J Health Tech Assess 2014;2(1):26-34 ISSN 2288-5811 Copyright © 2014 The Korean Association for Health Technology Assessment
서 론
한국의 심혈관질환 유병률과 이로 인한 사망률이 급격하 게 증가하고 있다. 고혈압은 이상지질혈증 및 비만, 당뇨 등 과 함께 심혈관질환의 주요 위험인자이며, 이들이 동반될 경
우 심혈관질환의 위험이 더욱 증가하기 때문에 적절한 관리 가 매우 중요하다.1) 고혈압이 이상지질혈증과 동반되었거나 여러 위험인자가 동반되어 심혈관질환 발생 위험이 높은 경 우, 혈압 조절과 동시에 3-hydroxy-3-methylglutaryl co en- zyme A reductase inhibitor(HMG-Co-A R inhibitor: statin)
Cost-Effectiveness of Single-Pill Combination Therapy of Amlodipine/Atorvastatin Compared with Concurrent Two-Pill Therapy in Patients with Hypertension in Korea
Young-Joo Kim, MS
1, Su-Kyoung Ko, MPH, PhD
1, and Cheol-Whan Lee, MD
21Pfizer Pharmaceuticals Korea Ltd., Seoul, Korea
2Department of Cardiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
한국인 심혈관질환의 일차 예방을 위한 Amlodipine/Atorvastatin 단일 복합제의 비용 효과 분석
한국 화이자제약1, 울산대학교 의과대학 서울아산병원 심장병원 심장내과학교실2
김영주1·고수경1·이철환2
Address for Correspondence:
Cheol-Whan Lee, MD Department of Cardiology, Asan Medical Center, University of Ulsan College of Medicine, 88 Olympic-ro 43-gil, Songpa-gu, Seoul 138-736, Korea
Tel: +82-2-1688-7575 Fax: +82-2-3010-5452 E-mail: [email protected]
Objectives: Single-pill combination therapy may be more effective compared with two pill ap- proach in hypertensive patients requiring concomitant statin therapy. We investigated the cost-ef- fectiveness of single-pill amlodipine/atorvastatin (SP) therapy compared with two-pill co-adminis- tration (TP) therapy for prevention of cardiovascular disease (CVD) with consideration to adherence in patients with hypertension using simulation model. Methods: Cohort simulation was per- formed with 1000 hypertensive patients at an increased risk of CVD or with concomitant dyslipid- emia. The efficacy was defined as the number of CVD prevention, which depends on differences in patients’ adherence to each alternative. ‘Adherence’ was defined as compliance to medication over 80% on proportional day covered and ‘non-adherence’ for the remaining. The number of cardiovas- cular event after TP treatment was based on the Anglo-Scandinavian Cardiac Outcomes Trial-Lipid Lowering Arm (ASCOT-LLA) trial. The proportion of the adherent patient and the cardiovascular outcome differences in adherence level were searched through systematic review. The annual costs of medicine were included according to the adherence levels of each alternative. Average cost-effec- tiveness ratio (ACER) was calculated as the cost per CVD event prevented in the cohort. All costs were described in 1000 Korean won (KRW). Results: The number of CVD prevention in SP ap- proach was higher than in TP approach by approximately 1–4 cases. Total annual medication cost with SP approach was 209719–225164 KRW which was lesser than the cost in TP approach, 261893–281993 KRW. ACERs in SP approach were lower than those in TP approach (214–231 KRW vs. 268–298 KRW per prevented CVD event, respectively). SP approach reduced medication cost by around 20% per cardiovascular prevention case than TP approach. Conclusion: SP ap- proach is cost effective compared with TP approach in hypertensive patients at risk of cardiovascu- lar event or those with concomitant dyslipidemia for CVD prevention.
Key Words Single-pill combination · Fixed-dose combination · Atorvastatin · Amlodipine · Adherence · Cardiovascular disease · Cost-effectiveness ·
Average cost-effectiveness ratio.
Original Article
JoHTA
를 사용하여 혈중 지질농도의 조절을 통해 심혈관질환을 예 방하도록 최근의 치료지침에서 권고하고 있다.2) 그럼에도 불구하고, 고혈압과 혈중 지질농도 조절률은 저조하여, 치료 받은 환자 중 절반 이하의 환자만이 혈압과 혈중 지질농도 의 목표치에 도달한 것으로 보고되고 있고,3) 이는 환자의 낮 은 복약 순응도가 하나의 이유일 것으로 지목되고 있다.4)
환자가 처방 약제를 올바르게 복용하는 것은 기대한 치료 효과를 얻기 위해 필수적이다. 처방을 제대로 지켜 복용하지 않을 경우 약리학적 치료의 유용성을 제한하는 결과를 가져 오므로 질병의 관리에 있어 중요하다.5) 복약 순응도는 약의 개수 및 복잡한 regimen과 관련이 있는 것으로 보고되고 있 기 때문에 단일 복합제 형태의 약제사용이 약의 개수에 대 한 복용 부담(pill-burden)을 감소시킬 것으로 기대되고 있 다.6,7) 실제로 최근의 연구 결과에서 단일 복합제의 투여가 단일제 병용투여에 비해 환자의 복약 순응도를 유의하게 증 가시킴이 보고된 바 있고,8) 증가된 복약 순응도는 더 나은 치료 성과를 나타내었다.9,10)
항 고혈압제인 amlodipine besylate(이하 amlodipine)와 atorvastatin calcium(이하 atorvastatin)의 단일 복합제는 단 일제 병용투여와 생물학적으로 동등한(bio-equivalent) 것 으로 입증되었고,11) 복약 순응도 측면에서 유의한 개선을 나 타내어12) 더 좋은 심혈관질환 예방효과가 기대되고 있다. 또 한, 국내에서는 복합제의 경우 단일제제 병용투여보다 약제 의 가격이 더 저렴할 뿐만 아니라, 비순응 환자의 경우 약을 복용하지 않는 만큼의 약제비 감소로 인해 순응 환자가 비 순응 환자보다 약제비가 증가할 수 있어 약제의 순응도 개 선이 경제적 이득으로 이어지는지에 대한 평가가 필요하다.
본 연구에서는 한국인의 심혈관질환 일차예방을 위한 am- lodipine과 atorvastatin의 단일 복합제 투여와 단일제 병용 투여를 비교한 경제성 평가를 시행하였다.
방 법
비용-효과 모형
본 연구는 고지혈증이 동반된 고혈압 환자 및 심혈관질환 위험인자 3개 이상의 고위험 환자군을 대상으로 하여, 심혈 관질환 일차예방을 위한 amlodipine과 atorvastatin의 치료 대안에 대한 비용-효과성을 평가하였다. 치료대안은 단일 복합제제 amlodipine/atorvastatin(Single pill amlodipine/
atorvastatin, 이하 SINGLE-PILL)과 amlodipine과 atorv- astatin의 단일제제 병용투여(Co-administration amlodipine and atorvastatin, 이하 TWO-PILLs)이다. 분석 방법은 경제 성평가 방법 중 비용-효과 분석을 이용하였고, 1000명을
cohort로 하여 cohort simulation 방법을 사용하였다.
본 연구에서 효과의 정의는 심혈관질환 발생의 1차 예방 환자 수이며, 이는 전체 코호트에서 심혈관질환 발생 환자를 뺀 나머지 환자 수로 하였다. 이때 심혈관질환의 정의는 본 연구의 효과값에 대한 자료원인 The lipid-lowering arm of the Anglo-Scandinavian Cardiac Outcomes(이하 ASCOT- LLA) trial13)에서 사용한 “Total cardiovascular events and procedures” 정의와 동일하며, 약제 투여 후 발생한 심장 및 혈관 관련된 모든 질환의 발생, 사망 및 관련 시술(proce- dures)을 의미한다. 두 치료 대안은 생물학적 동등성(bio- equivalence)이 입증되었으므로,11) 각 대안 간의 효과의 차이 는 복약순응도의 차이에 따라서만 달라지는 것으로 하였다.
복약순응의 수준은 복약순응(adherent)과 비순응(non-ad- herent)으로 구분하고, ‘복약순응’의 정의는 medicine pos- session ratio(이하 MPR) 혹은 percentage of day covered (이하 PDC) 기준으로 80% 이상인 경우로 하였고, ‘비순응’
은 80% 미만인 경우로 하였다. 비용의 정의는 심혈관질환 예방을 위해 시행되는 혈압 및 혈중 지질 조절에 있어서 1년 간 소요되는 의료비용으로 하였다.
이러한 분석을 통하여, 각 치료대안의 평균 비용-효과비 (average cost-effectiveness ratio, 이하 ACER)를 산출하여 비교하였다. ACER는 1명의 심혈관질환 예방을 위해 소요 되는 비용으로 정의하였다. 본 비용-효과 분석에 관한 기본 모형은 그림 1에 요약되었다.
자료원
본 연구에서는 앞서 언급한 환자군에서 amlodipine과 atorvastatin 병합 투여시의 심혈관질환 예방에 대한 효과값 으로 ASCOT-LLA Trial13)의 결과값을 각 대안에 동일하게 사용하였다. 각 치료대안의 복약순응 수준에 대한 환자 분포 (probability of adherence) 및 복약순응 수준에 따른 심혈관 질환 예방 효과의 차이에 대한 값의 검색은 체계적 문헌고 찰을 실시하였다. 자료의 검색은 pubmed를 검색원으로 하여 2013년 10월 30일에 실시하였다.
각 치료대안의 복약순응 수준에 대한 환자 분포의 확인을 위해 “(amlodipine AND atorvastatin) AND adherence”를 검색어로 하여 검색된 총 132개의 문헌 중 선정기준을 만족 하는 최종 2개의 문헌을 선정하였다. 이때 문헌 선정 기준은 1) amlodipine과 atorvastatin을 동시에 투여 받은 환자를 대 상으로, 2) SINGLE-PILL과 TWO-PILLs의 순응도의 차이 를 확인하였으며, 3) 순응도는 MPR 혹은 PDC의 형태로 80% 이상과 미만을 비교한 문헌으로 하였다.
복약순응 수준에 따른 효과 차이 확인을 위해 “(amlodip-
ine OR atorvastatin) AND adherence AND cardiovascular”
의 검색어로 문헌검색을 실시하였으나 적절한 문헌이 검색 되지 않아 검색어를 보다 확대하여 “(anti hypertensive drug OR lipid lowering drug) AND adherence AND cardiovas- cular”로 검색을 실시하였다. 검색된 558개의 문헌에 refer- ence 문헌 검색 4건을 포함하여 총 562개의 문헌 중 선정기 준을 만족하는 문헌 4건과, hand-search로 검색된 1건의 문 헌을 포함하여 총 5건의 문헌을 선정하였다. 이때 문헌 선정 기준은 1) 심혈관질환의 병력이 없는 환자를 대상으로, 2) amlodipine(or calcium channel blocker) or atorvastatin(or statin)을 사용하여, 3) 복약순응 수준에 따른 심혈관질환 발 생에 대해 odds ratio(이하 OR), hazard ratio(이하 HR), 혹 은 risk ratio(이하 RR)의 형태로 보고한 문헌이며, 4) 순응수 준은 MPR 혹은 PDC의 형태로 하여 80% 이상과 미만을 비 교한 문헌으로 하였다.
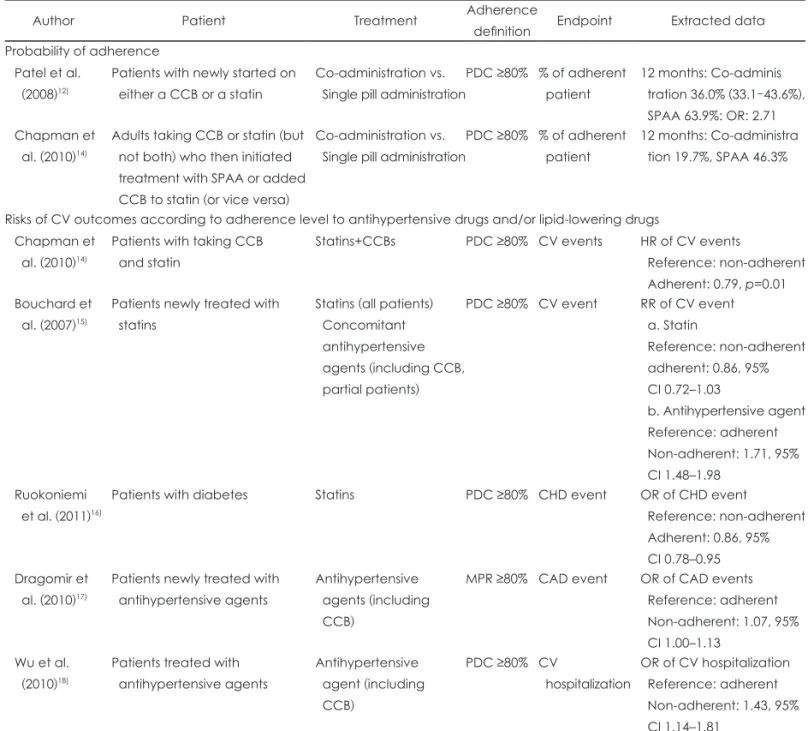
이상의 검색기준으로 최종 선정된 문헌은 각 치료대안의 복약순응 분포에 대한 문헌 2건, 순응 수준에 따른 효과 차 이에 대한 문헌 5건으로 표 1과 같으며, 최종 선정된 문헌들 에서 보고된 값들을 모두 모형에 반영하여 ACER의 범위를 확인하였다.
비용 추정에 포함된 항목은 약제비용이며, 다른 비용들은 두 치료대안에서 모두 같은 것으로 가정하여 본 연구의 분 석에서는 고려하지 않았다. 약제비용은 2014년 2월 기준으 로 건강 보험 약가를 이용하였으며, amlodipine 5 mg과 atorvastatin 10 mg의 오리지널 단일제제와 복합제제의 가 격을 적용하였다. 각 치료대안은 1일 1회 투여되는 것으로 하고, 복용법은 1년간 동일하게 약제 투여용량의 조절 없이 유지된다고 가정하였다.
분석 기간
본 연구는 혈압 및 혈중 지질농도 조절을 통한 심혈관질 환 예방을 위해 amlodipine과 atorvastatin 약물치료 시작 후 1년 동안의 평균 비용-효과 비를 분석하였다.
결 과
효 과
문헌에서 보고된 SINGLE-PILL과 TWO-PILLs의 복약 순응 환자 비율은 선정된 최종 2개의 문헌인 Patel 등12)의 문 헌에서 63.9% vs. 36.0%, Chapman 등14)의 문헌에서 46.3%
vs. 19.7%로 확인되었고, 순응한 환자비율을 이들 문헌의 결 과에 따라 2가지의 경우로 나누어 분석을 실시하였다.
ASCOT-LLA trial13)에서 보고된 amlodipine과 atrovas- tatin의 동시 투여시 심혈관질환 발생 환자수는 22.7 per 1000 patient-years였다. SINGLE-PILL과 TWO-PILLs는 생물학적 동등성이 입증되었으므로, 22.7 per 1000 patient- years를 각 치료 대안의 순응한 환자군에 모두 동일하게 적 용하였다. 문헌에서 보고된 복약순응 수준을 고려한 심혈관 질환 발생 위험도는 복약 순응도가 80% 이상인 경우, 80%
이하인 경우에 비해 HR 0.79,14) RR 0.82,15) OR 0.8616)으로 발 생 위험도를 낮추었고, 순응도가 80% 이하인 경우 80% 이 상인 경우보다 RR 1.71,15) OR 1.07,17) 1.4318)으로 심혈관질 환 발생 위험이 높았다. 이를 이용하여, 순응한 환자군에서 의 효과값으로부터 비순응 환자에서의 심혈관질환 발생 효 과값을 산출하면, 24.3~38.8 per 1000 patient-years였다(표 2). 1000명 cohort 모형에서 복약순응 환자 비율을 고려하여 심혈관질환 1차 예방환자수를 산출하면 그림 2와 같은 효과 의 분포를 나타내었다. 복약 순응도 80% 이상의 환자가 Fig. 1. Cost-effectiveness model. CVD: cardiovascular disease.
Adherence: key factor affecting on outcomes/input Probability of adherence (P)
Alternatives Administration types
Adherence P1
Drug cost C1 CVD prevention
E1
Adherence P2
Drug cost C3 CVD prevention
E1 Non-adherence
1-P1
Drug cost C2 CVD prevention
E2
Non-adherence 1-P2
Drug cost C4 CVD prevention
E2 Outcomes (effectiveness)
CVD prevention (E)=E1+E2 Input Drug cost (C)=C1 (3)+C2 (4)
Average cost-effectiveness ratio (ACER)=C/E
Administration of amlodipine & atorvastatin
SINGLE-PILL
ACER of SINGLE-PILL
TWO-PILLs
ACER of TWO-PILLs vs.
vs.
SINGLE-PILL과 TWO-PILLs에서 각각 63.9% vs. 36.0%
인 경우, 심혈관질환 예방 환자수는 SINGLE-PILL에서 1000명당 총 971.5~976.7명이며, 이는 복약 순응도가 80%
이상인 639명 중 624.5명, 80% 미만인 361명 중 347.0~
352.2명에서 심혈관질환 발생을 예방한 효과이다. TWO- PILLs의 경우 1000명 중 총 967.0~976.3명의 심혈관질환 예 방효과가 있고, 순응도가 80% 이상인 360명의 환자 중 351.8 명, 80% 미만인 640명의 환자 중 615.2~624.5명의 심혈관질 환 예방효과가 있다. 복약 순응도 80% 이상의 환자 분포가 SINGLE-PILL과 TWO-PILLs에서 각각 46.3% vs. 19.7%로 더 낮은 경우 심혈관질환 예방 효과는 감소하며, SINGLE-
PILL에서 1000명당 968.6~976.5명, TWO-PILLs에서 1000 명당 964.4~976.1명이 예방되었다(표 2). 즉, SINGLE-PILL 의 경우 복약 순응도의 개선으로 TWO-PILLs에 비하여 1000명당 0.4~4.5명의 추가적 심혈관질환 예방 효과를 기대 할 수 있다.
비 용
Amlodipine 5 mg과 atorvastatin 10 mg의 약가는 오리지 널 단일제제가 각각 367원, 663원이고 복합제제가 733원으 로, SINGLE-PILL과 TWO-PILLs 형태로 투약시 1년간의 약제비 산정치는 TWO-PILLs가 375950원, SINGLE-PILL
Table 1. Sources of included data in the model from the systematic review
Author Patient Treatment Adherence
definition Endpoint Extracted data Probability of adherence
Patel et al.
(2008)12)
Patients with newly started on either a CCB or a statin
Co-administration vs.
Single pill administration
PDC ≥80% % of adherent patient
12 months: Co-adminis tration 36.0% (33.1–43.6%), SPAA 63.9%: OR: 2.71 Chapman et
al. (2010)14)
Adults taking CCB or statin (but not both) who then initiated treatment with SPAA or added CCB to statin (or vice versa)
Co-administration vs.
Single pill administration
PDC ≥80% % of adherent patient
12 months: Co-administra tion 19.7%, SPAA 46.3%
Risks of CV outcomes according to adherence level to antihypertensive drugs and/or lipid-lowering drugs Chapman et
al. (2010)14)
Patients with taking CCB and statin
Statins+CCBs PDC ≥80% CV events HR of CV events
Reference: non-adherent Adherent: 0.79, p=0.01 Bouchard et
al. (2007)15)
Patients newly treated with statins
Statins (all patients) Concomitant antihypertensive agents (including CCB, partial patients)
PDC ≥80% CV event RR of CV event a. Statin
Reference: non-adherent adherent: 0.86, 95%
CI 0.72–1.03
b. Antihypertensive agent Reference: adherent Non-adherent: 1.71, 95%
CI 1.48–1.98 Ruokoniemi
et al. (2011)16)
Patients with diabetes Statins PDC ≥80% CHD event OR of CHD event Reference: non-adherent Adherent: 0.86, 95%
CI 0.78–0.95 Dragomir et
al. (2010)17)
Patients newly treated with antihypertensive agents
Antihypertensive agents (including CCB)
MPR ≥80% CAD event OR of CAD events Reference: adherent Non-adherent: 1.07, 95%
CI 1.00–1.13 Wu et al.
(2010)18)
Patients treated with antihypertensive agents
Antihypertensive agent (including CCB)
PDC ≥80% CV
hospitalization
OR of CV hospitalization Reference: adherent Non-adherent: 1.43, 95%
CI 1.14–1.81
CCB: calcium channel blocker, PDC: proportion of day covered, MPR: medication possession ratio, CV: cardiovascular, CAD:
coronary artery disease, RR: risk ratio, HR: hazard ratio, OR: odds ratio, CI: confidence interval, CHD: coronary heart disease, SPAA: single-pill amlodipine/atorvastatin
Table 2. Effectiveness of cardiovascular disease prevention in accordance with medication adherence of each alternative Alternatives
Adherence in cohort Efficacy (per 1000 patient-years) Effectiveness in cohort
Total effectiveness Adherence Non-
adherence CV event rate
in adherence CV event rate
in non-adherence CV prevention
in adherence CV prevention of non-adherence
Single-Pill* 639 361 22.7 24.3‡ 624.5 352.2 976.7
26.3§ 351.5 976.0
26.4∥ 351.5 976.0
28.7¶ 350.6 975.1
32.1** 349.4 973.9
38.8†† 347.0 971.5
Two-Pills* 360 640 22.7 24.3 351.8 624.5 976.3
26.3 623.2 975.0
26.4 623.1 974.9
28.7 621.6 973.4
32.1 619.4 971.3
38.8 615.2 967.0
Single-Pill† 463 537 22.7 24.3 452.5 524.0 976.5
26.3 522.9 975.4
26.4 522.8 975.3
28.7 521.6 974.1
32.1 519.7 972.2
38.8 516.2 968.6
Two-Pills† 197 803 22.7 24.3 192.5 783.5 976.1
26.3 781.9 974.4
26.4 781.8 974.3
28.7 779.9 972.5
32.1 777.2 969.7
38.8 771.8 964.4
Unit: N of patients. Number of cohort: 1000, Data source of the probability of adherence: *Patel et al. (2008),12)†Chapman et al.
(2010),14) Data sources for calculation of CV event rate in non-adherence: ‡Dragomir et al. (2010),17)§Ruokoniemi et al. (2011),16)∥Bo- uchard et al. (2007),15)¶Chapman et al. (2010),14) **Wu et al. (2010),18)††Bouchard et al. (2007).15) CV: cardiovascular
Fig. 2. Effectiveness of cardiovascular disease prevention in the cohort according to the adherence of each alternative. Unit: number of patients. CVD: cardiovascular disease, OR: odds ratio, RR: risk ratio, HR: hazard ratio, adh.: adherence.
Effectiveness in cohort 978.0
976.0 974.0 972.0 970.0 968.0 966.0
CVD prevention
% of adh. from CV event
adh. vs. non adh. OR: 1.0717) OR: 0.8616) RR: 0.8615) HR: 0.7914) OR: 1.4318) RR: 1.7115)
Patel et al. (2008)12) Single-Pill 976.7 976.0 976.0 975.1 973.9 971.5
Two-Pills 976.3 975.0 974.9 973.4 971.3 967.0
Chapman et al. (2010)14) Single-Pill 976.5 975.4 975.3 974.1 972.2 968.6
Two-Pills 976.1 974.4 974.3 972.5 969.7 964.4
이 267545원이다.
환자들의 복약 순응도는 복약순응 수준의 범위에서 평균 상위 80% 수준에 분포하는 것으로 가정하여 약제비를 적용 하였다. 즉, 본 연구에서 정의한 기준에 따라 복약순응 환자 의 경우 복약 순응도가 PDC(or MPR) 80~100%이므로 365 일 중 292~365일은 약제를 복용한 것이고, 범위내 상위 80%
수준인 평균 약 350일을 복용한 것이다. 비순응 환자는 PDC(or MPR) 0~79%의 범위에 속하므로 0~291일의 범위 내에서 약제를 복용한 것이고, 범위내 상위 80%인 평균 약 232일을 복용한 것이다. 이러한 가정으로 1명당의 평균 약 제비는 SINGLE-PILL로 복용하였을 때 복약순응 환자의 경우 256843원, 비순응 환자의 경우 169088원이고, TWO- PILLs로 복용하였을 때 복약순응 환자의 경우 360912원, 비 순응 환자의 경우 237600원으로 복약순응에 비하여 복약 비 순응의 경우 1인당 평균 약제비는 감소하였다(표 3).
1000명 cohort 모형에서 복약 순응도 80% 이상의 환자가 SINGLE-PILL과 TWO-PILLs에서 각각 63.9% vs. 36.0%
인 경우, SINGLE-PILL로 1년간을 투약한 경우의 총 약제 비는 1000명당 225163732원이고, 이 중 순응도 80% 이상 환 자의 약제비가 164122805원으로 비순응 환자의 약제비 61040927원보다 더 많았다. TWO-PILLs로 1년간 투여한 경 우 총 약제비는 281992576원이고, 순응한 환자들의 총 약제 비는 129928320원, 비순응 환자들의 총 약제비는 152064256 원이었다. 복약 순응도 80% 이상의 환자 분포가 46.3% vs.
19.7%로 더 낮은 경우는 SINGLE-PILL에서 209718894원, TWO-PILLs에서 261892785원으로, 복약순응 환자 분포가 상대적으로 높을 때보다 총 약제비는 감소하였으나, SIN- GLE-PILL과 TWO-PILLs 간의 약제비 차이는 비슷한 수 준으로 TWO-PILLs에서 높았다(표 3).
비용-효과비
본 연구에서는 효과단위당 비용 즉, 평균 비용-효과값 (ACER)을 1명의 심혈관질환 예방을 위해 발생하는 비용으 로 정의하였다. 따라서, ACER값이 작을수록 심혈관질환 예
방에 효율적인 대안임을 뜻한다.
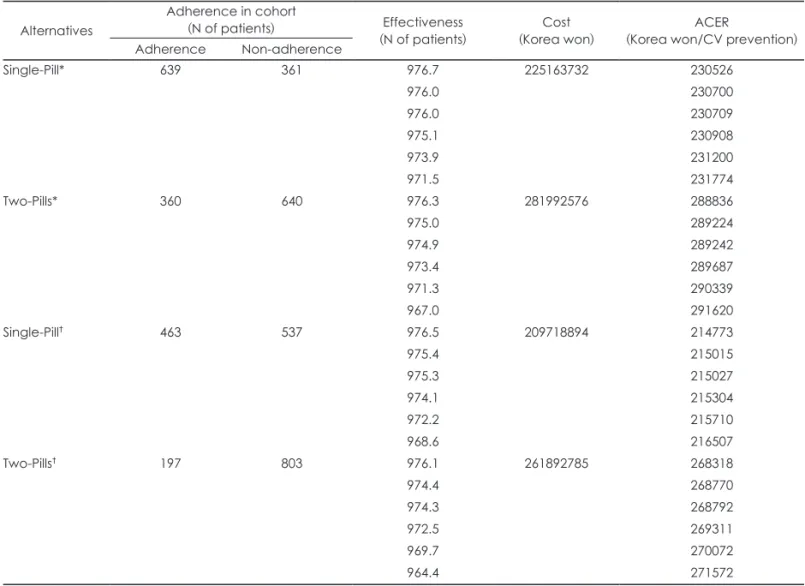
표 4에서 확인할 수 있듯이 SINGLE-PILL의 ACER값은 효과값의 범위에 따라 214773~231774원이고, TWO-PILLs 의 ACER값은 268318~291620원이므로 심혈관질환 1건의 예방을 위한 평균 약제비는 SINGLE-PILL의 형태로 투여 시 TWO-PILLs의 형태로 투여했을 때보다 약 20%의 비용 절감 효과를 나타내어 SINGLE-PILL이 효율적 대안으로 확인되었다. 복약 불순응 환자의 경우 복약하지 않는 만큼의 약제비가 감소할 수 있으나, SINGLE-PILL의 TWO- PILLs 대비한 복약 순응도의 개선은 1000명당 0.4~4.5명의 심혈관질환 예방에 대한 효과 개선을 보였고, 약제의 가격 또한 저렴하여 총 약제비가 TWO-PILLs로 투여할 때보다 저렴한 것으로 나타나 효과 단위당 비용이 낮게 나타났다.
고 찰
본 연구에서는 고지혈증이 동반된 고혈압 환자 및 위험인 자 3개 이상의 심혈관질환 고위험 환자군을 대상으로 심혈 관질환의 일차예방을 위해 사용되는 단일복합제 amlodip- ine/atorvastatin의 순응도 개선에 따른 경제성을 단일제제 로 병용투여 하는 치료대안과 비교하여 평가하였다. 비용측 면으로는 1년 동안의 약제비를 적용하고, 효과로는 심혈관 질환의 1차 예방 환자 수를 적용하여 효과를 얻기 위해 투입 되는 평균 약제비용을 cohort-simulation을 통해 비교분석 하였다. 본 연구의 결과, 심혈관질환의 일차 예방을 위해서 는 SINGLE-PILL로 투여하는 것이 TWO-PILLs로 투여하 는 것에 비하여 비용-효과적인 대안임이 확인되었다.
심혈관질환의 예방을 위해서는 multi-factorial approach 가 추천되고 있다.19) 심혈관질환의 위험인자들은 복합적으 로 동반되는 경우가 많은데 여러 위험인자를 동시에 조절하 여 심혈관질환의 발생 위험을 줄이고자 하는 것이다. 고혈압 과 고지혈증은 흔히 동반되는 심혈관질환 위험인자들로, 3-hydroxy-3-methylglutaryl-CoA reductase inhibitor (statins)가 환자 특성에 맞춘 고혈압제와 함께 일차 치료제
Table 3. Drug cost in accordance with medication adherence of each alternative Alternatives
Adherence in cohort (N) Cost (per patient) Cost in cohort
Total cost Adherence Non-
adherence Drug cost when
adherent Drug cost when
non-adherent Drug cost in
adherence Drug cost in non-adherence
Single-Pill* 639 361 256843 169088 164122805 61040927 225163732
Two-Pills* 360 640 360912 237600 129928320 152064256 281992576
Single-Pill† 463 537 256843 169088 118918402 90800492 209718894
Two-Pills† 197 803 360912 237600 71099664 190793121 261892785
Unit: Korea won. Number of cohort: 1000, Data source of the probability of adherence: *Patel et al. (2008),12)†Chapman et al.
(2010).14)
로 권고되고 있다.2) 특히, statin 중 atorvastatin을 amlodip- ine에 기반하여 사용하는 것은 atorvastatin을 사용하지 않거 나 다른 계열 약제인 atenolol을 기반하여 사용하였을 때보 다 심혈관질환의 예방에 있어 더 효과적일 뿐만 아니라, 효 율적인 치료대안임이 선행 연구에서 확인되었다.13,20)
Fixed dose single-pill combination amlodipine/atorvas- tatin은 long-acting calcium channel antagonist amlodipine 과 HMG-CoA reductase inhibitor atorvastatin의 복합제제 로, 환자의 복약 편의성을 고려하여 소개된 약이다. Pill 개수 의 감소는 복약 순응도의 개선효과로 이어져, 단일 복합제 투 여시의 복약순응 환자의 비율이 단일제제 병용 투여시보다 약 2배 정도 많은 것으로 보고되어 큰 차이를 보인다.12,14) 복 약 순응도의 차이는 치료 결과에도 영향을 미치게 되어 주요 심혈관질환 위험인자 조절에 실패하게 되고, 결국 심혈관질 환의 발생을 초래하게 된다. 실제로 고혈압 및 고지혈증의 치 료약제 복용에 있어 불순응 환자들의 경우, 순응 환자에 비하 여 심혈관질환 발생 위험이 증가됨이 보고된 바 있다.14-18)
심혈관질환 3개 이상의 고위험 고혈압 환자에서 amlodip- ine을 기반으로 하여 atorvastatin을 사용하면 22.7 per 1000 person-years의 심혈관질환 예방 효과가 있다.13) 이때, SIN- GLE-PILL로 투여할 때의 순응도의 개선은 TWO-PILLs와 비교하였을 때 1000명당 0.4~4.5명의 심혈관질환 예방을 추 가적으로 나타내는 것으로 본 연구의 모형 분석 결과 확인되 었다. 비용 측면에서는 TWO-PILLs로 복용할 경우 복약 순 응도의 감소로 1년간 복용하게 되는 약의 수가 줄어 들게 되 어 약제 비용의 감소를 가져올 수 있겠지만 이는 SINGLE- PILL 복용시의 약제 가격과 효과 증가분을 상쇄하지는 못하 는 것으로 나타났다. 결과적으로 SINGLE-PILL로 투여하 였을 때의 심혈관질환 예방 1건당 소요되는 약제비는 214773~231774원이었고, TWO-PILLs로 투여하였을 때에 는 268318~291620원으로 나타나 SINGLE-PILL로 투여하 였을 때 약 20%의 비용 절감을 나타내었다.
한국과는 비용이 상이한 외국의 비용-효과 연구결과를 한국인의 치료대안 결정시에 직접적으로 반영하기는 어렵
Table 4. Average cost-effective ratios Alternatives
Adherence in cohort
(N of patients) Effectiveness
(N of patients) Cost
(Korea won) ACER
(Korea won/CV prevention) Adherence Non-adherence
Single-Pill* 639 361 976.7 225163732 230526
976.0 230700
976.0 230709
975.1 230908
973.9 231200
971.5 231774
Two-Pills* 360 640 976.3 281992576 288836
975.0 289224
974.9 289242
973.4 289687
971.3 290339
967.0 291620
Single-Pill† 463 537 976.5 209718894 214773
975.4 215015
975.3 215027
974.1 215304
972.2 215710
968.6 216507
Two-Pills† 197 803 976.1 261892785 268318
974.4 268770
974.3 268792
972.5 269311
969.7 270072
964.4 271572
Number of cohort: 1000, Data source of the probability of adherence: *Patel et al. (2008),12)†Chapman et al. (2010).14) CV: cardio- vascular, ACER: average cost-effectiveness ratio
고, 더불어 현재까지 한국인을 대상으로 하여 single-pill amlodipine/atorvastatin이 심혈관질환 예방이라는 최종 결 과지표에 경제적 이득을 보이는가 하는 부분의 연구는 매우 드물어, 이에 대한 연구가 필요하였다. Liew 등21)의 연구에서 는 single-pill amlodipine/atorvastatin의 한국인 심혈관질환 예방에 대해 비용-효과성을 분석하여 경제적 이득의 결과 를 얻었으나, 비교대상이 특정 약제로 명시되지 않았었다.
본 연구는 국내에서 심혈관질환 예방을 위해 흔히 사용하는 amlodipine과 atorvastatin을 SINGLE-PILL로 투여하는 치 료대안과 TWO-PILLs로 동시에 투여하는 치료대안을 비교 하였으므로, 의료진이 임상에서 해당 약제의 처방시에 실제 로 고려하는 치료대안들의 경제성을 평가한 최초의 연구이 다. 뿐만 아니라, 치료의 효과에 영향을 미칠 수 있는 환자 측면에서의 주요 요소인 복약 순응도를 모델에 반영하여 비 용-효과성을 평가하였으므로, 본 연구에 포함된 환자군의 심혈관질환 예방을 목표로 하는 효율적 치료약제 선정시 판 단의 근거를 제공할 것으로 사료된다.
본 연구는 다음과 같은 제한점을 가지고 수행되었기 때문 에 결과를 해석할 때는 주의가 필요하다. 첫째, 분석에 포함 된 복약순응에 대한 확률값 및 순응도에 따른 심혈관질환 예방에 대한 효과값이 각기 다른 문헌에서 추출되어 정확한 차이를 추론하는 데 한계가 있다. 이에 현재 가용한 모든 관 련 데이터를 체계적 문헌고찰을 통해 검색하여 모델에 모두 반영하여, ACER를 존재 가능한 범위로 제시함으로써 그 불 확실성을 최소화 하였다. 둘째, 본 연구에 사용된 모델에서 는 각 치료대안에 대한 복약 순응도를 ‘순응’과 ‘불순응’ 두 개의 그룹으로만 반영하였기 때문에, 상이한 순응도를 가진 환자가 한 그룹 안에 존재함으로써 비용이 과소 혹은 과대 추정 되었을 가능성이 있다. 그러나, 두 치료대안 모두에 동 일하게 적용된 가정이므로, 오류 추정된 부분은 일정 부분 상쇄되어 분석 결과를 해석하는 데 큰 영향을 미치지 않았 을 것으로 사료된다. 셋째, 효과와 관련된 자료들이 모두 외 국인 대상인 문헌으로부터 값을 추출하여 사용하였으므로 국내의 현실을 정확히 반영하는 데에는 한계가 있고, 마지막 으로 비용에 약제비용만이 포함되어 심혈관질환 예방에 필 요한 총비용으로는 해석하기 어렵다. 향후 해당 약제의 사용 에 있어 한국인 환자의 순응도에 따른 심혈관질환 예방 효 과값 및 직/간접 의료비를 모두 반영하여 individual model 을 적용한 추가 연구가 요구된다.
결 론
고지혈증이 동반된 고혈압 환자 및 위험인자 3개 이상의
심혈관질환 고위험 환자군에게 심혈관질환의 일차예방을 위한 amlodipine과 atorvastatin 사용시, 단일복합제(SIN- GLE-PILL)의 투여는 다빈도로 처방되는 단일제제 병합 투 여(TWO-PILLs)보다 비용-효과적 대안임이 확인되었고, 이는 향후 해당 환자의 심혈관질환 1차 예방을 위한 적절한 치료 대안 선택시 의미 있는 정보로 활용될 수 있을 것이다.
REFERENCES
1) Asia Pacific Cohort Studies Collaboration. Joint effects of systolic blood pressure and serum cholesterol on cardiovascular disease in the Asia Pacific region. Circulation 2005;112:3384-3390.
2) Mancia G, De Backer G, Dominiczak A, Cifkova R, Fagard R, Ger- mano G. 2007 Guidelines for the management of arterial hyperten- sion: The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J 2007;28:1462-1536.
3) Johnson ML, Pietz K, Battleman DS, Beyth RJ. Therapeutic goal at- tainment in patients with hypertension and dyslipidemia. Med Care 2006;44:39-46.
4) Cowie MR. Simultaneous treatment of hypertension and dyslipidae- mia may help to reduce overall cardiovascular risk: focus on amlodip- ine/atorvastatin single-pill therapy. Int J Clin Pract 2005;59:839-846.
5) Cramer JA. Partial medication compliance: the enigma in poor medi- cal outcomes. Am J Managed Care 1995;1:167-174.
6) Osterberg L, Blaschke T. Adherence to medication. N Engl J Med 2005;353:487-497.
7) Chapman RH, Benner JS, Petrilla AA, Tierce JC, Collins SR, Battle- man DS. Predictors of adherence with antihypertensive and lipid- lowering therapy. Arch Intern Med 2005;165:1147-1152.
8) Dezii CM. A retrospective study of persistence with single-pill com- bination therapy vs. concurrent two-pill therapy in patients with hy- pertension. Manag Care 2000;9(9 Suppl):2-6.
9) Dezii CM. Medication noncompliance: what is the problem? Manag Care 2000;9(9 Suppl):7-12.
10) Simpson SH, Eurich DT, Majumdar SR, Padwal RS, Tsuyuki RT, Varney J, et al. A meta-analysis of the association between adherence to drug therapy and mortality. BMJ 2006;333:15.
11) Chung M, Calcagni A, Glue P, Bramson C. Bioavailability of amlo- dipine besylate/atorvastatin calcium combination tablet. J Clin Phar- macol 2006;46:1030-1037.
12) Patel BV, Leslie RS, Thiebaud P, Nichol MB, Tang SS, Solomon H, et al. Adherence with single-pill amlodipine/atorvastatin vs a two-pill regimen. Vasc Health Risk Manag 2008;4:673-681.
13) Sever PS, Poulter NR, Dahlof B, Wedel H; ASCOT Investigators.
Antihypertensive therapy and the benefits of atorvastatin in the An- glo-Scandinavian Cardiac Outcomes Trial: lipid-lowering arm exten- sion. J Hypertens 2009;27:947-954.
14) Chapman RH, Yeaw J, Roberts CS. Association between adherence to calcium-channel blocker and statin medications and likelihood of cardiovascular events among US managed care enrollees. BMC Car- diovasc Disord 2010;10:29.
15) Bouchard MH, Dragomir A, Blais L, Bérard A, Pilon D, Perreault S.
Impact of adherence to statins on coronary artery disease in primary prevention. Br J Clin Pharmacol 2007;63:698-708.
16) Ruokoniemi P, Korhonen MJ, Helin-Salmivaara A, Lavikainen P, Jula A, Junnila SY, et al. Statin adherence and the risk of major coro- nary events in patients with diabetes: a nested case-control study. Br J Clin Pharmacol 2011;71:766-776.
17) Dragomir A, Côté R, Roy L, Blais L, Lalonde L, Bérard A, et al. Im- pact of adherence to antihypertensive agents on clinical outcomes and hospitalization costs. Med Care 2010;48:418-425.
18) Wu PH, Yang CY, Yao ZL, Lin WZ, Wu LW, Chang CC. Relation- ship of blood pressure control and hospitalization risk to medication adherence among patients with hypertension in Taiwan. Am J Hyper- tens 2010;23:155-160.
19) Wald NJ, Law MR. A strategy to reduce cardiovascular disease by more than 80%. BMJ 2003;326:1419.
20) Chapman RH, Kowal SL, Cherry SB, Ferrufino CP, Roberts CS,
Chen L. The modeled lifetime cost-effectiveness of published adher- ence-improving interventions for antihypertensive and lipid-lowering medications. Value Health 2010;13:685-694.
21) Liew D, Park HJ, Ko SK. Results of a Markov model analysis to as- sess the cost-effectiveness of a single tablet of fixed-dose amlodipine and atorvastatin for the primary prevention of cardiovascular disease in Korea. Clin Ther 2009;31:2189-2203; discussion 2150-2151.