24
서 론
복강경 수술은 외과 영역에 도입된 후 진단과 치료 영역 에 있어서 새로운 paradigm을 제시하고 있다. 복강경 위 수 술은 소화성 궤양(1)과 같은 양성 질환에서부터 간질성 종 양(2)과 위암 등(3-19)의 악성 질환에까지 적용이 확대되고 있는 추세이다. 그러나 위암에서 복강경 위 수술은 기술적 인 면과 종양학적 면에서 아직 논란의 여지가 있다. Uyama 등(3)은 위암 환자에서 위 주위 림프절을 포함한 광범위 림 프절 절제가 복강경으로 가능하다고 하였으나 여전히 개복 술에 비해 복강경 위암 수술은 시간이 많이 소요되고 기술 적으로 어렵다는 인식이 크며 최근 복강경 수술을 위한 이 산화탄소를 이용한 기복(pneumoperitoneum)이 동물 실험에 서 종양학적으로 단점이 있다는 연구들이 발표되었다.
(20-22)
최근 많은 연구자들이 위암 환자의 복강경 수술에 대하 여 발표하였으나(4-8) 이런 연구들은 복강경 위암 수술 자
조기 위암의 복강경 보조하 및 개복 위아전 절제술의 비교
동아대학교 의과대학 외과학교실, 1분당서울대학교병원 외과학교실
김민찬․이성근․정일권․정갑중․김형호1
Comparison of Laparoscopy-Assisted by Con- ventional Open Distal Gastrectomy and Extra- perigastric Lymph Node Dissection in Early Gastric Cancer
Min-Chan Kim, M.D., Sung-Gun Lee, M.D., Il Kwon Jung, M.D., Ghap-Joong Jung, M.D. and Hyung Ho Kim, M.D.1 Purpose: A laparoscopy-assisted gastrectomy with lymph node dissection for gastric cancer is considered technically more complicated than the open method. To evaluate the short-term surgical validity, the surgical outcome of the laparoscopy-assisted distal gastrectomy (LADG) with extra- perigastric lymph node dissection was compared with that of the conventional open distal gastrectomy (CODG) in patients with early gastric cancer.
Methods: One hundred and forty-seven patients with early gastric cancer received a radical distal gastrectomy during 2002 and 2003, where a LADG was performed on 71 patients. The clinicopathological characteristics, postoperative outcomes and courses, and the postoperative morbidities and mortalities were compared between the two groups.
Data were retrieved from the stomach cancer database at Dong-A University Medical center.
Results: Baseline characteristics, including gender, age, body mass index (BMI), American Society of Anesthesiology (ASA) class, tumor size, T stage, and lymph node metas- tasis, were similar between the two groups. No significant differences were found between these groups in terms of the number of retrieved lymph nodes with respect to D1+
(D1+no. 7) and D1+β (D1+no. 7, 8a, and 9) lympha- denectomies. In the LADG group, the wound size was smaller (P<0.0001), but the operation time was longer (P=0.0001) than in the CODG group. The perioperative recovery was faster in the LADG than in the CODG group, as reflected by the shorter hospital stay (P=0.0176) and
less additional analgesics (P=0.0370). The serum albumin level in the LADG was higher (P=0.0002) on day 7 than that in the CODG group, and the leukocyte count in the LADG lower (P=0.0445) on day 1 than that in the CODG gruop. There were no significant differences in the post- operative morbidities and mortalities between the two groups.
Conclusions: Our data confirmed that a LADG with an extraperigastric (no. 7, 8, and 9) lymph node dissection was a feasible and acceptable surgical technique for early gastric cancer. From a surgical point of view, a LADG with an extraperigastric lymph node dissection is suggested to be a preferred surgical option for patients with early gastric cancer. Its oncological validity awaits larger and prospective multicenterd trials. (J Korean Surg Soc 2005;68:24-29) Key Words: Laparoscopic gastrectomy, Lymph node dis-
section, Gastric cancer
중심 단어: 복강경 위 절제술, 림프절 절제술, 위암 ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Department of Surgery, Dong-A University College of Medi- cine, Busan, 1Seoul National University Bundang Hospital, Seongnam, Korea
책임저자:김형호, 경기도 성남시 분당구 구미동 300 ꂕ 140-757, 분당 서울대학교병원 외과 Tel: 031-787-7095, Fax: 031-787-4055 E-mail:[email protected]
접수일:2004년 8월 5일, 게재승인일:2004년 9월 9일
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 체의 기술적인 부분에 초점을 맞춘 것이 대부분이고 복강
경 보조하 원위부 위절제술(Laparoscopic Assisted Distal Gastrectomy: LADG)과 기존의 개복 원위부 위절제술(Con- ventional Open Distal Gastrectomy: CODG)을 비교한 연구 (9-13)는 많지 않은 상태이며 이러한 비교 연구들의 림프절 절제 범위를 살펴보면 위 주위 림프절과 7번 림프절 절제로 제한된 연구가 많다.(9,10,12,13)
본 연구는 조기위암에서 LADG와 CODG의 수술 결과를 비교하여 복강경 수술의 안정성과 타당성을 알아보고자 하 였다.
방 법
1) 대상
2002년 1월부터 2003년 12월까지 만 2년 동안 본원 외과 에서 조기 위암에서 근치적 원위부 위절제술이 시행된 환 자는 147명이었으며 이중 LADG가 71명에서 시행되었다.
동아대학교 병원의 위암 데이터 베이스를 이용하여 양군간 의 임상병리학적 인자, 술 후 결과들과 경과, 술 후 합병증 및 사망률 등을 비교하였으며 다른 장기의 암과 동반된 경 우와 이전에 상복부 수술을 시행 받은 경우는 본 연구에서 제외되었다.
통계학적 분석은 연속변수에 대해 Unpaired Student's T test와 Mann-Witney U test를 사용하였고, 절대변수에 대해 Chi-square test를 사용하였다. 모든 경우에서 P값은 0.05 미 만 일 때 유의하다고 판정하였다.
2) 수술 방법
(1) LADG의 술기: 술자는 환자의 오른편에, 제1조수는 환자의 왼편에 위치하고 제2조수는 다리 사이에 위치한다.
10 mm의 camera 투관침 한 개와 2개의 12 mm 투관침, 2개 의 5 mm 투관침을 이용하였다. 복강경은 25도를 이용하였 고 7, 8a, 9번 림프절을 절제할 때는 50도로 바꾸어 사용하 였다. 이산화탄소를 이용한 기복압은 10∼14 mmHg로 유지 하였으며, 대망은 위대망혈관으로 부터 비장의 하극 방향 으로 위에서 4 cm 가량 떨어져 복강경용 지혈기구(The Li- gasureTM Vessel Sealing System, Valleylab, Boulder, Colorado, USA)를 이용하여 절제하였다. 좌위대망 혈관의 근위부는 ultrasonic dissector (Autosonix, Tyco/US Surgical Inc., Nor- walk, CT)로 박리하고 LigasureTM로 이중 결찰하여 잘랐다.
4번 림프절을 위의 대만곡에서 분리한 후 우위대망 동정맥 을 그 기시부에서 이중으로 결찰하고 각각 잘랐으며 우위 동맥 또한 그 기시부에서 이중 결찰 후 잘랐으며 복강경 자동문합기(Endo cutter 45 staple; Ethicon, Ohio, USA)를 이 용하여 유문부의 원위부 1 cm에서 십이지장을 절단하였다.
8a, 9, 11p번(LN along the proximal splenic artery) 림프절을 ultrasonic dissector (Autosonix, Tyco/US Surgical Inc., Nor-
walk, CT)와 갈고리 모양의 bovie를 이용하여 각 혈관을 따 라 절제하였다(Fig. 1). 술 전에 점막하층암이 의심된 경우 는 8p번 림프절(LN along the common hepatic artery (pos- terior group)), 12a번 림프절(LN in the hepatoduodenal liga- ment along the hepatic artery), 14v번 림프절(LN along the superior mesenteric vein)를 추가로 절제하였다. 좌위동정맥 을 각각 확인하여 자른 후 7번 림프절(LN along the left gastric artery)을 절제하였다. 이후 위주위 림프절을 위식도 연결부에서 위 하부 체부의 소만을 따라 절제하였다. 흉골 하에서 5 cm의 상부정중을 절개하여 위를 몸밖으로 끄집어 내어 원위부 2/3를 자동문합기(Proximate linear cutter 100 mm; Ethicon, Ohio, USA)을 이용하여 절제하였으며 B-I 위 십이지장 문합술은 원형 자동문합기(Proximate CDH 25;
Ethicon, Ohio, USA)를 이용하여, B-II 위공장 문합술은 복강 경 자동 문합기(Endo cutter 45 staple; Ethicon, Ohio, USA) 2개를 이용하거나 수기로 개복술과 같은 방법으로 문합하 였다.
(2) 수술 전후 관리: 양군의 환자들은 수술 후 표준화된 관리로 치료하였다. 술 전 비위관 삽입과 장세척을 시행하 지 않았고, 수술 중 위 내용물의 배출을 최소화하였으며, 수 술 후 복강내 폐쇄형 흡입 배액관을 하나 삽입하였다. 또한 수술 후 48시간부터 소량의 물을 섭취하게 하였고, 가스배 출 후 위절제 식이를 시작하였는데 미음을 하루 먹게 한 후 유동식으로 진행하였다. 수술 후 혈색소 수치가 8 g/dl 이하이고 빈혈에 대한 증상이 없는 한 수혈은 하지 않았다.
모든 환자는 자가통증 조절장치(butorphanol 20 mg, ket- olorac 300 mg, metoclopramide 30 mg, saline 100 ml)를 이용 Fig. 1. Intraoperative findings of laparoscopy-assisted distal gas- trectomy (LDAG) with extraperigastric lymph node dis- section for gastric cancer. After no. 8 and 11p lymph nodes had been dissected, the common hepatic artery (CHA), splenic artery (SA), left gastric artery (LGA) and gastro- duodenal artery (GDA) were exposed.
Pancreas GDA
CHA
LGA
SA
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
하여 수술 후 3∼4일간 1 ml/h의 용량으로 통증을 조절하였 다. 환자가 유동식 식사에 원활하고 열이 나지 않으면 퇴원 을 권유하였다.
결 과
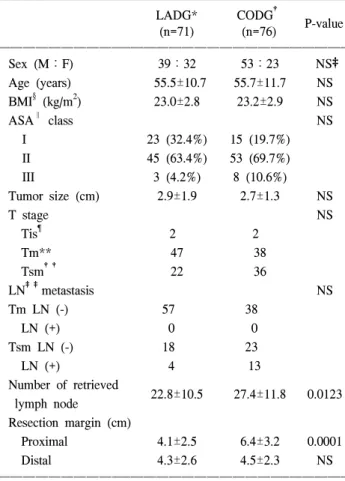
2002년 1월부터 2003년 12월까지 조기위암 환자에서 LADG를 시행 받은 환자는 71명이었으며, CODG를 시행 받 은 환자는 76명이었다. 성별, 나이, 비만도(body mass index, BMI), American Society of Anesthesiology (ASA) class, 종양 의 크기, 병변의 침습정도, 림프절 전이 등은 양 군간에 차 이가 없었다(Table 1). 그러나 LADG군에서 CODG군에 비 해 전체 절제된 림프절의 수가 적었으며 근위부 절제 거리 가 통계적으로 유의하게 짧았다. 절제된 림프절의 수의 차 이에서 전체 림프절 수는 통계적으로 유의하게 차이가 있 었으나 D1+α (D1+7번 림프절) 림프절 절제술과 D1+β (D1+7, 8a, 9번 림프절)(Japanese Gastric Cancer Association
(JGCA) 분류(23)) 림프절 절제술이 시행된 경우를 비교하였 을 때 양 군간의 유의한 차이는 없었다(Table 2).
Table 3은 두 군간의 술 후 결과들과 경과를 나타내고 있 다. 수혈이 시행된 환자의 수와 가스 배출 시간은 양 군간에 차이를 보이지 않았고 LADG가 시행된 군에서 수술 절개 창이 작았고 추가 진통제 투여 횟수가 작았으며 술 후 재원 일수가 짧았다. 술 후 7일째 알부민 수치가 LADG군에서 높았으며 술 후 첫날 백혈구 수는 적었다. 평균 수술 시간은 LADG군이 평균 249분으로 개복군 평균 수술시간 181분과 비교하여 통계적으로 유의하게 길었다.
전체 환자의 술 후 합병증 및 사망률(수술 후 30일 이내) 은 각각 17.0%와 0.7%였으며 양 군간의 유의한 차이는 없 Table 1. Clinicopathologic characteristics
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
LADG* CODG†
P-value
(n=71) (n=76)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Sex (M:F) 39:32 53:23 NS‡
Age (years) 55.5±10.7 55.7±11.7 NS
BMI§ (kg/m2) 23.0±2.8 23.2±2.9 NS
ASA∥ class NS
I 23 (32.4%) 15 (19.7%)
II 45 (63.4%) 53 (69.7%)
III 3 (4.2%) 8 (10.6%)
Tumor size (cm) 2.9±1.9 2.7±1.3 NS
T stage NS
Tis¶ 2 2
Tm** 47 38
Tsm†† 22 36
LN‡‡metastasis NS
Tm LN (-) 57 38
LN (+) 0 0
Tsm LN (-) 18 23
LN (+) 4 13
Number of retrieved
22.8±10.5 27.4±11.8 0.0123 lymph node
Resection margin (cm)
Proximal 4.1±2.5 6.4±3.2 0.0001
Distal 4.3±2.6 4.5±2.3 NS
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*LADG = laparoscopy-assisted distal gastrectomy; †CODG = con- ventional open distal gastrectomy; ‡NS = not significant; §BMI
= body mass index; ∥ASA = American society of anesthesiology;
¶Tis = carcinoma in situ; **Tm = mucosa; ††Tsm = submucosa;
‡‡LN = lymph node; Values are mean±standard deviations.
Table 2. Number of retrieved lymph nodes according to the extent of lymphadenectomy
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ LADG* (n=71) CODG† (n=76) P value ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ D1+No7 16.5±8.0 (n=11) 9.0±5.6 (n=3) 0.1617 D1+β 23.7±11.6 (n=42) 21.6±7.6 (n=34) 0.3785 D2 24.5±7.7 (n=18) 33.9±11.1 (n=39) 0.0019 ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Overall 22.8±10.5 27.4±11.8 0.0123
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*LADG = laparoscopy-assisted distal gastrectomy; †CODG = con- ventional open distal gastrectomy; Values are mean±standard de- viations.
Table 3. Postoperative outcomes and course
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ LADG* CODG†
P value
(n=71) (n=76)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Wound size (cm) 5.3±0.5 18.4±1.8 <.0001 Operation time (minute) 249.7±46.3 181.0±37.8 0.0001 Transfused patients (%) 14.1% (10/71) 7.0% (5/76) NS‡ Additional analgesics (times) 0.2±0.5 0.5±0.9 0.0370 Time to first flatus (days) 3.8±1.9 3.6±1.0 NS Postoperative hospital
9.1±3.4 10.8±3.9 0.0176 stay (days)
Albumin (g/dl)
POD§ 1 3.4±1.0 3.1±0.4 0.0568
POD 7 3.6±1.0 3.1±0.5 0.0002
Leukocyte (103/ul)
POD 1 12.5±3.7 13.7±3.7 0.0445
POD 3 9.4±3.0 10.0±3.2 NS
POD 7 7.8±2.3 8.0±3.3 NS
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*LADG = laparoscopy-assisted distal gastrectomy; †CODG = conventional open distal gastrectomy; ‡NS = not significant;
Values are mean±standard deviations; §POD = postoperative day.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
었고 CODG군에서 일어날 수 있는 다양한 합병증이 LADG 군에도 발생하였다(Table 4). 모든 환자에서 4개월에서 28개 월간 환자의 경과를 관찰하였으나 재발이나 투관 침 전이 는 없었다. 대합병증은 재수술이 필요한 경우로 정의하였 는데 대합병증은 LADG군에서 2명, CODG군에서 1명이 발 생하였다. 복강경군에서는 비장경색과 술 후 복강 내 출혈 이 각각 1명씩 발생하였고, 개복군에서는 십이지장절단부 의 누출이 1명에서 발생하였다. LADG 후에 비장경색이 있 던 환자는 술 후 44일째 폐부전으로 사망하였으며 CODG 후에 1명의 환자는 패혈증이 발생하여 술 후 19일째 다발성 장기부전으로 사망하였다.
고 찰
최근 복강경 위암 수술의 장점들에 대해 연구들이 있었 지만 주로 비무작위 후향적 연구가 대부분이다.(14-17) 조 기 위암 환자에서 LADG와 CODG에 대한 무작위 전향적 연구가 Kitano 등(9)에 의해 이루어졌는데 이 연구에서는 림 프절 절제 범위를 위주위 림프절과 7 번 림프절로 제한하였 으나 연구에 포함된 환자는 점막암, 점막하층암, 고유 근육
층암 등이 포함되어 있었다. 점막하층의 위암을 복강경 수 술에 적용하기 위해서는 위주위 림프절 뿐만 아니라 위주 위 외의 림프절 절제도 필요하다.(24) 최근에 Fujiwara 등 (18)이 43명의 조기위암 환자에서 위주위 림프절과 위주위 외의 림프절 절제가 시행된 LADG의 결과를 보고하였다.
불행하게도 이 연구에서는 상대적으로 높은 합병증으로 인 해 위암 환자의 복강경 수술의 적용에 대해 좀더 많은 연구 가 필요함을 제안하였다.
본 연구는 만 2년간 두 명의 술자에 의하여 147명의 조기 위암 환자에서 시행된 LADG와 CODG의 비무작위 후향적 연구이다. 본 연구에서는 LADG가 CODG보다 술 후 합병증 이나 수술과 관련된 사망률의 증가 없이 수술 후 통증이 적고 입원기간이 짧으며 영양학적 변화가 작았고 술 후 환 자의 염증 반응이 적다는 등의 여러 가지 장점이 있음을 보여 주었다.
절제된 림프절의 수는 수술의 근치도 즉 림프절 절제 범 위와 관련이 있다. 절제된 림프절의 수는 LADG가 CODG에 비해 작았으나 이 결과는 양 군의 림프절 절제 범위에 따른 환자의 수가 차이가 나기 때문이었다. LADG를 시행한 환 자 71명 중 42명(59.2%)이 D1+β (D1+7, 8a, 9번 림프절) 림프절 절제술이 시행되었고, CODG의 경우 76명 중 39명 (51.3%)이 D2 (D1+β+11p, 12a, 14v번 림프절) 림프절 절 제술을 시행하였다.(23) 두 군간에 있어 D1+α (D1+7번 림프절) 림프절 절제술과 D1+β (D1+7, 8a, 9번 림프절) 림프절 절제술에서 제거된 림프절 수를 비교하여 보면 두 군간에 유의한 차이는 없었다. 그러나 D2 (D1+β+11p, 12a, 14v번 림프절) 림프절 절제술을 비교했을 경우 제거된 림프절 수는 LADG가 CODG에 비하여 유의하게 작았다.
LADG에서 D2 림프절 절제술은 더 많은 연구와 기술적 극 복이 있어야 할 것으로 생각된다.
일본 위암 치료의 권고안에 따르면 T1 병변에서는 병변 과 절단면과의 거리가 1 cm, T2-3 병변에서는 3∼5 cm 정도 가 필요하다고 기술하고 있다.(24) 본 연구에서는 근위부 절단면과 병변과의 거리가 LADG의 경우 CODG에 비해 훨 씬 짧았지만(4.1 cm vs 6.4 cm; P<0.0001) 평균 4.1 cm의 근 위부 절단면과 병변의 거리는 T1 병변의 경우에 충분하다 고 생각한다.
본 연구에서 수술시간은 LADG에서 CODG보다 유의하 게 길었지만(249.7분 vs 181.0분; P<0.0001), 술 후 재원기간 은 LADG에서 CODG에 비해 통계적으로 유의하게 짧았 다.(9.1일 vs 10.8일; P=0.0176) 합병증이 없었던 대부분의 LADG 환자들은 술 후 6∼7일째 퇴원이 가능하였다. 본 연 구의 LADG에 걸린 평균 수술 시간은 다른 연구들의 결과 들과 비슷하였다.(10-12)
술 후 장마비의 정확한 기전은 아직 밝혀져 있지 않다.
Carli 등은 술 후 장마비는 수술의 스트레스와 원심성 교감 신경 경로의 자극으로 유발된 교감신경의 과항진과 연관된 Table 4. Postoperative morbidities and mortalities
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ LADG* CODG†
P value
(n=71) (n=76)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Major complication NS‡
Duodenal stump leakage 1
External bleeding 1
Spleen infarction 1
Minor complication NS
Anastomotic site bleeding 3 3
External bleeding 1
Intraabdominal abscess 1 1
Wound infection 1
seroma 1
evisceration 2
Intestinal obstruction 1
Paralytic ileus 1
Pancreatitis 1
Lymphorrhea 1
Pleural effusion 1
Dumping syndrome 1 1
Peroneal nerve palsy 1
Aggravated gout 1
Postoperative mortality 1 NS
Death in hospital 1 NS
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*LADG = laparoscopy-assisted distal gastrectomy; †CODG = con- ventional open distal gastrectomy; ‡NS = not significant.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 다고 하였다.(25) 위 수술에서 가스배출은 LADG에서 평균
2.5∼3.9일, 기존의 CODG에서 평균 3.5∼4.5일이 소요된다 고 보고하고 있다.(9,10,26) 본 연구의 가스 배출 시기는 LADG에서 3.8일, CODG에서 3.6일로 양군간에 차이가 없 었다.
Goh 등(27)은 12개국 16명의 수술자에게 질문서를 보내 어 그 중 10명(62%)으로부터 LADG가 CODG에 비해 통증 이 적고 회복이 빠르고 미용적으로 효과가 뛰어나 좀더 나 은 수술방법이라고 믿고 있다는 회신을 받았다고 보고하였 고 최근의 비교 연구들에서도 LADG가 개복술에 비해 명백 히 장운동이 더 빨리 회복되고 출혈이 적으며 진통제의 사 용이 적고 경구 식이가 더 빠르고 재원기간이 짧은 장점이 있다고 주장하였다.(10,11) 또한 Adachi 등(10)은 복강경 수 술이 술 후 급성기 반응을 감소시키고 수술의 손상을 최소 화하고 수술에 따른 면역 기능 저하를 최소화한다고 주장 하여 일부 동물실험에서 제기되었던 이산화탄소를 이용한 기복이 종양학적으로 좋지 않다는 염려를 불식시키기도 하 였다.
국내적으로 복강경 위 수술은 1999년 김 등(28)이 술기적 가능성을 제안한 바 있으며 2002년 이 등(19)은 조기 위암 에서 LADG와 hand-assisted 복강경 수술을 26명의 환자에서 전향적으로 시행하여 비교한 연구를 발표한 바 있다. 최근 복강경을 이용한 위 수술은 점차 확대되어 가고 있는 추세 로 생각된다.
국외의 연구들에 의하면 LADG 후 발생한 합병증은 발생 자체도 매우 적고 대부분 소합병증으로 재수술이나 사망에 대한 보고는 거의 없다. 그러나 본 연구 결과에 의하면 LADG 역시 개복술에서 발생할 수 있는 다양한 합병증이 발생하였고 재수술과 술 후 사망까지도 발생할 수 있는 수 술이므로 숙련된 술자에 의하여 조심스럽게 시행되어야 할 것으로 생각된다.
결 론
광범위 림프절 절제를 포함한 LADG는 조기 위암 환자에 서 술기적으로 가능하며 숙련된 술자에 의하여 시행된다면 개복술과 비교하여 수술 직후 환자의 회복적인 측면에서 여러 가지 장점을 가지며 환자의 삶의 질을 향상시킬 수 있는 술기라고 할 수 있다. 향후 복강경 술기의 표준화를 이루어 다 기관에서 전향적 연구를 시행된다면 조기 위암 의 표준 수술의 하나로 자리할 수 있을 것으로 생각한다.
REFERENCES
1) Lau H. Laparoscopic repair of perforated peptic ulcer: a meta- analysis. Surg Endosc 2004;18:1013-21.
2) Rothlin M, Schob O. Laparoscopic wedge resection for benign
gastric tumors. Surg Endosc 2001;15:893-5.
3) Uyama I, Sugioka A, Fujita J, Komori Y, Matsui H, Soga R, et al. Completely laparoscopic extragastric lymph node dis- section for gastric malignancies located in the middle or lower third of the stomach. Gastric Cancer 1999;2:186-90.
4) Uyama I, Sugioka A, Fujita J, Komori Y, Matsui H, Hasumi A. Laparoscopic total gastrectomy with distal pancreaticosplec- tomy and D2 lymphadectomy for early gastric cancer. Gastric Cancer 1999;2:230-4.
5) Huscher CG, Anastasi A, Crafa F, Recher A, Lirici MM.
Laparoscopic gastric resections. Semin Laparosc Surg 2000;7:
26-54.
6) Horiuchi T, Shimomatsuya T, Chiba Y. Laparoscopically as- sisted pylorus-preserving gastrectomy. Surg Endosc 2001;15:
325-8.
7) Mochiki E, Kamimura H, Haga N, Asao T, Kuwano H. The technique of laparoscopically assisted total gastrectomy with jejunal interposition for early gastric cancer. Surg Endosc 2002;16:540-4.
8) Uyama I, Sugioka A, Matsui H, Fujita J, Komori Y, Hatakawa Y, et al. Laparoscopic side to side esophagogastrostomy using a linear stapler after proximal gastrectomy. Gastric cancer 2001;4:98-102.
9) Kitano S, Shiraishi N, Fujii K, Yasuda K, Inomata M, Adachi Y. A randomized controlled trial comparing open vs laparos- copy-assisted distal gastrecomy for the treatment of early gastric cancer: an interim report. Surgery 2002;131:306-11.
10) Adachi Y, Shiraishi N, Shiromizu A, Bandoh T, Aramaki M, Kitano S. Laparoscopy-assisted billroth I gastrectomy com- pared with conventional open gastrectomy. Arch Surg 2000;
135:806-10.
11) Tanimura H, Higashino M, Fukunaga Y, Osugi H. Laparos- copic distal gastrectomy with regional lymph node dissection for gastric cancer. Surg Endosc 2003;17:758-62.
12) Weber KJ, Reyes CD, Gagner M, Divino CM. Comparison of laparoscopic and open gastrectomy for malignant disease. Surg Endosc 2003;17:968-71.
13) Migoh S, Hasuda K, Nakashima K, Anai H. The benefit of laparoscopy-assisted distal gastrectomy compared with conven- tional open distal gastrectomy: a case matched control study.
Hepatogastroenterology 2003;50:2251-4.
14) Tanimura S, Higashino M, Fukunaga Y, Osugi H. Laparos- copic gastrectomy with regional lymph node dissection for upper gastric cancer. Gastric Cancer 2003;6:64-8.
15) Shiraishi N, Adachi Y, Kitano S, Bandoh T, Katsuta T, Mori- moto A. Indication for and outcome of laparoscopy-assisted billroth I gastrectomy. Br J Surg 1999;86:541-4.
16) Asao T, Hosouchi Y, Nakabayashi T, Haga N, Mochiki E, Kuwano H. Laparoscopically assisted total or distal gastrec- tomy with lymph node dissection for early gastric cancer. Br J Surg 2001;88:128-32.
17) Noshiro H, Shimizu S, Nagai E, Ohuchida K, Tanaka M.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Laparoscopy-assisted distal gastrectomy for early gastric
cancer: Is it beneficial for patients of heavier weight? Ann Surg 2003;238:680-5.
18) Fujiwara M, Kodera Y, Fujiwara M, Ito S, Mochizuki Y, Yamamura Y, et al. Laparoscopy-assisted distal gastrectomy with systemic lymph node dissection for early gastric carci- noma: a review of 43 cases. J Am Coll Surg 2003;196:75-81.
19) Yi NJ, Kim YW, Han HS. Laparoscopy-assisted Billroth I gastrectomy compared with Hand-assisted laparoscopic surgery for early gastric cancer A Prospective study - J Korean Surg Soc 2002;62:57-63.
20) Gutt CN, Gessmann T, Schemmer P, Mehrabi A, Schmandra T, Kim ZG. The impact of carbon dioxide and helium insuf- flation on experimental liver metastases, macrophages, and cell adhesion molecules. Surg Endosc 2003;17:1628-31.
21) Gutt CN, Riemer V, Brier C, Berguer R, Paolucci V. Stan- dardized technique of laparoscopic surgery in the rat. Dig Surg 1998;15:371-5.
22) Jacobi CA, Sabat R, Bohm B, Zieren HU, Volk HD, Muller JM. Pneumoperitoneum with carbon dioxide stimulates growth
of malignant colonic cells. Surgery 1997;121:72-8.
23) Japanese Gastric Cancer Association. Japanese classification of gastric carcinoma, 2nd English ed. Gastric Cancer 1998;1:
10-24.
24) Nakajima T. Gastric cancer treatment guidelines in Japan.
Gastric Cancer 2002;5:1-5.
25) Carli F, Trudel JL, Belliveau P. The effect of intraoperative thoracic epidural anesthesia and postoperative analgesia on bowel function after colorectal surgery: a prospective, rando- mized trial. Dis Colon Rectum 2001;44:1083-9.
26) Mochiki E, Nakabayashi T, Kamimura H, Haga N, Asao T, Kuwano H. Gastrointestinal recovery and outcome after laparoscopy-associated versus conventional open distal gastec- tomy for early gastric cancer. World J Surg 2002;26:1145-9.
27) Goh PMY, Alponat A, Mak K, Kum CK. Early international results of laparoscopic gastrectomies. Surg Endosc 1997;11:
650-2.
28) Kim HH, Cho SH, Kim SS. Laparoscopic Billroth-II gastrec- tomy for benign gastric diseases. J Korean Surg Soc 1999;
56:664-70.