- 24 -
Serum Eotaxin and Interleukin-13 Level in Patients with Allergic Rhinitis
*Kyung Chul Lee, M.D .
ABSTRACT
Background and Objectives:Eosinophils play a central role in the development of allergic diseases, including asthma, nasal allergy, and atopic dermatitis. Eosinophil migration in vivo is regulated by many cytokines and chemokines. Eotaxin has multifaceted effects on eosinophils and is a key mediator in the development of tissue eosinophilia, and interleukin (IL)- 13 causes surface expression of vascula r cell adhesion molecule-1 (VCAM-1) on endothelial cells and may be important in eosinophilic inflammation in the nasal mucosa. We investigated whether serum eotaxin and IL-13 levels are elevated in allergic rhinitis and drew a correlation with the blood eosinophil counts, serum total IgE, and nasal allergic symptoms in patients with allergic rhinitis. Materials and Methods:Serum eotaxin and IL-13, blood eosinophils, total IgE, and symptom scores were measured in 30 patients with allergic rhinitis, 20 patients with non-allergic rhinitis, and 20 normal control subjects. Results:The serum eotaxin concentration was significantly higher in the allergic rhinitis group than in the non-allergic rhinitis and normal control group (p<0.01, p <0.01). The serum eotaxin concentration was significantly correlated with the peripheral blood eosinophil counts in the allergic rhinitis group. But serum IL-13 concentration in the allergic rhinitis group was not higher than the other groups, and did not correlate with the blood eosinophil counts. Conclusion:Although further investigations will be necessary, evaluation of the serum eotaxin level in allergic rhinitis will provide better understanding of the mechanism involved in allergic tissue eosinophilia.
KEY WORDS:Eosinophils ・Eotaxin・Interleukin-13・A llerg ic rhinitis.
INTRODUCTION
Eosinophils play an important role as inflammatory cells in allergic diseases such as allergic rhinitis, bron- chial asthma, atopic dermatitis etc. Its functions are controlled by numerous cytokines and chemokines.1) Chemokines are substances which carry functions that stimulate white blood cells and chemotaxis, which col- lect white blood cells in a specific area. Chemokines are divided into CXC, CC, C and CX3C according to
the position of the cysteine residue of the protein structure. 40 different groups have been identified and among them CXC usually operates upon neutrophils and CC is known as a chemotactic material of mono- cytes, eosinophils, basophils and lymphocytes.2)3)
Eotaxin, a CC chemotaxin, participates in the mo- bilization of eosinophils and differently from other eosinophil chemokines, eotaxin is a selective eosino- phil chemoattractant, by a specific receptor (CCR-3) that is expressed only in eosinophils.4) Interleukin-13 is attached to the alpha-chain of the IL-4 receptor. It increases the expression of VCAM-1 in the human mucosa microvascular endothelial cell. It is also known to play an important role in eosinophilic inflammatory reaction of the nasal mucosa by increasing the adhe- siveness of eosinophils and endothelial cells.5)
Activated eosinophils are closely related to the edema or hypersensitivity of the nasal mucosa in allergic rhinitis patients. Edema and infiltration of inflamma- tory cells are noticed in the nasal mucosa of allergic rhinitis patients or nas al polyps, and an abundant
*This study was conducted with the financial support of Hyo- seok research fund.
Department of Otolaryngology Head and Neck Surgery, Ka- ngbuk Samsung Hospital, School of Medicine, Sungkyunkwan University, Seoul, Korea
Address correspondences and reprint requests to Kyung-Chul Lee, M.D., Department of Otolaryngology Head and Neck Sur- gery, Kangbuk Samsung Hospital, School of Medicine, Sungky- unkwan University, 108 Pyungdong, Jongroku, Seoul 110-746, Korea
Tel:82-2-2001-2268, Fax:82-2-2001-2273 E-mail:[email protected]
Accepted for publication on July 8, 2002
increase of eosinophils and basophils are especially noticeable.6)
It is well known that eotaxin and IL-13 play an important role in the infiltration of eosinophils in the tissues of allergic nasal polyps or nasal mucosa of allergic rhinitis, however, no further research has been established on the relationship between eosinophils and the function of such substances in the circulation.
Therefore, the expression of eotaxin and IL-13 in the plasma of allergic rhinitis patients has been studied in this present study along with the interrelationship between these substances with the number of eosino- phils, total IgE and the symptoms of patients.
MATERIALS AND METHODS Materials
This study was based on patients that visited our outpatient department from January 1999 through Fe- bruary 2000. There were 30 cases of allergic rhinitis, 20 cases of non-allergic rhinitis and 20 cases of normal control group. The allergic rhinitis group consisted of patients with typical clinical manifestations, positive reaction in the skin prick test, above class 2 positive reaction to house dust tick, house dust, dogs, cats, cockroaches etc., in the MAST® (MAST Immunosys- tem, CA, USA), test and a normal simple PNS x-ray.
The non-allergic rhinitis groups consisted of patients with nasal inflammatory symptoms such as nasal obstruction, rhinorrhea, sneezing and etc., or abnormal physical findings such as nasal mucosa edema, on phy- sical examination, with a negative MAST test result with normal findings in radiological examinations. The normal control groups consisted of people with no nasal inflammatory symptoms, normal physical and radiological findings along with a negative reaction in the skin prick test with no family or allergy history.
Subjects were off all medication such as anti-inflam- matory, antihistamines or local or oral steroids 4 weeks prior to the study.
Methods
A peripheral blood test in all three groups was carried out to measure the concentration of eosinophil, total IgE, eotaxin and IL-13. The measurement of
eosinophil in serum was carried out by collection of peripheral blood in an EDTA-coated tube analyzed through a blood automatic analyzer (ADVIA120, Bayer co, NY, USA). The total-IgE was measured with an immunoradiometric assay kit (Immunotech, Marseille, France). The concentration of intravascular eotaxin and IL-13 was measured by collecting blood in a SST test tube and kept in room temperature for 1 hour for separation of the serum. Serum eotaxin was measured by a human eotaxin kit and serum IL-13 was measured by a human IL-13 kit. Also, to evaluate the allergic symptoms in the patient group, the typical symptoms of allergic rhinitis, such as sneezing, rhinorrhea and nasal obstruction were scored according to the Okuda classification.7) Group analysis of the three groups were compared by one-way ANOVA. The interrelationship between serum eotaxin and intravascular eosinophil, total IgE and allergic rhinitis symptoms were proven by the Pearson rank method. All statistic al studies were carried out by the SPSS statistics program and the statistical deviation was p<0.05.
RESULTS
The average concentration of serum eotaxin in the allergic rhinitis group was 136.38±66.57 pg/ml, 94.80
±53.31 pg/ml in the nonallergic rhinitis group and 68.50±33.14 pg/ml in the normal control group. The allergic rhinitis group showed a significant difference (p<0.01, p<0.01) from the other two groups, however, the non-allergic and normal control group showed no
300
Non-allergic rhinitis Normal control Group
Eotaxin (pg/ml)
200
100
Allergic rhinitis
Fig. 1. Comparison of serum eotaxin levels in patients with all- ergic and non-allergic rhinitis.
significant difference among each other (Fig. 1).
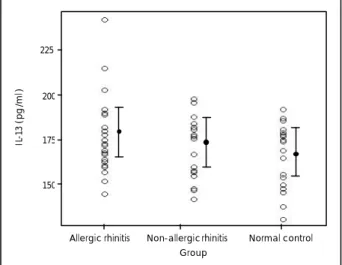
The average concentration of serum IL-13 in the allergic rhinitis group was 178.33±19.58 pg/ml, 172.15
±17.02 pg/ml in the non-allergic rhinitis group and 167.60±27.95 pg/ml in the normal control group.
There was no significant difference noticed among all three groups (Fig. 2).
The average eosinophil in peripheral blood in the allergic rhinitis group was 426.67±229.84/mm3, 335.50
±183.12/mm3 in the non-allergic rhinitis group and 209.00±141.01/mm3 in the normal control group, wh- ich showed a significant difference (p<0.05) between the allergic rhinitis and normal control group. There was no significant difference in the non-allergic rhinitis and allergic rhinitis group (Fig. 3).
The average concentration of serum total IgE in the
allergic rhinitis group was 314.87±292.47 IU/ml, 236.05±212.40 IU/ml in the non-allergic rhinitis group and 149.70±123.58 IU/ml in the normal control group showing a significant difference (p<0.05) between the allergic rhinitis and normal control group. There was no significant difference in the non-allergic rhinitis and allergic rhinitis group (Fig. 4).
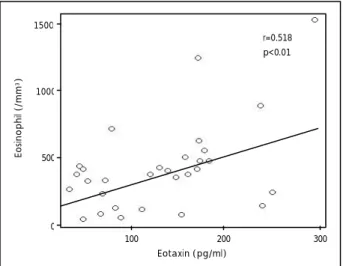
In all subjects, a statistically significant relationship was noticed among serum eotaxin and peripheral blood eosinophil (r=0.630, p<0.01)(Fig. 5). A significant interrelationship was also noticed in the allergic rhi- nitis group (r=0.518, p<0.01)(Fig. 6). However, there was no significant relationship among serum IL-13 and peripheral blood eosinophil.
In all subjects, the concentration of serum eotaxin in the eosinophil increase group was 139.63 pg/ml and
225
Non-allergic rhinitis Normal control Group
IL-13 (pg/ml)
200
150
Allergic rhinitis 175
1500
Non-allergic rhinitis Normal control Eosinophil (/mm3)
1000
0
Allergic rhinitis 500
Fig. 2. Comparison of serum IL-13 levels in patients with allergic and non-allergic rhinitis.
Fig. 3. Comparison of blood eosinophil counts in patients with allergic and non-allergic rhinitis.
1000
Non-allergic rhinitis Normal control
Total IgE (IU/ml) 750
250
Allergic rhinitis 500
0
Fig. 4. Comparison of serum total IgE levels in patients with al- lergic and non-allergic rhinitis.
Fig. 5. Correlation of serum eotaxin levels with blood eosinophil counts (N=70).
r=0.630 p<0.01 1500
200 300
Eotaxin (pg/ml) Eosinophil (/mm3)
1000
0
100 500
76.39 pg/ml in the eosinophil non-increase group, which shows a significant difference among the two groups (p<0.01). Also in the allergic rhinitis group, the serum eotaxin concentration in the eosinophil increase group was 151.42 pg/ml, which was higher than 127.11 pg/ml in the eosinophil non-increase group (p<0.05).
There was no significant interrelationship between serum eotaxin and IL-13 in the allergic rhinitis group.
Also, there was no significance noticed among each symptoms of rhinorrhea, sneezing and nasal obstruction.
DISCUSSION
Allergic rhinitis and bronchial asthma are the typical type I hypersensitivity reaction disorders, which carry the characteristics of infiltration of inflammatory cells of the respiratory mucosa and increase of chemical mediators. Eosinophils are inflammatory cells that in- crease upon allergic diseases and parasite infections.
Eosinophils secrete many protein granules that destroy tissues and they also maintain and strengthen localized allergic inflammatory reactions by secreting various kinds of cytokines, lipid metabolites and enzymes .8)9)
It has come to knowledge that CD4+ T-helper cells and increase of IL-5, adhesion molecules such as VCAM-1 and ICAM-1, and chemotactic agents such as RANTES and eotaxin participate in the increase and activate tissue eosinophilia that contain allergic inflam- matory reactions.
Eotaxin is an eosinophil chemoattractant chemotac- tic agent that is secreted by epithelial and endothelial
cells and eosinophils. Eotaxin has a huge effect on eosinophils and show a synergistic effect by IL-3, IL-4, IL-5, IFNγand TNF-α in allergic and non-allergic reactions.10) Also, eotaxin helps the increase of ex- pression of adhesion molecules in microvascular endothelial cells which help localized infiltration of eosinophils in the nasal mucosa and accelerate the formation and differentiation of bone marrow stem cells in the bone marrow. This induces fast secretion of eosinophils and its progenitors.11) Also, the secreted eotaxin acts on the eosinophils through an autoreaction mechanism where the infiltration of eosinophils in many allergic diseases can induce the infiltration of eosinophils to a greater extent.
IL-13 has similar biological activities and a 30%
homology to IL-4.12) IL-13 also induces IgE isotype switch, stimulates the formation of B cells in allergic reactions and derives adhesion molecules such as VCAM-1 that help the selective accumulation of eo- sinophils and lymphocytes.13)14) IL-13, along with TNF-α in the fibroblast of the nasal mucosa, plays an important role in eosinophilic inflammatory reactions by increasing the expression of eotaxin in an ascending manner.1)
Increase of eosinophils or increased expression of eotaxin in the nasal mucosa of allergic rhinitis patients or allergic nasal polyps is being reported and it has come to knowledge that eotaxin and IL-13 play an important role in the infiltration and activation of eosinophils in such tissues.15-17) The mechanism of such tissue eosinophilia can be explained by either increased migration of eosinophils to the target organs or elongated survival ability of eosinophils of the tissues.
For the accumulation of eosinophils in the blood, they must first be carried and captured by substances such as VCAM-1 and VLA-4 and then activated by chemotactic materials. As the bonding nature becomes stronger the escape mechanism occurs and with the help of CD31 eosinophils begin to migrate into the tissue.18) It is also regarded that not only does the nasal mucosa play an important role for the migration of eosinophils to the nasal mucosa tissue of allergic rhinitis, the function of chemotactic materials that specifically effect eosinophils in the blood are also necessary for this mechanism.
In this study, a significant increase of serum eotaxin was indicated in the allergic rhinitis group compared to
r=0.518 p<0.01 1500
200 300
Eotaxin (pg/ml) Eosinophil (/mm3)
1000
0
100 500
Fig. 6. Correlation of serum eotaxin levels with blood eosinophil counts in patients with allergic rhinitis (N=30).
the other two groups. Also, in all subject patients of this study, serum eotaxin and eosinophils in the peri- pheral blood showed a statistically significant interre- lationship with one another, which was also shown in the allergic rhinitis group. Also, in all subject patients of this study and the allergic rhinitis group, the serum eotaxin in the eosinophils increase group showed a significant difference compared to the serum eotaxin in the eosinophil non-increase group. In this study, we were not able to explain the relationship between the increase of eosinophils in the nasal mucosa by simply studying the interrelationship between the increase of serum eotaxin and eosinophils in allergic rhinitis. Va - rious factors along with adhesion molecules participate in tissue eosinophilia however, a more accurate evalua- tion through a test to observe whether or not there is an eosinophil increase will be necessary. It is regarded that through the relationship of the increase of serum eotaxin and eosinophils can assist in understanding the etiology of tissue eosinophilia.
In this study, the average concentration of serum IL- 13 showed no significant difference among all three groups. There was also no significant relationship with eosinophils in the peripheral blood. This leads to the conception that IL-13 increases the adhesive nature of endothelial cells by increasing the expression of VC- AM-1 in the tunica propria of tissues that contain allergic inflammatory reactions. Thereafter, this activates the removal of eosinophils from the endothelial cells in the tunica propria, which increases the migration of eosinophils that eventually help in the selective accumulation of eosinophils in the tissue. However, because the concentration of IL-13 in the blood is very low, the influence of IL-13 can only be minor.19) Therefore, it is inferred that it would be difficult to surmise the relationship with eosinophils by simply measuring serum IL-13 in allergic rhinitis patients.
In this study, eosinophils in the peripheral blood showed a significant difference among the allergic rhi- nitis and normal control group. There was no significant difference with the non-allergic rhinitis group. Mygind et al.,20) reported that the number of eosinophils in allergic diseases speaks for the size of the shock organ and the absolute value has meaning. Only in 15% of all allergic rhinitis patients showed an increase of eosinophils in the peripheral blood and there was no relatively notable increase of eosinophils than in aller-
gic dermatitis and asthma patients.
The allergic rhinitis group and normal control group showed a significant difference in serum total IgE, however, there was no significant difference with the non-allergic rhinitis group. Miyamodo et al.,21) reported that serum IgE does not show a significant increase in allergic diseases. Min et al.,22) reported that only a minor group showed an increase in eosinophil which revealed diagnostic meaning in patients only under the age of 29 but this also showed no statistical significance with serum eosinophils.
The serum eotaxin and IL-13 concentration and comparison of symptom scoring showed no interrela- tionship with one another, however, various factors participate in the manifestation of symptoms in allergic rhinitis and when considering the fact that there may be a vast difference among each individual in the ma- nifestation of symptoms, a simple comparison carried out of patient symptoms may have limitations.
CONCLUSION
Tissue infiltration of eosinophils and eotaxin in the serum of allergic rhinitis patients has been signifi- cantly detected and they also showed a significant interrelationship with peripheral blood eosinophil. Ev- enthough it is not possible in this study to presume eosinophil infiltration of the tissue and its activity, it is inferred that the measurement of eotaxin in the serum of allergic rhinitis patients may assist in the research of the etiology of tissue eosinophilia.
REFERENCES
1) Terada N, Hamano N, Nomura T, Numata T, Hirai K, Nakajima T, et al. Interleukin -13 and tumour necrosis factor-α synergistically induce eotaxin production in human nasal fibroblasts. Clinical and Experimental Allergy 1999;30:348-55.
2) Choe H, Farzan M, Sun Y, Sullivan N, Rollins S, Ponath PD, et al.
The β-chemokine receptors CCR3 and CCR5 facilitate infection by prim ary HIV-1 isolates. Cell 1996;85:1135-48.
3) Baggiolini M, Dewald B, Moser B. Interleukin -8 and related che- motactic cytokines-CXC and CC chemokines. Adv Immunol 1994;
55:97-179.
4) Ponath PD, Shixin Q, Ringler DJ, Lewis IC, Wang J, Kassam N, et al. Cloning of the human eosinophil chemoattractant, Eotaxin. J Clin Invest 1996;97:604-12.
5) Bochner BS, Klunk DA, Sterbinsky SA, Coffman RL. Interleukin 13 selectively induces vascular cell adhesion molecule-1 expression in human endothelial cells. J Immunol 1995;154:799-803.
6) Nobuhisa T, Akiyoshi K, Kiyoshi T. Biochemical properties of eo- sinophils and their preferential accumulation mechanism in nasal
allergy. J Allergy Clin Immunol 1994;94:629-42.
7) Okuda M, Ohtsuka H, Sakaguchi K, Watase T. Nasal histamine sensitivity in allergic rhinitis. Ann Allergy 1983;51:51-5.
8) Gleich GJ. The eosinophil and bronchial asthma: Current underst - anding. J Allergy Clin Immunol 1990;85:422-36.
9) Motojima S, Frigas E, Loegering DA, Gleich GJ. Toxicity of eosi- nophil cationic proteins for guinea pig tracheal epithelium in vitro.
Am Rev Respir Dis 1989;139:801-5.
10) Garcia-Zepeda EA, Rothenverg ME, Ownbey RT, Celestin J, Leder P, Luster AD. Human eotaxin is a specific chemoattractant for eosinophil cells and provides a new mechanism to explain tissue eosinophilia. Nature Medicine 1996;2:449-56.
11) Palframan RT, Collins PD, Williams TJ, Rankin SM. Eotaxin indu- ces a rapid release of eosinophils and their progenitors from the bone marrow. Blood 1998;91:2240-8.
12) Defrance T, Carayon P, Billian G, Guillemont JC, Minty A, Caput D. Interleukin 13 is a B cell stimulating factor. J Exp Med 1994;
79:135-43.
13) Borish L, Rosenwasser LJ. Update on cytokines. J Allergy Clin Im- munol 1996;97:719-34.
14) Jirapongsananuruk O, Leung DYM. Clinical application of cytoki- nes: New directions in the therapy of atopic diseases. Ann allergy Asthma Immunol 1997;79:5-20.
15) Hanazawa T, Antuni JD, Kharitonov SA, Barnes PJ. Intranasal ad-
ministration of eotaxin increases nasal eosinophils and nitric oxide in patients with allergic rhinitis. J Allergy Clin Immunol 1999;105:
58-64.
16) Shin SH, Heo WW, Ye MK, Park JY, Cho CH, Sohn JH, et al.
Expression of eotaxin and RANTES mRNA in nasal polyps and its effect on eosionphils. Korean J Otolaryngol 2000;43:724-30.
17) Hwang CS, Park H, Park SH, Lee JH, Hong YH, Kim H, et al.
Regulation of CC chemokines in TDI-induced nasal hyperreactive rat : Expression of RANTES and eotaxin mRNA examined using competitive PCR. Korean J Otolaryngol 1999;42:985-92.
18) Carlos TM, Harlan JM. Leukocyte-endothelial adhesion molecules.
Blood 1994;84:2068-101.
19) Terada N, Hamano N, Hohki G, Ikeda T, Sai M, Yamashita T, et al.
The potential role of interleukin-13 in eosinophilic inflammation in nasal mucosa. Allergy 1998;53:690-7.
20) Mygind N. Nasal allergy, 2nd ed. Oxford, blackwell Scientific pu- blicaton;1979.
21) Miyamodo Y, Oshima S, Ishiazkz T, Sato S. Allergenic identity bet- ween the common floor mite (Dermatophagoiedes Farinae Hughes) and house dust as a causative antigen in bronchial asthma. J All- ergy 1968;42:14-28.
22) Min YG, Koh JW, Park HS, Shin KC. Diagnostic significance of serum IgE level in perennial allergic rhinitis. Korean J Otolaryngol 1981;21:172-6.