수두 포진 감염 후 악화된 시신경척수염 스펙트럼 장애 1례
서울대학교병 어린이병원원 소아청소년과1, 서울대학교병원 어린이병원 소아뇌신경센터2, 분당서울대학교병원 소아청소년과3,
서울대학교 보라매병원 소아청소년과4
고영준1・우승1・김헌민3・임병찬1,2・황희3・채종희1,2・김기중1,2・황용승1,2・최지은4
Case report
This report was presented as a poster at annual meeting of Korean Pediatric Society (2014).
Submitted: 11 May, 2015 Revised: 28 June, 2015 Accepted: 4 July, 2015
Correspondence to Ji-Eun Choi, MD, PhD
Division of Pediatric Neurology, Department of Pe- diatrics, SMG-SNU Boramae Medical Center, Seoul National University College of Medicine, 20, Boramae- ro 5-gil, Dongjak-gu, Seoul 156-707, Korea
Tel: +82-2-840-2376, Fax: +82-2-831-2826 E-mail: [email protected]
J Korean Child Neurol Soc 2015;23(2):67-70 pISSN 1226-6884•eISSN 2383-8973
A Case of Neuromyelitis Optica Spectrum Disorder Aggravated after Varicella Zoster Infection
Neuromyelitis optica (NMO) is a rare demyelinating disease of the central nervous system (CNS) that affects the optic nerves and spinal cord. Although aggressive immunosuppressive treatment is mandatory due to the poor prognosis of NMO, there is always a risk of life-threatening infections. A 4-year-old boy was admitted because of headache and weakness of both lower extremities. Brain and spinal magnetic resonance imaging (MRI) demonstrated diffuse ill-defined lesions with T2 hyperintensity in the lower medulla and whole cervical cord. He improved with intravenous immune-globulin (IVIG) and methylprednisolone pulse therapy.
However, after 2 years, he developed recurrent vomiting and hyperesthesia on his neck and shoulder. Aquaporin-4 antibody (AQP-4 Ab) was positive in his serum and he was diagnosed with NMO spectrum disorder (NMOSD). After 1 year, he developed a generalized vesicular rash and was treated with acyclovir for chickenpox. However, after 2 weeks, he re-developed left ear vesicles with severe headache and hyperes- thesia on his post scalp and upper shoulder without muscle weakness. His brain and spinal MRI revealed extensively increased T2 hyperintensity lesions down through the upper thoracic cord (T6). He again received IVIG and methylprednisolone pulse therapy, followed by oral prednisolone and azathioprine maintenance. We also treated zoster infection with IV acyclovir for 3weeks and chronic famciclovir pro- phylaxis and neurontin for trigeminal neuralgia. His headache and hyperesthesia showed some improvement, but not complete. Here, we present a case of NMOSD aggravated after varicella zoster infection during chronic steroid maintenance.
Key words: Neuromyelitis optica, Varicella zoster
Young Jun Ko, MD
1, Seung Woo, MD
1, Hunmin Kim, MD
3, Byung Chan Lim, MD
1,2, Hee Hwang, MD
3, Jong Hee Chae, MD
1,2, Ki Joong Kim, MD
1,2, Yong Seung Hwang, MD
1,2, Ji-Eun Choi, MD
41
Department of Pediatrics,
2Pediatric Clinical Neuroscience Center, Seoul National University Children’s Hospital, Seoul,
3Department of Pediatrics, Seoul National Univer sity Bundang Hospital, Gyeonggi-do,
4Department of Pediatrics, SMG-SNU Bo ramae Medical Center, Seoul, Korea
Copyright © 2015 by The Korean Child Neurology Society
http://www.cns.or.kr
Introduction
NMO is a rare auto-immune mediated demyelinating disease of CNS that affects the optic nerves and spinal cord1). In 2004, the water channel AQP-4 Ab was turned out to be a disease-specific autoantibody for NMO2,3). That finding of auto Ab to water channel implicated in the pathogenesis of NMO gave insights not only into revising the diagnostic classification of NMO, but into expanding the spectrum of NMO. Therefore, NMOSD includes limited forms of the disease such as recurrent isolated longitudinally extensive transverse myelitis (LETM) or re-
68
Ko YJ, et al. • A Case of NMO Spectrum Disorder Aggravated after Varicella Zoster Infection http://www.cns.or.krcurrent isolated optic neuritis (ON) and atypical cases with brain lesions based on the same pathogenesis4).
The prognosis of NMO and NMOSD is devastating and very difficult to be cured because of severe disabling relapse. Thus, early diagnosis, aggressive treatment and long term prophylaxis are recommended. However, due to the main immunosuppres- sant treatment, there is always a risk of severe infections rather than controlling disease itself.
Here we present a boy with NMOSD aggravated after varicella zoster infection during steroid maintenance therapy.
Case report
A 4-year-old boy was admitted because of headache and weakness of both lower extremities for 2 months. At the time of admission, the patient was alert and well oriented. Papilledema was absent and cranial nerve dysfunction including his visual acuity and extraocular muscles was not observed. There was no objective sensory loss but he had a both lower extremities weakness which was graded as a Medical Research Council (MRC) grade 4. White blood cell (WBC) count was 4,540/uL, hemoglobin was 13.2 g/dL, high sensitivity C-reactive protein (hs-CRP) was 0.04 mg/L. The cerebrospinal fluid (CSF) analysis was normal and bacterial cultures of the spinal fluid and blood were negative. Brain and spinal MRI demonstrated diffuse, ill- defined lesions with T2 hyperintensity in the lower medulla and whole cervical cord (Fig. 1A). He could not walk by himself.
Under the impression of transverse myelitis, we treated him with IVIG (1 g/day) for 2 days and methylprednisolone (20 mg/kg/
day) pulse therapy for 5 days, followed by oral prednisolone for 1 month. His symptom was improved, and image finding after 1 year also showed slight improvement.
After 2 years, he developed recurrent vomiting and hyperes- thesia on his neck and shoulder and showed an increased extent of lesions down through the thoracic cord (T4) in spinal MRI (Fig. 1B). AQP-4 Ab was 8.1 ng/mL in his serum (normal control 0.5-1.4 ng/mL) and he was confirmed to NMOSD. He received treatment with IVIG (400 mg/kg/day for 5 days) and methylpred- nisolone pulse therapy and he became symptom free with no neurologic deficit. After then, he kept oral glucocorticoid main- tenance therapy every other day to prevent relapse without any side effects.
He developed a sudden-onset generalized vesicular rash with- out fever after 1 year of maintenance therapy and was treated with IV acyclovir on the impression of chickenpox. Three days later, his vesicles were crusted and he received oral acyclovir for
2 weeks. However, he abruptly complained of left ear vesicles with severe headache and hyperesthesia on his post scalp and upper shoulder without motor weakness after 2 weeks, sugges- ting zoster relapse. His brain and spinal MRI revealed extensively increased T2 high signal intensity lesions down through the upper thoracic cord (T6) (Fig. 1C). Under the impression of NMOSD relapse, he received again intravenous methylprednisolone pulse therapy and IVIG followed by oral prednisolone. We also treated zoster infection with IV acyclovir for 3 weeks and chronic fam- ciclovir maintenance prophylaxis and neurontin for trigeminal neuralgia. His headache and hyperesthesia showed some im- provement.
Three months after zoster infection, he complained of another attack of right arm weakness and a tingling sensation. Brain MRI
A B
C D
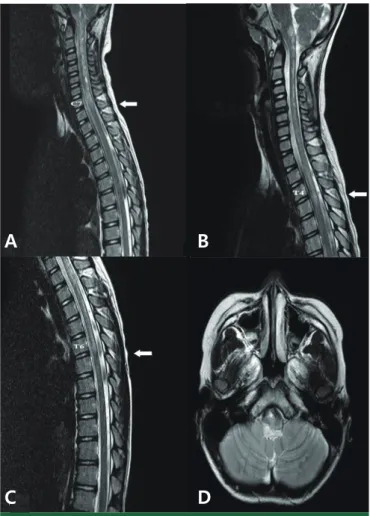
Fig. 1. Spinal magnetic resonance imaging (MRI) showed ill-defined
high signal intensity lesions in the lower medulla and whole cervical
cord (C1-7) on the sagittal view of T2-weighted image at initial admis-
sion (A). There was an increased extent of ill-defined high signal inten-
sity lesions from the medulla to the upper thoracic cord (T4) in follow-
up spinal MRI at diagnosis of Neu romyelitis optica spectrum disorder
(B) and to the upper thoracic cord (T1-6) at 1
strelapse after zoster in-
fection (C). Brain MRI revealed increased extent of high SI lesions on
T2 WI in the medulla (right side dominant) at 2
ndrelapse (D).
J Korean Child Neurol Soc 2015;23(2):67-70
69
http://www.cns.or.krrevealed an increased extent of high SI lesions on T2 WI in the medulla (right side dominant) (Fig. 1D). He received IVIG for 5 days and his motor weakness and paresthesia were improved.
But 3 months later, he complained again right side motor weak- ness and paresthesia. We started azathioprine (1 mg/kg/day) in addition to IVIG therapy. After azathioprine plus steroid mainte- nance and famciclovir prophylaxis, he complained only of an intermittent tingling sensation in both legs at night and showed no further relapse.
Discussion
Longitudinally extensive transverse myelitis is a syndrome showing an inflammatory spinal cord lesion that involves three or more vertebral segments in length. The description of AQP-4 Ab broadens the spectrum of NMO to include the limited forms of the disease and recurrent LETM5). Aquaporin-4 (AQP4) is ex- pressed on the plasma membrane of astrocytes throughout the CNS and binding of AQP-4 Ab is thought to cause complement- dependent cytotoxicity, leading to leukocyte infiltration, cytokine release and blood-brain barrier breakdown6). AQP-4 Ab is de- tected in approximately 50% of patients with recurrent LETM2), and 40% of patients with LETM relapse or develop NMO7). In our case, the patient showed recurrent LETM and AQP-4 Ab was detected at second attack. Therefore, he was diagnosed with NMOSD and treated with immune-suppressive therapy.
Considering the accumulated disabilities of untreated NMO/
NMOSD, early diagnosis and aggressive treatment are now con- sidered standard practice. Acute exacerbation is treated with corticosteroids, typically 1 g of intravenous methylprednisolone for 5 days followed by oral prednisolone (1 mg per kg) for a month, and then a gradual tapering off over a 6-12 months8). However, long term steroid treatment has a risk of side effects (e.g. infection, hypertension, hyperglycemia, and osteoporosis) and especially infection may be a cause of relapse. In a subgroup of NMOSD, preceding viral infections account for 15-25%9,10). Causal agents are cytomegalovirus (CMV), herpes simplex virus (HSV), varicella zoster virus (VZV), mumps and Epstein–Barr virus (EBV), and dengue virus10-12). Para-infectious triggering can be explained by bystander activation8). Bystander activation involves inflammatory reactions that damage AQP-4, triggering an immune cascade leading to the activation of AQP-4 specific B-cells.
In 2013, there was a first case of recurrent LETM with AQP-4 Ab after varicella zoster infection14). However, to our knowledge, there has not yet been a report of NMOSD relapse or aggravation
due to varicella zoster infection.
In summary, we present a boy who was diagnosed with NMOSD aggravated by zoster infection. He showed good response to corticosteroid therapy initially, but he suffered a recurrent relapse and neurologic disability after the outbreak of varicella zoster infection during steroid maintenance. Varicella zoster infection can be an initiating cause of LETM, but it may also be an aggra- vating factor of NMOSD.
Clinicians must be aware that immunosuppressant treatment can be a trigger of neuro-tropic viral infection, and prompt, pro- longed antiviral treatment and long term prophylaxis are suggested.
요약
시각신경척수염은 양측 시신경과 척수를 침범하는 중추신경계의 자가면역성 탈수초 질환이다. 질병 특이적 항체인 AQP-4 항체가 밝 혀지면서 기존의 진단 기준이 바뀌었고, 반복성 광범위 횡단 척수염 혹은 반복성 시신경염과 같이 시각신경 척수염의 범주에 속하는 질 환에 대한 인식이 생겼다. 시각신경 척수염의 치료는 면역억제제 치료 로 스테로이드를 투여하며, 부작용으로 중증 감염이 생길 수 있다. 본 저자들은 면역억제 치료 중에 발생한 수두 감염 이후 시각신경척수염 스펙트럼장애의 악화소견을 보인 1례를 경험하고, 이 증례를 통해 시 각신경척수염 스펙트럼장애 치료뿐만 아니라 치료의 부작용을 감시 하고 예방하는 것의 중요성을 제시하고자 하였다.
References
1) Wingerchuk DM1, Lennon VA, Lucchinetti CF, Pittock SJ, Wein
shenker BG. The spectrum of neuromyelitis optica. Lancet Neurol 2007;6:80515.
2) Lennon VA, Wingerchuk DM, Kryzer TJ, Pittock SJ, Lucchinetti CF, Fujihara K, et al. A serum autoantibody marker of neuromy
elitis optica: distinction from multiple sclerosis. Lancet 2004;364:
210612.
3) Lennon VA, Kryzer TJ, Pittock SJ, Verkman AS, Hinson SR. IgG marker of opticspinal multiple sclerosis binds to the aquaporin
4 water channel J Exp Med 2005;202:4737.
4) Jacob A, Matiello M, Wingerchuk DM, Lucchinetti CF, Pittock SJ, Weinshenker BG. Neuromyelitis optica: changing concepts. J Neuroimmunol 2007;187:12638.
5) Jacob A, McKeon A, Nakashima I, Sato DK, Elsone L, Fujihara K, et al. Current concept of neuromyelitis optica (NMO) and NMO spectrum disorders. J Neurol Neurosurg Psychiatry 2013;84:922
30.
6) Frigeri A, Gropper MA, Umenishi F, Kawashima M, Brown D, Verkman AS. Localization of MIWC and GLIP water channel homologs in neuromuscular, epithelial and glandular tissues. J
70
Ko YJ, et al. • A Case of NMO Spectrum Disorder Aggravated after Varicella Zoster Infection http://www.cns.or.krCell Science 1995b;108:29933002.
7) Weinshenker BG, Wingerchuk DM, Vukusic S, Linbo L, Pittock SJ, Lucchinetti CF, et al. Neuromyelitis optica IgG predicts relapse after longitudinally extensive transverse myelitis. Ann Neurol 2006;59:5669.
8) Sellner J, Hemmer B, Mühlau M. The clinical spectrum and im
munobiology of parainfectious neuromyelitis optica (Devic) syndromes. J Autoimmun 2010;34:3719.
9) Koga M, Takahashi T, Kawai M, Fujihara K, Kanda T. A serological analysis of viral and bacterial infections associated with neuro
myelitis optica. J Neurol Sci 2011;300:1922.
10) Heerlein K, Jarius S, Jacobi C, Rohde S, StorchHagenlocher B,
Wildemann B. Aquaporin4 antibody positive longitudinally extensive transverse myelitis following varicella zoster infection.
J Neurol Sci 2009;276:1846.
11) Tran C, Du Pasquier RA, Cavassini M, GuexCrosier Y, Meuli R, Ciuffreda D, et al. Neuromyelitis optica following CMV primo
infection. J Intern Med 2007;261:5003.
12) Miranda de Sousa A, PuccioniSohler M, Dias Borges A, Fern
andes Adorno L, Papais Alvarenga M, Papais Alvarenga RM. Post
dengue neuromyelitis optica: case report of a Japanesedescen
dent Brazilian child. J Infect Chemother 2006;12:3968.
13) Park JS, Hwang SJ, Shin JH, Kim DS. A recurrent longitudinally extensive transverse myelitis with Aquaporin4(AQP4) antibody after herpes zoster. J Neurol Sci 2013;334:6971.