투고일: 2011년 6월 15일, 심사일: 2011년 6월 20일, 게재확정일: 2011년 7월 1일 책임저자:박진우, 경기도 고양시 일산동구 식사동 814
(410-773) 동국대학교 일산병원 재활의학과 Tel: 031) 961-7484, Fax: 031) 961-7488 E-mail: [email protected]
Copyrights ⓒ The Korean Dysphagia Society, 2011.
비디오 투시 삼킴 검사에서 점수화 도구들
박진우
동국대학교 일산병원 재활의학과
Scoring System in Videofluoroscopic Swallowing Study
Jin-Woo Park, M.D., Ph.D.
Department of Physical Medicine and Rehabilitation, Dongguk University Ilsan Hospital, Goyang, Korea
Videofluoroscopic swallowing study (VFS) is accepted as a gold standard tool for evaluating dysphagia. The real time video radiographic image provides visualization of the structures, movement, and coordination of swallowing.
Abnormal oropharyngeal and esophageal anatomy can be readily identified. There are several scoring systems for analyzing VFS; A Penetration-Aspiration Scale (PAS), The Dysphagia Outcome and Severity Scale (DOSS), National Institutes of Health Swallowing Safety Scale (NIH-SSS) and Videofluoroscopic Dysphagia Scale (VDS). They can pro- vide reliable quantification of selected events observed during VFS and be used as powerful outcome measures to investigate the efficacy of various swallowing treatments. This article reviews these scoring systems. (JKDS 2011;1:55-59)
Keywords: Dysphagia, Deglutition disorders, Evaluation, Scale
서론
비디오 투시 삼킴 검사(videofluoroscopic swallowing study; VFS)는 삼킴 이상의 진단을 위해 가장 많이 사용하 는 검사법이며, 현재 표준 검사로 인정을 받고 있다1,2. Logemann은 1980년대 초반 표준화된 방법을 제시하였고 이후 약간씩의 변형은 있지만 기본 틀이 되고 있다3,4. 검사 를 통해 삼킴 과정과 관련된 해부학적 구조(구강, 인두, 후 두, 식도)와 그들의 움직임, 조화 등을 관찰할 수 있으며 기도 흡인의 원인을 확인하고 치료적인 접근을 동시에 할 수 있는 장점이 있다5.
이러한 비디오 투시 삼킴 검사의 결과를 정량화 해 보려
는 노력들이 이루어졌고 몇몇 점수화 도구들이 개발되었 다. 연구자들은 이 도구들을 통해 치료 효과를 판정하거나 병의 예후를 예측하기도 하였다. 본 논문에서는 이러한 점 수화 도구들에 대하여 알아보고자한다.
본론
1. A Penetration Aspiration Scale (PAS) Rosenbek 등에 의해 개발되어 1996년 발표되었다6. 이 들은 비디오 투시 삼킴 검사에서 후두 통과와 기도 흡인 두 가지 결과만을 가지고 8단계의 척도를 만들었다.(Table 1) 후두 통과란 음식물이 후두로 들어가지만 성대주름 아래
Table 1. Penetration-aspiration scale.
1. Material does not enter the airway
2. Material enters the airway, remains above the vocal folds, and is ejected from the airway
3. Material enters the airway, remains above the vocal folds, and is not ejected from the airway
4. Material enters the airway, contacts the vocal folds, and is ejected from the airway
5. Material enters the airway, contacts the vocal folds, and is not ejected from the airway
6. Material enters the airway, passes below the vocal folds and is ejected into the larynx or out of the airway 7. Material enters the airway, passes below the vocal folds,
and is not ejected from the trachea despite effort 8. Material enters the airway, passes below the vocal folds,
and no effort is made to eject
로는 통과하지 않는 것을 말하며 기도 흡인은 성대주름 아래 로 음식물이 내려가는 것을 뜻한다. 이 척도의 단계를 나누 는 기준은 성대주름을 기준으로 음식물이 들어간 깊이와 이 음식물이 기침 등을 통해 밖으로 나오는지 여부로 하였다.
척도의 상세 내용은 다음과 같은데, 1점은 음식물이 기 도로 들어가지 않은 경우, 2점은 기도로는 들어갔으나 성대 주름 상부에 머물면서 기도 밖으로 배출된 경우, 3점은 2점 과 같은 상태에서 기도 밖으로 배출이 되지 않은 경우, 4점 은 음식물이 기도로 들어가서 성대주름과 닿았으나 다시 배 출된 경우, 5점은 4점과 같은 상태에서 배출이 되지 않은 경우, 6점은 성대주름 하부로 통과하였으나 후두 혹은 기도 밖으로 배출된 경우, 7점은 6점과 같은 상태에서 배출이 되 지 않은 경우 이며 마지막 8점은 7점과 같은 상태에서 배출 에 대한 노력이 전혀 보이지 않는 경우로 침묵 흡인(silent aspiration)을 가리킨다.
본 도구의 장점은 무엇보다도 간단하다는 것이다. 그렇 기 때문에 쉽게 적용이 가능하여 현재까지 가장 널리 사용 되며 가장 많이 인용되고 있다. 또한 검사의 신뢰도에서 검 사자 내 일치도가 63-84% 정도를 보였으며 검사자 간 일치 도는 60-75%로 나타나 아주 높지는 않지만 비교적 괜찮은 결과를 보여 이를 뒷받침 해주고 있다. 하지만 비디오 투시 삼킴 검사에서의 다양한 소견을 반영하지 못하고 오로지 후 두통과나 기도흡인만 집중되어 있다는 것이 큰 단점으로 지 적되고 있다. 또한 환자에 적용했을 때 1점부터 8점까지 고르게 분포를 하지 못하고 양쪽으로 치우쳐져 있으며 4점 의 경우는 해당되는 경우가 거의 없는 것도 단점으로 얘기 되고 있다.
2. The Dysphagia Outcome and Severity Scale (DOSS)
이 도구는 O’Neil 등에 의해 1999년 개발되어 발표 되었 다7. 비디오 투시 삼킴 검사 결과에 기초하여 독립성의 정 도, 영양 수준, 식사의 변형 정도에 따라 7단계의 기능적 척도 만들었다. 이는 삼킴 장애를 장애(disability)의 한 부 분으로 보고 장애 평가에 많이 이용되는 기능적 평가 척도 인 기능적 독립 측정(Functional Independence Measure;
FIM)8 도구에 기초하여 그 단계 구분을 이루었고 기능적 측정이라는 것에 많은 강조점을 두었다. 또한 그 구성에 후 두통과와 기도흡인의 내용뿐만 아니라 구강기의 이동 및 인 두기의 저류까지 넣어 평가 하였다는 특징을 가지고 있 다.(Table 2)
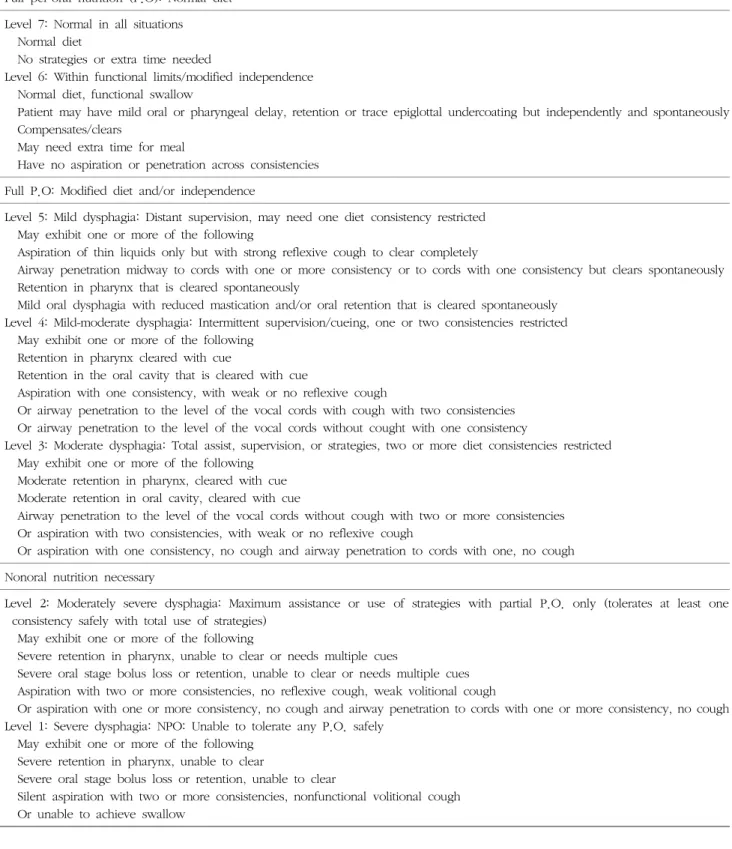
구체적으로 살펴보면 크게 완전한 구강 섭취, 독립적이 나 변형된 구강 섭취, 그리고 구강 외 영양 공급으로 3가지 단계로 나뉘며 각각의 단계에서 2 내지 3단계의 세분화된 내용으로 구성되어 있다. 7단계는 가장 높은 단계로 아무런 변형이나 치료 없이 정상적인 상태를 뜻하고 6단계는 식사 시 시간이 좀 더 걸린다던지, 구강기에 약간의 지연 등이 관찰되어 기능적 제한이 있긴 하나 독립 수준은 유지하는 상태를 뜻한다. 5단계는 경도의 삼킴 장애로 한가지 정도의 점도 제한이 필요한 수준이다. 4단계는 경도 내지 중간 정 도 삼킴 장애로 때때로 관리감독이 필요하고 하나 혹은 두 가지의 점도 제한이 필요한 상태이고 3단계는 중간 정도 삼킴 장애로 지속적 도움이 필요하며 두 가지 이상의 점도 제한이 필요한 상태이다. 2단계는 중간 내지는 중증의 삼킴 장애로 경구 섭취는 부분적으로 가능한 상태이고 1단계는 중증의 삼킴 장애로 절대 구강 영양을 할 수 없는 상태를 뜻한다.
이 도구의 장점은 기능적 측면을 고려하여 단계 구분에 반영하였다는 점과 구강기 및 인두기를 포괄적이지는 않지 만 포함했다는 점이다. 또한 신뢰도 면에서도 검사자 내 일 치도가 86-100%, 검사자 간 일치도가 82-100%로 매우 높 게 나타났다. 하지만 단계별 내용 구성이 다소 복잡하여 매 우 숙달되지 않으면 도표를 외우기가 쉽지 않으며 단계별 구분에서도 모호성을 띠어 정확한 구분이 어려운 경우가 많 다. 그리고 단계가 진행함에 따라 진정으로 연하장애가 심 해지는 것인지에 대한 것은 좀 더 고찰이 필요하다.
3. National Institutes of Health Swallowing Safety Scale (NIH-SSS)
이 도구는 Ludlow 등에 의해 2006년 개발되었는데9 이
Table 2. Dysphagia outcome and severity scale-final revision.
Full per-oral nutrition (P.O): Normal diet Level 7: Normal in all situations Normal diet
No strategies or extra time needed
Level 6: Within functional limits/modified independence Normal diet, functional swallow
Patient may have mild oral or pharyngeal delay, retention or trace epiglottal undercoating but independently and spontaneously Compensates/clears
May need extra time for meal
Have no aspiration or penetration across consistencies Full P.O: Modified diet and/or independence
Level 5: Mild dysphagia: Distant supervision, may need one diet consistency restricted May exhibit one or more of the following
Aspiration of thin liquids only but with strong reflexive cough to clear completely
Airway penetration midway to cords with one or more consistency or to cords with one consistency but clears spontaneously Retention in pharynx that is cleared spontaneously
Mild oral dysphagia with reduced mastication and/or oral retention that is cleared spontaneously Level 4: Mild-moderate dysphagia: Intermittent supervision/cueing, one or two consistencies restricted May exhibit one or more of the following
Retention in pharynx cleared with cue
Retention in the oral cavity that is cleared with cue
Aspiration with one consistency, with weak or no reflexive cough
Or airway penetration to the level of the vocal cords with cough with two consistencies Or airway penetration to the level of the vocal cords without cought with one consistency
Level 3: Moderate dysphagia: Total assist, supervision, or strategies, two or more diet consistencies restricted May exhibit one or more of the following
Moderate retention in pharynx, cleared with cue Moderate retention in oral cavity, cleared with cue
Airway penetration to the level of the vocal cords without cough with two or more consistencies Or aspiration with two consistencies, with weak or no reflexive cough
Or aspiration with one consistency, no cough and airway penetration to cords with one, no cough Nonoral nutrition necessary
Level 2: Moderately severe dysphagia: Maximum assistance or use of strategies with partial P.O. only (tolerates at least one consistency safely with total use of strategies)
May exhibit one or more of the following
Severe retention in pharynx, unable to clear or needs multiple cues
Severe oral stage bolus loss or retention, unable to clear or needs multiple cues Aspiration with two or more consistencies, no reflexive cough, weak volitional cough
Or aspiration with one or more consistency, no cough and airway penetration to cords with one or more consistency, no cough Level 1: Severe dysphagia: NPO: Unable to tolerate any P.O. safely
May exhibit one or more of the following Severe retention in pharynx, unable to clear
Severe oral stage bolus loss or retention, unable to clear
Silent aspiration with two or more consistencies, nonfunctional volitional cough Or unable to achieve swallow
도구에 대한 단독 연구는 없으며 저자들의 삼킴 장애 관련 연구에 측정 도구로서 사용되었다. 점수는 각 항목에서 이 상을 보이면 1점이 주어지도록 하였는데 그 항목에는 후두
덮개계곡 고임, 조롱박오목에 고임, 하인두에서 시작된 후 두통과, 조롱박오목에서 시작된 후두통과가 있다. 기도 흡 인의 경우 그 횟수를 모두 세어 점수를 매겼고 식도로 이동
Fig. 1. National institutes of health swallowing safety scale (revised version).
Table 3. Videofluoroscopic dysphagia scale.
Parameter Coded value Score
Lip closure
Bolus formation
Mastication
Apraxia
Tongue to palate contact
Premature bolus loss
Oral transit time Triggering of
pharyngeal swallow Vallecular residue
Laryngeal elevation Pyriform sinus residue
Coating of pharyngeal wall
Pharyngeal transit time Aspiration
Total
Intact Inadequate None Intact Inadequate None Intact Inadequate None None Mild Moderate Severe Intact Inadequate None None
<10%
10-50%
>50%
≤1.5s
>1.5s Normal Delayed None
<10%
10-50%
>50%
Normal Impaired None
<10%
10-50%
>50%
No Yes
≤1.0s
>1.0s None Supraglottic
penetration Subglottic
aspiration
0 2 4 0 3 6 0 4 8 0 1.5 3 4.5 0 5 10 0 1.5 3 4.5 0 3 0 4.5 0 2 4 6 0 9 0 4.5 9 13.5
0 9 0 6 0 6 12
4
6
8
4.5
10
4.5
3 4.5 6
9 13.5
9 6 12
100 된 음식물의 양에 따라 2점까지 주도록 하였다.(Fig. 1)
매우 간단하여 사용하기 쉽고 인두의 저류 및 식도 통과 여부에 대한 것까지 반영되어 매우 실용적이다. 하지만 구 강기에 대한 반영이 없고 이 도구에 대한 신뢰도 연구가 되어 있지 않으며 설명이 부족하여 몇 회 삼킴에서 얼마까 지 점수를 더하는지 등에 대한 정보를 알 수 없는 것이 아 쉬운 점이다.
4. Videofluoroscopic Dysphagia Scale (VDS) Han 등에 의해 2008년 발표된 척도로서 14개 항목, 100 점 만점으로 구성되어 있다10. 당초에 뇌졸중 환자에서 6개 월 이후에도 회복되지 않는 경우를 예측하기 위해 만든 척 도였으나 구강기와 인두기의 많은 항목들이 포함되어 삼킴 상태를 포괄적으로 반영해 줄 수 있어 기능 평가의 척도로 도 유용하다.(Table 3)
구강기 항목으로는 입술 닫힘이 4점, 식괴 형성 6점, 저 작기능 8점, 실행증 4.5점, 혀-구개 접촉 10점, 조기 식괴 붕괴 4.5점, 구강 통과 시간 3점으로 구성되어 있고 인두기 는 인두 삼킴 유발 4.5점, 후두덮개계곡 잔여물 6점, 후두 상승 9점, 조롱박 오목 잔여물 13.5점, 인두 벽 코팅 9점, 인두 통과 시간 6점, 기도 흡인 여부 12점으로 되어 있다.
또한 각 항목들은 1-3개 세부 항목으로 나누어져 점수를 세분화 하고 있다.
이 도구의 장점은 앞서 언급했듯이 구강기와 인두기의 다양한 항목들이 중대성에 따라 가중치를 두어서 점수를 배 치하여 포괄적이면서 또한 어떤 항목이 더 심한가에 대한 논쟁을 배제시킬 수 있게 해 주었고 100점 만점으로 하고 있어 환자 변화에 대해 매우 민감하게 반영해 준다는 것이 다. 하지만 신뢰도 검증이 되어 있지 않고 식도기에 대한
반영이 되지 않은 점, 몇몇 항목에서 세부 단계 구분이 모호 한 점은 단점으로 지적되고 있다.
결론
이상에서 현재 가장 널리 사용되고 있는 비디오 투시 삼 킴 검사에 기반을 둔 점수화 도구들에 대하여 알아보았다.
각각의 도구들이 나름의 장점과 단점을 보유하고 있는 바 이를 잘 고려하여 선택하여 사용하는 것이 바람직할 것으로 사료된다. 또한 도구들이 나름의 신뢰도를 제시하고 있으 나 이는 훈련된 전문가들에 의한 결과로 이러한 도구들을 사용하기 위해서는 많은 연습과 훈련이 필요할 것이다.
REFERENCES
1. Kuhlemeier KV, Yates P, Palmer JB. Intra- and interrater variation in the evaluation of videofluorographic swal- lowing studies. Dysphagia. 1998;13:142-7.
2. Palmer JB, Kuhlemeier KV, Tippett DC, Lynch C. A pro- tocol for the videofluorographic swallowing study.
Dysphagia. 1993;8:209-14.
3. Logemann JA. Evaluation and treatment of swallowing disorders. San Diego, CA: College-Hill Press, 1983.
4. Logemann JA. Evaluation and treatment of swallowing disorders. 2nd ed. Austin, Tex.: PRO-ED, 1998.
5. Leslie P, Carding PN, Wilson JA. Investigation and man- agement of chronic dysphagia. BMJ. 2003;326:433-6.
6. Rosenbek JC, Robbins JA, Roecker EB, Coyle JL, Wood JL. A penetration-aspiration scale. Dysphagia. 1996;11:
93-8.
7. O'Neil KH, Purdy M, Falk J, Gallo L. The dysphagia out- come and severity scale. Dysphagia. 1999;14:139-45.
8. Ottenbacher KJ, Hsu Y, Granger CV, Fiedler RC. The re- liability of the functional independence measure: a quan- titative review. Arch Phys Med Rehabil. 1996;77:1226-32.
9. Humbert IA, Poletto CJ, Saxon KG, Kearney PR, Crujido L, Wright-Harp W, et al. The effect of surface electrical stimulation on hyolaryngeal movement in normal in- dividuals at rest and during swallowing. J Appl Physiol.
2006;101:1657-63.
10. Han TR, Paik NJ, Park JW, Kwon BS. The prediction of persistent dysphagia beyond six months after stroke.
Dysphagia. 2008;23:59-64.