC:optic canal, SR:sphenoid roof, d:days, hr:hours, mo:months
Fig. 1. Our Current Management Protocol of TON.
138 / J Rhinol 6(2), 1999 ble 1).
Optic canal fractures were confirmed intra-operatively (Fig. 2) in eight out of the 13 patients who underwent surgery. Four out of the eight patients indicated optic ca- nal fracture and two out of the five patients without optic canal fracture indicated improvements in vision after OND. Four out of the seven patients treated within 24 hours after injury and four out of the eight patients treated after more than 24 hours following injury, demonstrated improved vision (Table 3).
DISCUSSION
It is generally agreed that blindness occurring immed- iately at the moment of injury represents a poor prognosis regardless of treatment, while delayed or progressive visual loss indicates a better prognosis.3) However, we excluded patients who were able to perceive light because of possible medicolegal problems after OND. Luxenb- erger et al.8) report that four out of the 10 cases of im- mediate blindness in their series of 15 patients showed improvements in vision after OND. Li et al.9) report a 34.2% mean percentage improvement in their no-light- perception group and 47.1% improvement in the light-
perception-orbetter group among 45 consecutive patients treated surgically. In our series, two out of the 15 patie- nts with immediate blindness demonstrated improved vi- sion after MDS and six out of the remaining 13 patients who were unresponsive to MDS experienced visual im- provement after OND; in total, eight out of 15 patients experienced an overall improvement in vision. A com- parison of the results presented herein and those previ- ously reported in the literature shows a similar rate of recovery. However, it appears that OND may successf- ully treat patients who are found to be unresponsive to MDS, so we followed a policy of reserving the procedure for those patients exclusively.
Most cases of the TON are believed to be related to damage to the intracanalicular segment of the nerve.4) It has been suggested that OND may be particularly ef- fective when the visual loss is associated with optic ca- nal fracture or when a bone fragment impinges on the optic nerve,10) but the incidence of an optic canal fracture in the reported cases of TON is highly variable, ranging
Table 2. Summary of the treatment results Treatment Recovery of vision
Recovery (+) Recovery (-) Total
MDS 2 2
MDS+OND 6 7 13
Total 8 7 15
Table 3. Relationship between the recovery of vision and the timing of treatment or the presence of optic canal fracture
Timing of treatment Recovery of vision
Recovery (+) Recovery (-) Total Tx within 24 hr of injury 4 3 7 Tx after 24 hr of injury 4 4 8 Optic Canal fracture Recovery of vision
Recovery (+) Recovery (-) Total
Fracture(+) 4 4 8
Fracture(-) 2 3 5
Fig. 2. Intra-operative photographs of a patient taken under the operating microscope. Left:A fracture line (arrowheads) running over the optic canal is seen in the upper lateral corner of the left sphenoid sinus. Right:Bony fragment over the optic nerve is removed and the roof of the sphenoid sinus is drilled out. The optic nerve (ON) and the dura (D) of the anterior cranial fossa are uncovered.
Jeon et al:Treatment of Traumatic Optic Neuropathy / 139
from 6% to 92% of cases.4)8) In our series, optic canal fractures were confirmed in eight out of the 13 patients who underwent OND. Four out of the eight patients with optic canal fracture and two out of the five patients wit- hout optic canal fracture demonstrated visual improve- ment after OND. It appears that OND may produce a response even when the visual loss is not associated with optic canal fracture.
The interval between injury and treatment is believed to be an important prognostic factor, and immediate tr- eatment after injury has been stressed.3) However, Spoor et al.6) and Girard et al.7) report finding no relationship between successful recovery and the interval between injury and treatment. In the present study, we evaluated the relationship between visual recovery and the timing of treatment. An immediate start of treatment was def- ined as treatment beginning after the diagnosis of TON, usually within 24 hours after injury in clinical practice.
In our series, four out of the seven patients treated wit- hin 24 hours after injury and four out of the eight patients treated later than 24 hours after injury showed improv- ements in vision. Our results support findings that the recovery rate is not directly related to the interval bet- ween injury and treatment.
Dosing schedules for MDS in the treatment of TON vary widely. Our schedule is based on the recommend- ations made by Anderson et al.4) There is no consensus on the timing of OND in cases found unresponsive to MDS. Anderson et al.4) recommend OND for cases un- responsive to 12 hours of MDS, Li et al.9) recommend 12 to 24 hours, and Luxenberger et al.8) recommend 36 to 48 hours. We looked for visual recovery during a 48- hour course of MDS, based on our decision to reserve OND for patients unresponsive to MDS, and the results of our series imply that the recovery is not directly re- lated to the interval between injury and treatment.
The surgical technique of OND we applied in our st- udy was based on the description by Takahashi et al.11) We drilled with a diamond burr to expose the optic nerve, if there was no optic canal fracture or if the covering bone was thick. We mobilized the septum to achieve enough space for instrumentation in most cases, because Koreans tend to have a relatively narrow nasal cavity. The nerve
sheath was not opened, but covered with autologous se- ptal mucosa. Splitting the optic nerve sheath is a contr- oversial procedure for which there is no study to guide proper patient selection. Intrasheath hematoma, fracture of the optic canal, and impingement on the optic nerve are suggested reasons for splitting the nerve sheath,8) while routine splitting, including annulus of Zinn, has been recommended.9) However, without splitting the op- tic nerve sheath, we achieved visual improvement in six of 13 surgical patients.
CONCLUSION
This study is uncontrolled but suggests that our prot- ocol of MDS and, in cases found unresponsive to MDS, OND may be an effective and valid treatment modality for patients with immediate complete TON, which has been believed to represent a poor prognosis regardless of treatment.
REFERENCES
1) Walsh FB, Hoyt WF. Clinical Neuro-ophthalmology. 3rd ed, Balt- imore, Williams & Wilkins;1969. p.2375-81.
2) Holt GR, Holt JE. Incidence of eye injuries in facial fractures: An analysis of 727 cases. Otolaryngol Head Neck Surg 1983;91:276-9.
3) Lipkin AF, Woodson GE, Miller RH. Visual loss due to orbital fr- acture. Arch Otolaryngol Head Neck Surg 1987;113:81-3.
4) Anderson RL, Panje WR, Gross CE. Optic nerve blindness follo- wing blunt forehead trauma. Am Acad Ophthalmol 1982;89:445-55.
5) Wollin MJ, Levin PJM. Spontaneous visual recovery from traum- atic optic neuropathy after blunt head injury. Am J Ophthalmol 1990;
109:430-5.
6) Spoor TC, Hartel WC, Lensink DB, Wilkinson MJ. Treatment of traumatic optic nerve neuropathy with corticosteroids. Am J Oph- thalmol 1990;110:665-9.
7) Girard BC, Bouzas EA, Lamas G, Soudant J. Visual improvement after transethmoid-sphenoid decompression in optic nerve injuries.
J Clin Neuro-ophthalmol 1992;12(3):142-8.
8) Cook MW, Levin LA, Joseph MP, Pinczower EF. Traumatic optic neuropathy, A meta-analysis. Arch Otolaryngol Head Neck Surg 1996;122:389-92.
9) Luxenberger W, Stammberger H, Jebeles JA, Walch C. Endos-co- pic optic nerve decompression: The Graz experience. Laryngoscope 1998;108:873-82.
10) Li KK, Teknos TN, Lai A, Lauretano AM, Joseph MP. Traumatic optic nerve neuropathy: Result in 45 consecutive surgically treated patients. Otolaryngol Head Neck Surg 1999;120:5-11.
11) Takahashi M, Itoh M, Kaneko M, Ishii J, Yoshida A. Micros-copic intranasal decompression of the optic nerve. Arch Otorhinolaryngol 1989;246:113-6.