144 www.kjtcvs.org
KJTCVSThe Korean Journal of Thoracic and Cardiovascular Surgery
CaseReport
Aortic Valve–Sparing Surgical Treatment of Supravalvar Aortic Stenosis in a 65-Year-Old Adult
Hong Ju Shin, M.D., Ph.D., Jae Seung Shin, M.D., Ph.D.
Department of Thoracic and Cardiovascular Surgery, Korea University Ansan Hospital, Korea University College of Medicine, Ansan, Korea
ARTICLE INFO Received April 3, 2019 Revised January 28, 2020 Accepted February 9, 2020 Corresponding author Jae Seung Shin Tel 82-31-412-5060 Fax 82-31-414-3249 E-mail [email protected] ORCID
https://orcid.org/0000-0001-8147-6665
Supravalvar aortic stenosis (SVAS) is a rare congenital cardiac disease that usually co-occurs with Williams syndrome. In the adult population, a few SVAS cases have been reported in patients affected by homozygous familial hypercholesterolemia. However, because of the rarity of this disease entity, there is no standard surgical treatment for SVAS. Here, we present a case of successful surgical treatment using an autologous excised aortic patch in a 65-year-old patient with SVAS.
Keywords: Supravalvar aortic stenosis, Aortic valve
Copyright©The Korean Society for Thoracic and Cardiovascular Surgery. 2020. All right reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Case report
Supravalvar aortic stenosis (SVAS) is a rare cardiac anom- aly. It usually occurs in combination with Williams syn- drome—with a typical facial appearance and mental retar- dation [1]—but can also present in adult patients affected by homozygous familial hypercholesterolemia (HFH) [2,3].
Because of the rarity of this disease, the surgical technique for SVAS is not standardized and has evolved from a plain patch technique to simple sliding aortoplasty [4,5]. In adult patients with SVAS, conventional surgical treatment is dif- ficult to apply due to reduced flexibility and atherosclerotic changes of the vasculature. We performed autologous ex- cised aortic patch aortoplasty and ascending aorta replace- ment sparing the aortic valve in a 65-year-old adult patient with SVAS who did not have either Williams syndrome or HFH.A 65-year-old female patient with a history of transient ischemic attack. hypertension, dyslipidemia, and paroxys- mal atrial fibrillation had SVAS. She took medication for dyslipidemia, hypertension, and atrial fibrillation. Her blood cholesterol level was 230 mg/dL and no other famil- ial member had dyslipidemia. Preoperative echocardiogra- phy showed SVAS with a peak velocity of 4.5 m/sec and mild aortic regurgitation with an ejection fraction of 65%.
Computed tomography showed severe focal stenosis at the
aortic root with diffuse soft tissue thickening and calcifi- cation with a diameter of 14×10 mm (Fig. 1).
The operative approach was through a median sternoto- my. Cardiopulmonary bypass was instituted with a cannu- la for arterial return in the ascending aorta and a venous single cannula in the right atrium. The aortic cross-clamp- ing point was decided after manual palpation of the area of calcification. Cardiac arrest was achieved using cold ante- grade cardioplegic solution. The aorta was transected sev- eral millimeters distal to the point of stenosis. The calcified ascending aorta was removed to a few millimeters below the ascending aorta cross-clamping site. After a careful in- spection of the stenotic segment of the sinotubular junc- tion, as well as the conditions of the coronary opening and the aortic valve, we meticulously excised the stenotic calci- fied tissue, taking care not to damage other tissues. Even though the intimal defect of the sinus portion appeared se- rious (Fig. 2B), it was not especially remarkable because the aortic wall was thickened. Since the stenotic tissue was close to the coronary opening and aortic valve commis- sure, the procedure was time-consuming. After the remov- al of stenotic tissue, an incision was made in the non-coro- nary sinus of the proximal aorta. Autologous healthy aortic tissue from the previously excised ascending aorta was used for patch aortoplasty. After a saline test to detect pos- sible aortic regurgitation, ascending aorta replacement was
https://doi.org/10.5090/kjtcs.2020.53.3.144 pISSN: 2233-601X eISSN: 2093-6516
Korean J Thorac Cardiovasc Surg. 2020;53(3):144-146
145
Hong Ju Shin and Jae Seung Shin. Aortic Valve–Sparing Surgical Treatment of SVAS in a 65-Year-Old Adult
www.kjtcvs.org
KJTCVS
performed using a 24-mm Gelweave graft (Vascutek, Ren- frewshire, Scotland) (Fig. 2). After surgery, the patient had an uneventful postoperative course with arrhythmic medi- cation and electrocardiogram monitoring. Follow-up echo- cardiography and computed tomography showed decreased SVAS, with a peak velocity of 2.3 m/sec and an increased sinotubular junction diameter of 21×21 mm (Fig. 1B). The pathologic report of the aortic tissue was simply athero- sclerosis with calcification. The patient did not have either HFH or Williams syndrome.
The patient provided written informed consent for the publication of clinical details and images.
Discussion
SVAS is a rare cardiac disease that is often progressive in childhood, and scant data are available on its outcomes in the adult population [6]. In particular, only anecdotal re- ports exist of SVAS in patients older than 60 years [2]. Irre- spective of whether its origin is congenital or acquired, the surgical goal is to enlarge the aortic root and to maintain aortic valve function. Because this patient showed exten- sive calcification inside the aortic root and ascending aor- ta, as well as aortic regurgitation associated with old age, we could not rule out the possibility of performing a Ben-
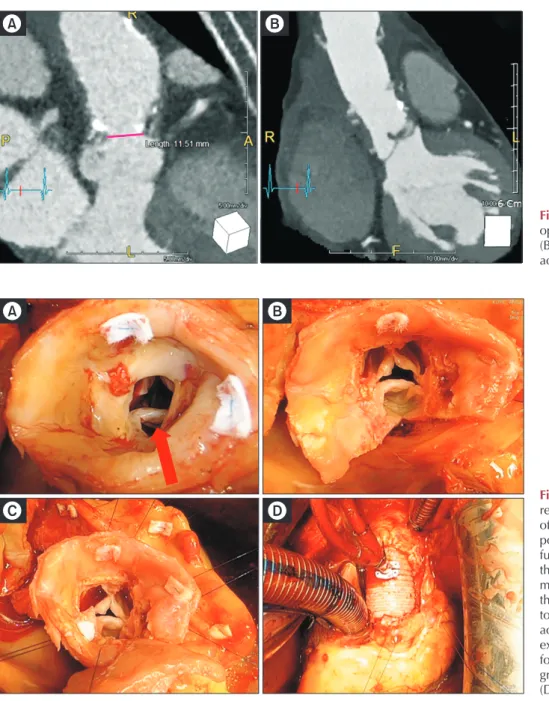
Fig. 1. Preoperative (A) and post- operative computed tomography (B) showed the relief of supravalvar aortic stenosis.
A B
A B
C D
Fig. 2. Supravalvar aortic stenosis repair procedure. After transection of the aorta distal to the narrow point, the calcified tissue was care- fully inspected (A). After removal of the stenotic tissue, an incision was made into the noncoronary sinus of the proximal aorta (B). Patch aor- toplasty using autologous healthy aortic tissue from the previously excised ascending aorta was per- formed (C). Finally, ascending aorta graft interposition was performed (D).
146
https://doi.org/10.5090/kjtcs.2020.53.3.144
www.kjtcvs.org
KJTCVS
tall operation.
However, after careful observation and meticulous re- moval of the calcified lesions, we were able to preserve the coronary opening and aortic valve. Since it appeared that removal of the calcified tissue itself was not sufficient to decrease the pressure gradient, we decided to perform an additional patch aortoplasty using the autologous excised ascending aorta. From our experience, we knew that slid- ing aortoplasty is a good surgical option for handling SVAS [4,5]. However, as this procedure is not suitable for adult patients with stiff aortic tissue, we used a synthetic graft for ascending aorta replacement and performed a modified procedure using patch aortoplasty with autologous aortic tissue. With regard to the choice of patch material, a Da- cron patch is stronger than other tissue types (e.g., pericar- dium) for preventing aneurysm formation. However, be- cause using a Dacron patch would have caused difficulties in handling needle-hole bleeding and resulted in an un- even reconstruction of the aortic wall in terms of its ability to endure aortic pressure, we decided to use autologous healthy aortic tissue that had been removed for the ascend- ing aorta replacement. Using autologous aortic tissue not only avoided the need for foreign material, but also had the advantage of enabling easy handling during the suturing procedure; furthermore, it may prevent future aneurysm formation, which is a possible complication of using peri- cardial tissue. In conclusion, we were able to treat SVAS in an older patient safely using modified patch aortoplasty without aortic valve replacement.
Conflict of interest
No potential conflict of interest relevant to this article was reported.
ORCID
Hong Ju Shin: https://orcid.org/0000-0002-0731-3523 Jae Seung Shin: https://orcid.org/0000-0001-8147-6665
References
1. Williams JC, Barratt-Boyes BG, Lowe JB. Supravalvular aortic ste- nosis. Circulation 1961;24:1311-8.
2. Sato H, Yoshikai M, Ikeda K, Mukae Y. Surgical treatment of valvu- lar and supravalvular aortic stenosis in homozygous familial hyper- cholesterolemia. Gen Thorac Cardiovasc Surg 2016;64:98-100.
3. Morimoto N, Morimoto K, Morimoto Y, et al. Patch annulo-aorto- plasty in an adult patient with congenital supravalvular aortic steno- sis and a small aortic annulus. Gen Thorac Cardiovasc Surg 2011;59:
569-71.
4. Seo D, Shin H, Park J, et al. Modified simple sliding aortoplasty for supravalvar aortic stenosis. Ann Thorac Surg 2007;83:2248-50.
5. Shin HJ, Jhang WK, Park JJ, Goo HW, Seo DM. Modified simple sliding aortoplasty for preserving the sinotubular junction without using foreign material for congenital supravalvar aortic stenosis. Eur J Cardiothorac Surg 2011;40:598-602.
6. Greutmann M, Tobler D, Sharma NC, et al. Cardiac outcomes in adults with supravalvar aortic stenosis. Eur Heart J 2012;33:2442-50.