Reoperative Aortic Root Replacement in Patients with Previous Aortic Root or Aortic Valve Procedures
8
0
0
전체 글
(2)
(3)
(4)
(5)
(6)
(7)
(8)
수치
+2
관련 문서
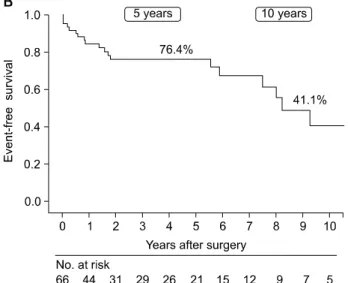
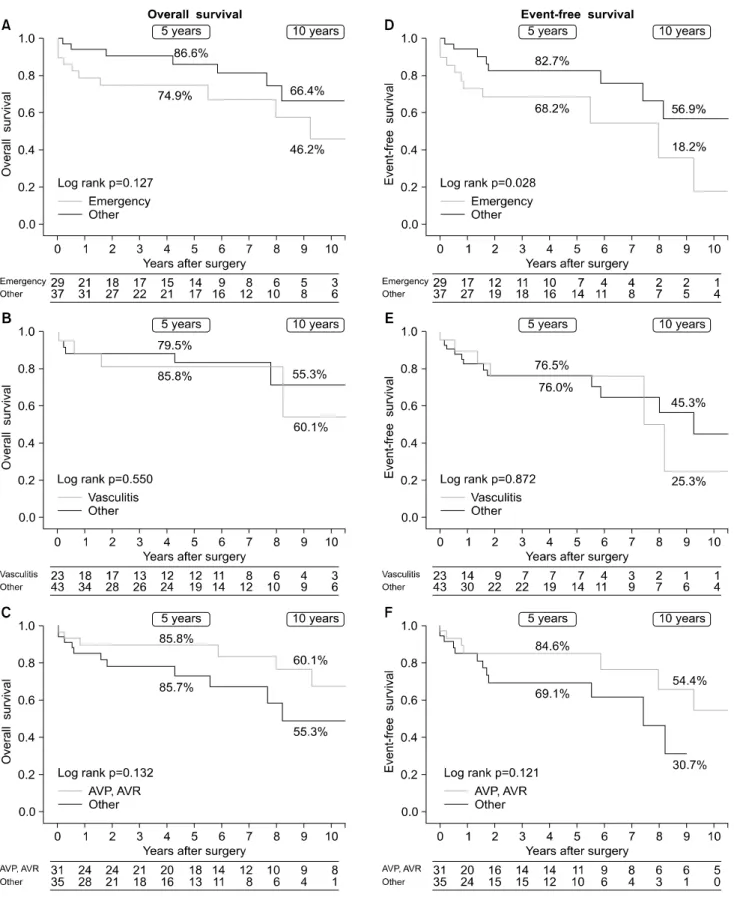
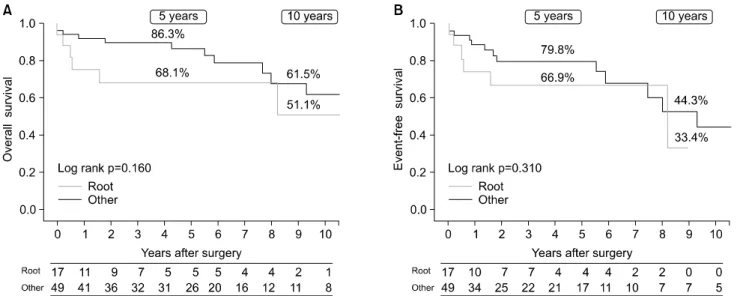
This finding could be caused by diseased myocardium such as LVH, which is more easily influenced by afterload increase associated with aortic stiffness. Kaplan-Meier survival
Second, we removed the previous graft, debrided the abscess, and performed an in situ re-replacement of the ascending aorta, aortic arch, and proximal descending thoracic aorta,
Changes in the degree of paravalvular aortic leakage (p=0.153). Since all patients had functional MR, the extent of MR was expected to de- crease after aortic stenosis
Because aortic or femoral artery cannulation and cross-clamping would have a high risk of stroke owing to severe calcification of the ascending aorta and
Background: This study evaluated the early and long-term outcomes of surgical aortic valve replacement (AVR) in elderly patients in the era of transcatheter
This retrospective study analyzed the outcomes of aortic diameter, including aortic root, ascending aor- ta, and proximal arch diameters, after aortic wrapping during aortic
Of the 143 patients, we excluded 22 patients with prior aortic dissection, 4 patients who underwent ARR under the age of 18 years, 11 patients who had a change in β-blocker or
In this case report, we present a patient with symptomatic severe aortic stenosis and previous mechanical mitral valve replacement who was successfully treated with TAVI using
