- 29 -
Skin Prick Testing of Patients with Allergic Rhinitis and/
or Asthma: a Study in Catholic Medical Center, Korea
Ji-Hyeon Shin, MD, Byung-Guk Kim, MD, Jin-Hee Cho, MD, Sung Won Kim, MD, Beom Jun Lee, MD, Ye Won Kim, MD and Soo Whan Kim, MD
Department of Otolaryngology-Head and Neck Surgery, College of Medicine, The Catholic University of Korea, Seoul, Korea
ABSTRACT
Background and Objectives: Allergic rhinitis is closely related to asthma. The skin prick test is an essential diagnostic tool for allergic disease. We evaluated differences in skin sensitization patterns between groups of pa- tients with allergic rhinitis or asthma, or allergic rhinitis with asthma, in Korea. Materials and Methods : From 2000 to 2009, patients with positive results from skin prick testing were divided into three groups: allergic rhinitis (AR), allergic asthma (AS), and allergic rhinitis with allergic asthma (AR+AS). We analyzed demographic data, rhinitis and asthma symptoms, and sensitization patterns. Results : The most common aeroallergen was the house dust mite. The age distributions of the three disease groups differed significantly. Sensitization number, sensiti- zation index, and atopy index were all significantly higher among the AR+AS group than among the AR or AS groups. Conclusion: Patients with allergic rhinitis with high numbers of skin sensitizations or intensive positivi- ties should be considered to have concomitant asthma or to be at high risk for asthma development.
KEY WORDS : Allergic Rhinitis · Asthma · Skin Prick Test.
INTRODUCTION
Allergic rhinitis is a symptomatic disorder of the nose induced after allergen exposure by an IgE-mediated in- flammation and is characterized by one or more symp- toms including sneezing, itching, nasal congestion, and rhinorrhea.
1)The reported prevalence of allergic rhinitis in epidemiologic studies ranges from 10% to 25% and rates have increased in developed countries over recent decades.
1) 2)Asthma and allergic rhinitis have similar underlying pathogenesis and immunologic mechanisms, and recent studies have identified both disorders as manifestations of the chronic inflammatory respiratory syndrome of the common airways.
3) 4)Of all patients with asthma, 30–90%
have concomitant rhinitis, and 20–50% of patients with allergic rhinitis also have asthma.
5) 6)Some studies have demonstrated that allergic rhinitis is a risk factor for asth-
ma, regardless of the presence of allergy.
7)In clinical practice, the skin prick test (SPT) has been extensively used to assess sensitization to allergens. The test is useful for confirming a diagnosis of allergic rhinitis, allergic conjunctivitis, or asthma, and for demonstrating immediate hypersensitivity.
8)Skin sensitization patterns against allergens differ significantly by age, gender, envi- ronmental factors, and the presence of respiratory diseases such as allergic rhinitis and asthma. Especially for the al- lergic rhinitis and asthma, some authors have suggested that an increasing number of sensitizations to inhalant al- lergens may be associated with the development of aller- gic rhinitis or asthma.
9)Other authors, however, have not found any differences between patients with rhinitis and asthma in terms of number of sensitizations or the size of wheals.
21)Little is known about the relationship between skin test reactivity to inhalant allergens and allergic rhini- tis or asthma in Korean populations.
This study evaluated differences in skin sensitization patterns between groups of patients with allergic rhinitis or asthma or allergic rhinitis with asthma.
MATERIALS AND METHODS
The study population consisted of 2015 patients who Address correspondence and reprint requests to Soo Whan Kim, MD,
Department of Otolaryngology-Head and Neck Surgery, College of Med- icine, The Catholic University of Korea, Seoul St. Mary`s Hospital, #505 Banpodong, Seochogu, Seoul 137-701, Korea
Tel: +82-2-2258-6214, Fax: +82-2-595-1354 E-mail: [email protected]
Received for publication on November 2, 2011
Accepted for publicatoin on April 5, 2012
underwent SPT in Seoul at St. Mary’s Hospital at the Catholic University of Korea College of Medicine be- tween 2000 and 2009. The patients were referred to oto- rhinolaryngologist or pulmonologist and performed SPT to evaluate the allergic conditions. The inclusion criteria were the followings: (1) Age between 5 and 87, (2) pres- ence of rhinitis symptoms or asthma symptoms, apart from a viral infection, for a period of more than 2 weeks in the last year, (3) positive skin test for the tested aeroallergens (4) positive metacholine challenge test in the patients with asthma symptoms. We excluded any patients who had a negative skin prick test for the tested aeroallergens; we also excluded any patients with nasal or upper airway in- fections or severe skin disorders, or who had used medica- tion that could affect results. We retrospectively reviewed their medical records, including demographic data, the presence or rhinitis or asthma symptoms, and the sensi- tization patterns.
Patients who exhibited a positive result to a SPT were divided into three groups: allergic rhinitis (AR), allergic asthma (AS), and allergic rhinitis with allergic asthma (AR+AS). The clinical diagnosis of AR was confirmed by positive skin test results and the presence of one or more of the following rhinitis symptoms: watery rhinor- rhea, nasal obstruction, or sneezing. A positive diagnosis of allergic asthma was made when the patient had asthma symptoms and exhibited at least a 20% decrease in forced expiratory volume in 1 second (FEV1) after inhaling 25 mg/mL metacholine.
To analyze sensitization patterns in patients with al- lergic rhinitis and/or asthma by age group, subjects were divided into seven age categories: 5–14, 15–24, 25–34, 35–44, 45–54, 55–64, or 65 years or older.
The SPT (Hollister-Stier, Laboratories, USA) included 53 common aeroallergens, including mite, pollen, mold, animal dander. Histamine phosphate at 10 mg/mL and phosphate-buffered saline were used as positive and nega- tive controls, respectively. A SPT was considered positive when the minimal allergen wheal diameter was the same size or larger than that caused by a histamine, or was 3 mm or larger, or the largest wheal + perpendicular diameter/2 was 3 mm or larger, or the skin index (allergen wheal di- ameter/histamine wheal size) was greater than 0.6.
Demographic data, rhinitis, and asthma symptoms were collected for all subjects from medical records. Common allergens, number of sensitizations, sensitization index (the sum of diameters of positive skin test reactions), and atopy index (sensitization index/number of sensitization) were recorded from the results of SPTs to analyze differ- ences in skin sensitization patterns by disease and age groups. To measure sensitization index and atopy index, we used the methodology introduced by Valero et al.
22)This study was approved by Catholic Medical Center In- stitutional Review Board.
STATISTICAL ANALYSIS
Statistical analyses were performed using the SPSS pro- gram for Windows version 15.0 (Statistical Package for the Social Sciences, Inc., Chicago, IL). For all analyses, a p value of < 0.05 was accepted as significant. Differ- ences in sensitization rates between the variables were determined using chi-square tests and one-way ANOVA test (Scheffe’s test).
RESULTS
Subject characteristics
Of the 2015 patients, 871 patients had at least one posi- tive skin test. In total, 368 (42.3%) patients were classi- fied into the AR group, 323 (37.1%) patients into the AS group, and 180 (20.6%) patients into the AR+AS group.
Subjects had a mean age of 37.4 years (range: 5–87 years) and 434 patients (49.8%) were male. The numbers of pa- tients according to the age groups were as follows: 5–14;
54, 15–24; 218, 25–34; 177, 35–44; 130, 45–54; 126, 55–64; 112, and 65 years or older; 54. The mean age of subjects differed significantly between the disease groups (p < 0.05, one-way ANOVA test) (Fig. 1). About 90%
of subjects aged 5–25 years were classified into the AR group, and about half of subjects over the age of 55 were classified into the AS group.
Common allergens
Among the total study population, sensitization was most common for D. farina (56.4%), followed by D.
pteronyssinus (46.3%). Subjects in the AR+AS group had significantly higher positive rates to D. farina and D.
pteronyssinus than subjects in the AR or AS groups. Der- matophagoides farina was the most common allergen in all age groups.
Sensitization patterns among the various disease groups
Most subjects in all three groups exhibited multiple sen- sitizations during SPTs and a significantly greater number of patients in the AR+AS group were simultaneously sensi- tized to more than five allergens compared to subjects in the AR and AS groups (p < 0.001, chi-square test) (Fig. 2).
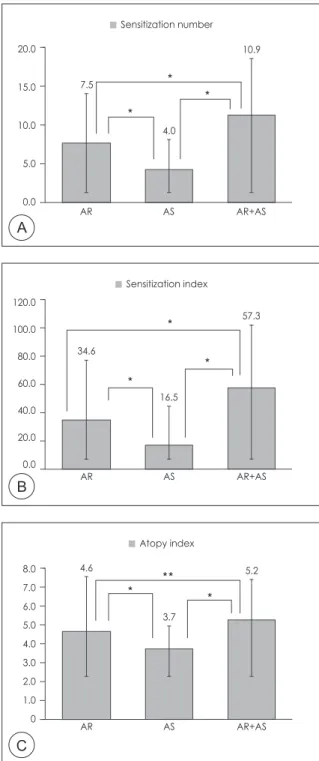
Subjects in the AR+AS group had a significantly great-
er mean sensitization number (10.9) than subjects in the
AR and AS groups (7.5 and 4.0, respectively) (p < 0.01, chi-square test). Subjects in the AR+AS group also had a significantly higher mean sensitization index (57.4) than subjects in the AR and AS groups (34.6 and 16.5, respec- tively) (p < 0.01, chi-square test). The AR+AS group had a significantly higher mean atopy index (5.2) than the AR (4.6) (p <0.05, chi-square test) and AS group (3.7) (p <
0.001, chi-square test). Patients in the AR group had sig- nificantly greater sensitization number, sensitization in- dex, and atopy index compared to the AS group (p < 0.01, chi-square test) (Fig. 3).
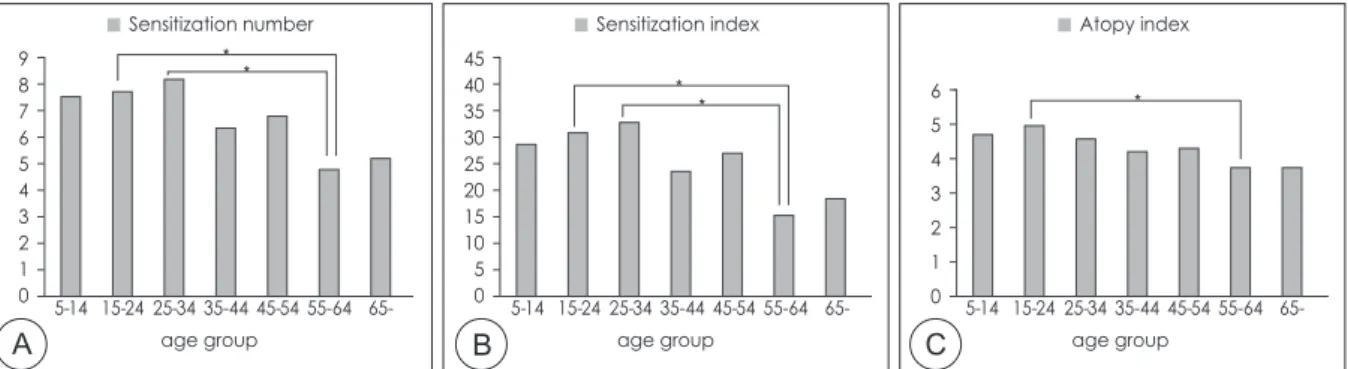
Sensitization patterns by various age groups Figure 4 presents the mean sensitization number, mean sensitization index, and mean atopy index by the various disease groups. Mean sensitization number and mean sen- sitization index were significantly higher in the 15–24- and 25–34-year-old age groups than in the 55–64-year-old group (p < 0.01, chi-square test).
The mean atopy index was significantly higher in the
15–24-year-old age group than in the 55–64-year-old group (p < 0.01, chi-square test).
Sensitization patterns by various allergen groups Figure 5 presents the distribution of sensitizations to al- lergens among patients in the three age groups by strati-
Fig. 1. The mean age of patients in each disease group.
* : P < 0.05.
Fig. 2. The number of sensitized allergens by disease group.
a P < 0.01, AR vs. AS; b P < 0.001, AS vs. AR+AS; c P < 0.001, AS vs.
AR+AS. (AR: allergic rhinitis, AS: allergic asthma)
Fig. 3. Sensitization patterns by disease group: (A) Sensitization number, (B) Sensitization index, (C) Atopy index. * : P < 0.01, **:
P < 0.05
AR AS AR+AS
number of allergen
percentage of sensitization
Age
AR AS AR+AS
28.3
44.9 39.0
70.0 60.0 50.0 40.0 30.0 20.0 10.0 0.0
90 80 70 60 50 40 30 20 10 0
c
a
b
2 3 4
1 ≥5
B
Sensitization index
34.6
16.5
57.3 120.0
100.0 80.0 60.0 40.0 20.0 0.0
AR AS AR+AS
A
AR AS AR+AS Sensitization number
7.5
4.0 20.0 10.9
15.0 10.0 5.0 0.0
C
AR AS AR+AS
Atopy index 4.6
3.7 8.0 5.2
7.0 6.0 5.0 4.0 3.0 2.0 1.0 0
fication. Sensitization to mold was significantly higher in patients with the AR+AS group than those with the AR group for all age groups (p < 0.01, one-way ANOVA test).
Subjects in the AR group had higher sensitization rates to pollens than to other allergens.
DISCUSSION
Asthma and rhinitis are often comorbid conditions, and the overall characteristics of the diseases and treatment options for the disorders are similar.
3)In 1997, Gross- man proposed the theory of “one airway, one disease” and demonstrated that leukotrienes act as potent inflammatory mediators in the pathophysiologic state of inflammation in both airways.
4)Recently, leukotriene receptor antagonists have been applied in important therapeutic advances with potential clinical utility in both asthma and allergic rhini- tis.
4)Several studies have demonstrated that patients with perennial allergic rhinitis are at increased risk for develop- ing asthma.
7)Our data revealed that the prevalence of comorbid- ity between allergic rhinitis and asthma in the AR+AS group (20.6%) fell within previously reported ranges (18–
40%).
10)However, Navarro et al. also found a high preva- lence of comorbidity (89.5%) of allergic rhinitis among patients with asthma.
11)We observed significant differences in age distribution among the three disease groups. The mean age was high-
est in the AS group, followed by the AR+AS group and then the AR group. This relationship confirms the findings of a previous survey, which reported that the prevalence of asthma among patients with allergic rhinitis was not correlated with age until 50 years, and only increased in older age groups.
7)Many other studies have demonstrated the late development of asthma among patients who only exhibited allergic rhinitis when they were younger.
3) 10)Many patients with allergic rhinitis without a clinical history exhibit lower airway hyperreactivity, and the num- ber of their bronchial inflammatory cells increase.
12)The presence of bronchial hyperreactivity has been suggested as an intermediate step in the transition from allergic rhin- itis alone to the development of clinical asthma.
13)Based on our data, D. farina (56.4%) was the most prevalent allergen and dust mite (DF or DP) was signifi- cantly associated with allergic rhinitis and asthma comor- bidity. Multivariate analyses revealed that sensitization to mold was associated with allergic rhinitis and asthma comorbidity.
The most common aeroallergen in Korea is the house dust mite, which is abundant in an environment with high humidity and temperatures.
14)The indoor environment in Korea is particularly suitable for the dust mite, in contrast to Nordic countries, which reportedly have a low inci- dence of house dust mite allergy due to the cold and dry weather in these regions.
15)Most house dust mite allergic patients are co-sensitized to DP and DF.
16)Fig. 5. Sensitization patterns by different groups of aller- gens. : (A) Mold, (B) Pollen
a P<0.01, AR vs. AS;
b P<0.001, AR vs. AR+AS;
c P<0.001, AS vs. AR+AS.
(AR: allergic rhinitis, AS: al- lergic asthma)
Fig. 4. Sensitization patterns by age group: (A) Sensitization number, (B) Sensitization index, (C) Atopy index. *: P<0.01.
A
A
B
B C
Sensitization number
age group age group age group
5-14 15-24 25-34 35-44 45-54 55-64 65- 5-14 15-24 25-34 35-44 45-54 55-64 65- 5-14 15-24 25-34 35-44 45-54 55-64 65- 9
8 7 6 5 4 3 2 1 0
Sensitization index 45
40 35 30 25 20 15 10 5 0
Atopy index
6 5 4 3 2 1 0
age group age group
5-14 15-24 25-34 35-44 45-54 55-64
5-14 15-24 25-34 35-44 45-54 55-64 65- 65-
AR AS AR+AS AR AS AR+AS
a a
a
c c c
b
a a a
b b b
c c
c 10090
80 7060 5040 3020 100
100 90 80 70 60 50 40 30 20 10
percentage of sensitization percentage of sensitization 0