Although plane radiography is the first step for mak- ing the diagnosis of small bowel obstruction, its accura- cy for determining the presence of obstruction is only 46-80% (1-7). CT currently has an essential role in di- agnosing small bowel obstruction. It has a high sensitivi- ty of 94%-100% and an accuracy of 90%-95% (1, 3, 8).
In addition, the recent evolution of conventional CT into MDCT has brought about great advances in the evalua- tion of the small bowel. With the use of the 3-dimen-
sional imaging technique, it is possible to reconstruct the VR, MIP or MPR images from the volume data. In this article, we illustrate and discuss the usefulness of the multiplanar MDCT images for diagnosing the site of bowel obstruction and characterizing the specific causes of small bowel obstruction. In addition, we also illus- trate the findings of complicated loops due to small bow- el obstruction.
Scan parameters of the MDCT Examination
A 16-detector row spiral CT scanner (Sensation 16;
Siemens Medical Systems, Erlangen, Germany) with a gantry rotation time of 0.5 seconds was used at our insti- tute for the abdominal examinations. All the patients were placed in the supine position on the CT table. The acquisition volume included the whole abdomen from
Evaluation of Small Bowel Obstruction Using Multidetector Computed Tomography (MDCT)
1Jee Hye Lee, M.D., Soon-Young Song, M.D., On Koo Cho, M.D., Byung Hee Koh, M.D., Yongsoo Kim, M.D.2
1Department of Radiology, Hanyang University College of Medicine, Hanyang University Hospital, Korea
2Department of Radiology, Hanyang University College of Medicine, Hanyang University Kuri Hospital, Korea
Received September 13, 2007 ; Accepted November 1, 2007
Address reprint requests to : Soon-Young Song, M.D., Department of Radiology, Hanyang University College of Medicine, Hanyang University Hospital, 17 Haengdang-dong, Seongdong-gu, Seoul 133-792, Korea Tel. 82-2-2290-9160 Fax. 82-2-2293-2111
E-mail: [email protected]
Small bowel obstruction is a relatively common clinical condition and its diagnosis is based on the clinical signs, the patient’s history and the radiologic findings. For a pa- tient with suspected small bowel obstruction, it is essential to determine the site, loca- tion and cause of obstruction for the appropriate management. Because of the poor ac- curacy of plain radiography, computed tomography (CT) now has an essential role to diagnose bowel obstruction. With the recent evolution of conventional CT into multi- detector computed tomography (MDCT), it is possible to obtain cross sectional images with high spatial resolution and different post-processes can be done, such as obtain- ing the volume rendering (VR), maximum intensity projection (MIP), or multiplanar reformatted (MPR) images from the volume data. In this article, we illustrate and dis- cuss the utility of the multiplanar images of MDCT for diagnosing the sites, causes and complications of small bowel obstruction.
Index words :Intestine, small intestinal obstruction
Tomography, spiral computed, multi-detector Multiplanar images
Imaging, three-dimensional
the dome of the diaphragm to the lower margin of the symphysis pubis. An 18-gauge intravenous cannula was inserted into a vein in the antecubital fossa, forearm or wrist. Scanning of the abdomen was performed after in- travenously injecting 2 mg/kg of contrast medium (io- promide [Ultravist 370]; Schering, Berlin, Germany) with an automatic power injector at a flow rate of 2.5- 3.0 mL/sec. for a total of 100-120 mL. The scan delay time was determined by the automatic bolus tracking method. The region of interest (R.O.I.) was positioned at the descending aorta at the level of the diaphragm. The
CT scan for the hepatic arterial-phase images was start- ed 8 seconds after the attenuation reached 150 H.U. An additional CT scan for the portal-phase images was start- ed 60 seconds after starting the contrast injection. The CT scan was done during a breath holding at the end of inspiration. The CT examination was performed by us- ing 16×1.5-mm collimation and a table feed rate of of 24 mm per gantry rotation. The X-ray tube voltage was 120 kV and amperage was 140 mAs. The volume data of both the arterial and portal-phased scans was recon- structed at a 2-mm thickness and with a 1-mm interval.
A B
C D
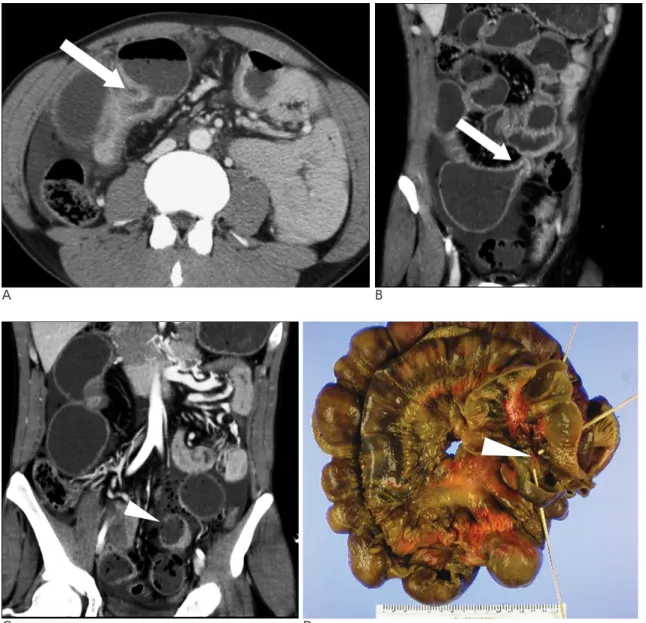
Fig. 1. A-D. Small bowel perforation in a 50 year-old male patient with advanced Crohn’s disease.
A. The axial CT scan shows marked dilatation of the small bowel loops and multifocal mural thickening. There are multiple foci of extraluminal air suggesting intestinal perforation (not seen). An abrupt change of caliber is noted (arrow).
B, C. The coronal reformatted images also easily demonstrate the site of obstruction with an abrupt change of caliber (arrow).
Multifocal extraluminal air bubbles are noted in the peritoneal cavity. There is a well-demonstrated site of perforation (arrow- head).
D. The gross specimen shows strangulated bowel loops and the site of perforation (arrowhead).
Image Interpretation
The volume data of the whole abdomen was acquired during a single breath hold for all the patients who un- derwent abdominal CT for the evaluation of small bow- el obstruction. The axial images of both the portal and arterial phases and the coronal image of the arterial phase were reformatted for routine study. We acquired additional MPR images at various angles and the curved MPR images from the volume data with using PC-based 3-dimensional software (Rapidia 2.8; InfinitⓇ, Seoul, Korea).
Classifying the Causes of Small Bowel Obstruction
The causes of small bowel obstruction can be classi- fied in two major categories, that is, the intrinsic and ex- trinsic causes. The intrinsic causes include inflammato- ry disease and neoplastic disease. Other conditions such as an intraluminal bezoar or a foreign body can also cause obstruction. The extrinsic extraluminal patholo- gies can result in small bowel obstruction. Adhesion and hernia are seen frequently. Although other conditions such as superior mesenteric artery (SMA) syndrome are infrequent, it can be a cause of duodenal obstruction.
Complicated cases such as strangulation, closed loop ob- struction and afferent loop syndrome are classified in the third category of the complicated small bowel ob- struction.
Intrinsic Causes
Inflammatory diseases Crohn’s disease
Crohn’s disease is an idiopathic inflammatory disease that can affect any part of the gastrointestinal tract from the mouth to the anus. The small bowel is the major site of involvement. Small bowel wall thickening and lumi- nal narrowing may be the common findings. The in- flamed mucosa and serosa may be markedly enhanced, and the intensity of enhancement correlates with the clinical activity of the disease. Mural stratification disap- pears during the chronic phase, so that the affected bow- el wall typically has homogeneous attenuation at CT (2, 9). In the advanced or stenotic phase of Crohn’s disease, the patients frequently present with recurrent episodes of partial small bowel obstruction associated with stric- ture. Dilated small bowel loops with an abrupt change in caliber can be detected on the routine axial CT images (Fig. 1A) (2). The reformatted images can demonstrate the full-length of the obstruction site (Fig. 1B). Severe obstruction can sometimes lead to perforation of the small bowel, which requires emergency surgical inter- vention (Fig. 1C). MDCT may be a useful tool not only for diagnosing the level and cause of obstruction, but al- so for detecting the site of perforation (Fig. 1A to 1D).
Intestinal tuberculosis
Even though Mycobacterium tuberculosis can involve any part of the gastrointestinal tract, the ileocecal region
A B C
Fig. 2. A-C. Intestinal tuberculosis with focal stricture in a 65 year-old female patient.
A, B. The slab VR images of CT shows a dilated jejunal loop, and note the abrupt change of caliber (arrow).
C. The curved MPR image shows focal bowel wall thickening that is suggestive of inflammatory lesion (arrowhead).
is the most common site of involvement for tuberculosis of the gastrointestinal tract. Intestinal tuberculosis may cause stricture of the small bowel and subsequent ob- struction. The gross morphologic features of this patho- logic process have been well evaluated with CT (9).
When the inflammation is mild, CT demonstrates only slight, symmetric mural thickening and a few small re- gional nodes. When the pathologic process is severe and advanced, then the more characteristic abnormalities are evident. Characteristically, the CT findings include asymmetric thickening of the ileocecal valve and the medial wall of the cecum, with an exophytic extension that engulfs the terminal ileum. Massive lym- phadenopathy can be combined with this, and the lym- phadenopathy shows central areas of low attenuation (10, 11). The cecum becomes conical, shrunken and re- tracted out of the iliac fossa due to fibrosis within the mesocolon (12). Symmetric annular stenosis and ob- struction associated with shortening, retraction and pouch formation may be seen (Fig. 2A and 2C) (13).
Using MDCT, the 3D data sets with using the volume rendering technique can be applied for the evaluation of
bowel disease with the advantage of an overlap-free dis- play of such individual structures as the bowel, vessels and solid organs. The images of the small bowel can be reconstructed in a pattern resembling enteroclysis and this makes the pathologic segment more easily de- tectible (Fig. 2A to 2C).
Parasitic infestation
Parasites can be a rare intrinsic inflammatory cause of small bowel obstruction. The possible organisms that can infest the bowel are Ascaris lumbricoides, hook- worm (Ancylostoma duodenale and Necator ameri- canus), tapeworm (Diphyllobothrium latum, Taenia solium), Strongyloides stercoralis, Giardia lamblia and the Anisakis species. When adult Ascaris are present in large numbers, they may form an intertwined bolus, causing intestinal obstruction (14).
Nematodes of the Anisakis genera inhabit the intesti- nal tracts of marine mammals and piscivorous birds.
Humans are infected by eating raw or insufficiently cooked fish or squid. Several types of lesions can be pro- duced by the Anisakis larvae that have burrowed into
A B
C
Fig. 3. A-C. Small bowel obstruction due to anisakiasis in a 28 year-old male.
A. An axial CT scan shows focal wall thickening of the ileal loop (arrow).
B. The curved MPR image shows focal concentric wall thicken- ing at the site of obstruction (arrow).
C. The surgical specimen excised from the site of obstruction shows inflamed mucosa. There is a larva of the Anisakis species (arrow).
the wall of the intestine. Ulcers, abscesses, eosinophilic granuloma and perforations are possible findings. CT may reveal bowel wall thickening, mucosal edema, stricture and occasionally an inflammatory mass effect and all this can be a cause of small bowel obstruction (Fig. 3A to 3C) (15, 16). Ascites may accompany the in- testinal changes.
The curved multi-planar reformatted images are ex- tracted by defining a path on the key images. It is possi- ble to visualize the whole length of the pathologic bowel segment and the exact location of obstruction in a single image (Fig. 3B).
Non-specific inflammation
Other than Crohn’s disease or tuberculosis, there are non-specific inflammatory conditions that may involve the small bowel and cause obstruction, and the cause or pathogen is not usually recognized (2). This may resolve spontaneously with conservative care and without the
physician arriving at a specific diagnosis.
Neoplastic Diseases
Small bowel neoplasms are another rare cause of ob- struction. Adenocarcinoma of the small bowel is seen more frequently in the duodenum and proximal je- junum than in the ileum (18, 19). Tumor is usually de- tected at an advanced stage. Small bowel obstruction secondary to adenocarcinoma usually manifests on CT as mural thickening with abrupt luminal narrowing at the transition zone. Usually only a short segment is in- volved. CT may provide unique information about tu- mor extension and local or distant metastases (Fig. 4A to 4C). The oblique MPR image can be reformatted when the reviewers rotate the basic axial, coronal and sagittal images in the 3D program. Using this easy technique, the pathologic bowel segment can be demonstrated along its axis (Fig. 4B).
Other types of small bowel neoplasm, such as lipoma,
A
C
B
Fig. 4. A-C. Small bowel obstruction due to jejunal adenocarci- noma in a 59 year old male patient.
A. The axial CT scan shows an abrupt caliber change of the di- lated small bowel loop (arrow).
B. The curved MPR image shows the site of obstruction with an abrupt caliber change. The narrowed segment shows focal ec- centric wall thickening, suggesting the possibility of malignancy (arrow).
C. The cut surface shows short segmental stricture of the small bowel with irregular mucosal thickening, which was confirmed as adenocarcinoma (arrow).
can also be a cause of small bowel obstruction due to the resulting intussusception. The lipoma and subsequent intussusception can be easily diagnosed on CT (20).
Submucosal tumors such as lymphoma or gastrointen- stinal stromal tumor rarely cause small bowel obstruc- tion.
Other Intrinsic Causes Bezoar
Bezoars are an unusual cause of an acute abdomen due to small bowel obstruction. The number of cases of bezoars has increased since the introduction of gastric surgery for treating gastroduodenal peptic ulcer or gas- tric cancer (21). Complete mechanical bowel obstruction is the most frequent clinical manifestation of bezoars.
The obstruction caused by small bowel phytobezoars frequently occurs in the jejunum or proximal ileum (22).
CT has become a useful method for diagnosing the pres- ence and cause of small bowel obstruction in this set- ting. The CT findings for obstruction due to bezoars in- clude a gas-containing intraluminal mass in the transi- tion zone that causes obstruction (Fig. 5A to 5D). In typi- cal cases, the luminal obstructing mass has a mottled ap- pearance that’s outlined by fluid attenuation and this is similar to the small bowel feces sign (Fig. 5A and 5B) (1, 23).
Foreign body
Incidentally ingested foreign material or an artificial device can be a cause of bowel obstruction (24). Foreign
A B
C D
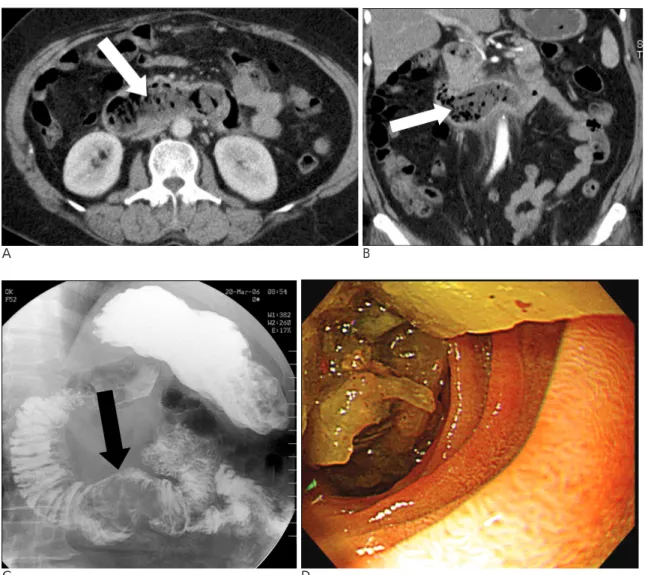
Fig. 5. A-D. Bezoar in the duodenum causing duodenal obstruction in a 66 year-old female patient.
A. The axial CT scan-coronal reformatted image shows material containing mottled gas in the dilated duodenal lumen (arrow).
B. The coronal reformatted image shows intraluminal food material that contains mottled gas, and this has a mass effect in the 3rd and 4th portions of the duodenum (arrow), suggesting possibility of a bezoar.
C. Barium study of the duodenum shows a large filling defect in the 4th portion of the duodenum (arrow).
D. Gastrofiberscopy demonstrates the bezoar.
bodies may pass smoothly through the bowel, but they can also directly obstruct a bowel segment (2).
Intraluminal devices such as a stent placed in malignant
gastrointestinal stricture can migrate to the distal part of the bowel and cause subsequent bowel obstruction. On MDCT, the curved MPR image can demonstrate the di-
A
B
Fig. 6. A-C. Migrated stent in the terminal ileum in a 59 year-old female patient.
A. The axial CT scan shows dilated ileal loops and an intralumi- nal metallic device, which is the distally migrated stent.
B. The oblique MPR image shows the full-length of the stent in the distal portion of the obstructed loop.
C. The curved MPR image shows thickening of the ileal wall at the distal end of the stent (arrow).
A B C
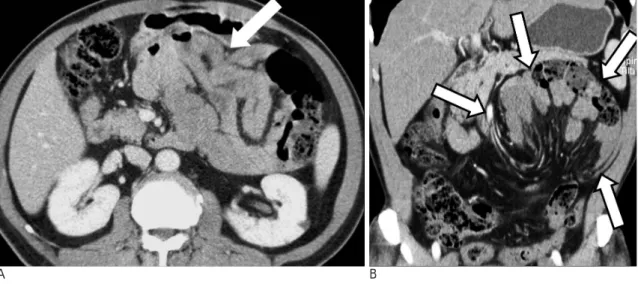
Fig. 7. A-C. Small bowel obstruction due to adhesion with closed loop obstruction and strangulation in a 56 year old female patient with a history of transabdominal hysterectomy.
A. Axial CT scan shows markedly dilated small bowel loops, which suggest small bowel obstruction. The degree of contrast en- hancement of the bowel wall is decreased.
B. The oblique axial image demonstrate an abrupt change of caliber and the beak appearance of two small bowel loops (arrow), which is the site of the adhesion. The narrow segments are pointing toward a single spot, suggesting closed loop obstruction.
C. The coronal image shows the markedly decreased contrast enhancement of the dilated small bowel loops and a large amount of ascites. These findings suggest strangulation of the loops. The narrow segments are pointing toward a single spot, suggesting closed loop obstruction (arrowhead).
C
rect relationship between the foreign body and the bow- el change with proximal obstruction (Fig. 6A to 6C).
Extrinsic Causes
Adhesions
There are adhesions in more than 90% of patients who have undergone laparotomy even one time. Adhesions may exist in either the area of surgical intervention or at the undersurface of the abdomen (25). Adhesive bands are formed by fibrin deposition and fibrinous adherence between the intraperitoneal surfaces that are stimulated by trauma or ischemia (26). However, symptoms are produced only in a few cases. Adhesions are responsible for at least 60% of the cases of small bowel obstruction;
more than 80% of these lesions occur after surgery, 15%
are due to inflammation and the remaining 5% are due
to congenital or unexplained causes. The CT findings are abrupt change of the luminal caliber at the distal portion of the dilated small bowel loops. A sharp, straight or slightly curved edge can be seen where the band crosses the bowel lumen (Fig. 7A to 7C) (2). All other possible causes of obstruction should be excluded on CT (1).
Hernia Internal Hernia
Internal hernia is a rare cause of small-bowel obstruc- tion, with a reported incidence of 0.2%-0.9% (27).
These hernias may be either congenital or acquired.
This condition involves herniation of a viscus, usually the small bowel, through a normal or abnormal aperture within the peritoneal cavity. This herniation may be persistent or intermittent. Because of the risk of strangu-
A B
C
Fig. 8. A-C. Left paraduodenal hernia presenting in a 54 year-old male patient with vomiting symptoms
A. The axial CT scan shows clustered small bowel loops between the stomach and pancreas. The inferior mesenteric vessel is displaced to the left and it is located at the anterior aspect of the hernial sac (arrowhead).
B. The coronal MPR image clearly demonstrates the hernial sac (arrows).
C. Barium study of the small bowel shows clustered proximal jejunal loops in the left upper abdomen (arrow).
lation of the hernia contents, even small internal hernias are dangerous and they can be lethal.
More than 50% of the internal hernias reported in the radiology and surgery literature have been paraduode- nal (28). The opening into the left paraduodenal hernial sac is known as the fossa of Landzert and it contains the inferior mesenteric vein and left colic artery in its anteri- or edge. The opening into the right paraduodenal her- nial sac is known as the fossa of Waldeyer and it con- tains the superior mesenteric vessels in its anterior edge.
On CT, the encapsulated bowel loops are seen either at the dudodenal junction between the stomach and pan- creas to the left of the ligament of Treitz, which is be- hind the pancreatic tail itself, and this displaces the infe- rior mesenteric vein to the anterior left or between the transverse colon and the left adrenal gland (Fig. 8A to 8C) (27).
The other types of internal hernia that have been de- scribed include transmesenteric hernia, supra- and/or perivesical hernia, intersigmoid hernia, foramen of Winslow hernia, and on rare occasions omental hernia.
External Hernia
Hernia through the walls of the abdominal cavity de- velops in approximately 1.5% of the population and this usually involves specific sites of congenital weakness or previous surgical incision (27, 29). CT is useful for de- picting the precise sites and the types of hernia and the contents. Among them, 75% of all abdominal hernias occur in the groin. These are inguinal, femoral, obtura-
tor and sciatic hernias. The inguinal hernias are usually an indirect type. Overall, the indirect inguinal hernias are the most common abdominal wall hernias. Indirect inguinal hernias account for 15% of all intestinal ob- struction (30). CT examination can provide useful diag- nostic information of the hernia’s contents and its differ- entiation from other masses involving the groin or scro- tum (Fig. 9A to 9B). In cases of strangulated hernia, a compromised blood supply is present that can cause thickening of the bowel loops. Adjacent inflammatory changes can be seen on CT in association with small bowel obstruction. The herniation occurs into the scro- tal sac along the long axis of the body, although to view this it is very helpful to reformat the images in the coro- nal or sagittal plane (Fig. 9B).
Obturator hernia is relatively rare. It occurs through the obturator canal, adjacent to the obturator vessels and nerve. The reported incidence of obturator hernia ranges from 0.05% to 1.5% of all hernias (31). Because of its anatomical position, this hernia more commonly presents as a bowel obstruction than as a protrusion of bowel contents. It can be easily diagnosed on MDCT with the MPR images, and the hernial sac is seen as a fluid filled mass or bowel loop extending between the pectineus and obturator muscles (Fig. 10A, B) (32).
Other extrinsic causes SMA Syndrome
SMA syndrome is an uncommon, but well recognized clinical entity that’s characterized by compression of the
A
B Fig. 9. A, B. Right inguinal hernia in a 63 year-old male patient.
A. The axial CT scan shows a small bowel loop and mesenteric fat in the right scrotal sac. The inferior mesenteric vein is displaced to the left and it is located at the anterior aspect of the hernial sac (arrowhead).
B. The oblique MPR image exclusively demonstrates a large peritoneal defect and herniation of the segmental ileal loop along the inguinal canal into the scrotal sac.
Fluid density is seen below the herniated loop.
third or transverse portion of the duodenum against the aorta by the SMA, resulting in chronic, intermittent or acute complete or partial duodenal obstruction (33, 34).
The MPR images can directly demonstrate the duodenal obstruction and distension and they can delineate the di- agnostic findings of a decreased aortomesenteric angle and distance (Fig. 11A and 11B). The aortomesenteric angle is 45 degrees with a range between 33 and 60 de- grees. In patients with SMA syndrome, the angle is sharply decreased, ranging from 6 to 25 degrees (Fig.
11B).
Complicated small bowel obstruction
Strangulation
The reported prevalence of strangulating small bowel obstruction ranges from 5% to 42% and its mortality rate ranges from 20% to 37% (35, 36). Strangulation is associated with adhesions and internal or external her- nias. The CT findings include evidence of small bowel obstruction, a circumferentially thickened loop with high attenuation within the wall, the “target sign,” and congestion or hemorrhage in the mesentery attached to the closed loop (Fig. 7A to 7C). Pneumatosis intestinalis
A B
Fig. 10. A, B. Intestinal obstruction due to obturator hernia in an 82 year-old female patient.
A. The axial image shows a fluid-filled round structure between the pectineus and obturator muscles (arrow).
B. The curved MPR image demonstrates a short segment of herniated bowel loop and dilatation of the proximal bowel, suggesting mechanical obstruction due to obturator hernia (arrow).
A
B Fig. 11. A, B. Proximal duodenal obstruction associated with superior mesenteric artery syndrome in a 34 year-old male patient.
A. The axial CT scan shows dilatation of the second portion of the duodenum with a compressed third portion between the aorta and superior mesenteric artery (ar- row).
B. The oblique MPR image shows a compressed duodenal loop (arrow) in the nar- rowed aortomesenteric angle (14 degrees).
may develop in advanced cases. Although ascites may be present in patients with closed loop obstruction with- out ischemia or with simple bowel obstruction, it is more commonly seen in patients with strangulation and this should be considered as a suspicious finding.
Closed Loop Obstruction
A closed or incarcerated small bowel loop is a form of mechanical obstruction in which a segment of bowel is occluded at two points along its course by a single con- strictive lesion occluding both the small bowel and mesentery. The closed loop is able to rotate along its ax- is, thereby producing a small bowel volvulus. The CT findings in closed-loop obstruction depend on its length and the degree of distention and the orientation of the closed loop in the abdomen (8). When a closed small bowel loop is horizontally oriented, it has a U- or C- shaped configuration on the cross-sectional imaging. A radial configuration with stretched mesenteric vessels converging toward the site of torsion may be detected depending on the orientation of the different small bow- el loops within the incarcerated bowel segment. At the
site of obstruction, the collapsed loops are round, oval or triangular (Fig. 7A to 7C). The “beak sign” seen at the site of torsion appears as a fusiform tapering on the lon- gitudinal bowel imaging (Fig. 7B and 7C) (37). A tightly twisted mesentery is occasionally seen in patients with volvulus and this has been described as the “whirl sign”
(38). Multiplanar reformation can provide easier visual- ization of these specific findings.
Afferent loop syndrome
Afferent loop obstruction is an uncommon complica- tion that occurs in 0.3% of the patients that have under- gone subtotal gastrectomy with Billroth II gastrojejunos- tomy (38). The causes include internal hernias, kinking of the anastomosis, adhesive bands, stomal stenosis, neoplasm and inflammatory disease. The abdominal ra- diographs are often normal because the afferent loop is fluid-filled as a result of distal obstruction. CT allows di- rect visualization of the obstructed afferent loop. The fluid-filled, dilated afferent portion of the jejunum can be easily identified (39) (Fig. 12A to 12C). With use of the curved MPR images, the cause of afferent loop syn-
A B
Fig. 12. A-C. Afferent loop syndrome after subtotal gastrectomy with gastro- jejunostomy in a 47 year-old male pa- tient.
A. The initial simple abdominal radi- ography demonstrates no specific ab- normality.
B. The coronal MPR image shows the fluid-filled, dilated duodenum in the upper abdomen.
C. The curved MPR image shows a to- tally fluid-filled duodenum and proxi- mal jejunum connected to the rem- nant stomach. There is focal wall thickening of the gastrojejunostomy site (arrow), which is the cause of the afferent loop obstruction.
C
drome can also be correctly predicted (Fig. 12C) (40).
Conclusion
Small bowel obstruction is frequently seen in daily CT practice. When bowel obstruction is diagnosed, it is es- sential to determine the site, level and cause of obstruc- tion for the appropriate management. In the new era of MDCT, it is possible to reconstruct the multiplanar im- ages and these images have proven validity for properly diagnosing patients suffering with small bowel obstruc- tion.
References
1. Boudiaf M, Soyer P, Terem C, Pelage JP, Maissiat E, Rymer R. CT evaluation of small bowel obstruction. Radiogrpahics 2001;21:613- 624
2. Herlinger H, Rubesin SE. Small bowel obstruction. In Gore RM, Levine MS, Laufer I. Textbook of gastrointestinal radiology 2nd ed.
Philadelphia: W. B. Saunders, 2000;815-837
3. Maglinte DD, Gage SN, Harmon BH, Kelvin FM, Hage JP, Chua GT, et al. Obstruction of the small intestine: accuracy and role of CT in diagnosis. Radiology 1993;188:61-64
4. Frager DH, Baer JW. Role of CT in evaluating patients with small- bowel obstruction. Semin Ultrasound CT MR 1995;16:127-140 5. Frager D, Medwid SW, Baer JW, Mollinelli B, Friedman M. CT of
small-bowel obstruction: value in establishing the diagnosis and determining the degree and cause. AJR Am J Roentgenol 1994;162:
37-41
6. Mucha P. Small intestinal obstruction. Surg Clin North Am 1987;
67:597-620
7. Marshall S, Nielsen A, Andruczak R. Bezoar following gastrectomy Digest Dis & Sc 2005;13:579-583
8. Megibow AJ. Bowel obstruction: evaluation with CT. Radiol Clin North Am 1994; 32:861-870
9. Choi D, Lee JS, Cho AY, Lim HK, Kim HS, Lee JW,et al. Bowel wall thickening in patients with Crohn’s disease: CT patterns and correlation with inflammatory activity. Clin Radiol 2003;58:68-74 10. Balthazar EJ, Gordon R, Hulnick D. Ileocecal tuberculosis: CT and
radiologic evaluation. AJR Am J Roentgenol 1990;154:499-503 11. Bargallo N, Nicolau C, Luburich P, Ayuso C, Cardenal C, Gimeno
F. Intestinal tuberculosis in AIDS. Gastrointest Radiol 1992;17:115- 118
12. Healy JC, Gorman S, Kumar PJ. Tuberculous colitis mimicking Crohn’s disease: case report. Clin Radiol 1992;46:131-132
13. Harisinghani MG, McLoud TC, Shepard JA, Ko JP, Shroff MM, Mueller PR. Tuberculosis from head to toe. Radiographics 2000;20:449-470
14. Pawlowski AS. Ascariasis. Clin Gastroenterol 1978;7:157-178 15. Sasaki T, Fukumori D, Matsumoto H, Ohmori H, Yamamoto F.
Small bowel obstruction caused by anisakiasis of the small intes- tine: report of a case. Surg Today 2003;33:123-125
16. Yoon SW, Yu JS, Park MS, Shim JY, Kim HJ, Kim KW. CT find- ings of surgically verified acute invasive small bowel anisakiasis resulting in small bowel obstruction. Yonsei Med J 2004;45:739-742 17. Mendelson RM, Nolan DJ. The radiological features of chronic ra-
diation enteritis. Clin Radiol 1985;36:141-148
18. DiSario JA, Burt RW, Vargas H, McWhorter WP. Small bowel can- cer: epidemiological and clinical characteristics from a populations based registry. Am J Gastroenterol 1994;89:699-701
19. Buckley JA, Fishman EK. CT evaluation of Small bowel neoplasm:
spectrum of disease. Radiographics 1998;18:379-392
20. Dudiak KM, Johnson CD, Stephens DH. Primary tumors of the small intestine: CT evaluation. AJR Am J Roentegenol 1989;152:
995-998
21. Verstandig AG, Klin B, Bloom RA, Hadas I, and Libson E. Small bowel phytobezoar: detection with radiography. Radiology 1989;
172:705-707
22. Hayes PG, Rotstein OD. Gastrointestinal phytobezoars: presenta- tion and management. Can J Surg 1986;29:419-420
23. Quiroga S, Alvarez-Castells A, Sebastia MC, Pallissa E, Barluenga E. Small bowel obstruction secondary to bezoar: CT diagnosis.
Abdom Imging 1997;22:315-317
24. Di Muria A, Formisano V, Di Carlo F, Aveta A, Giglio D. Small bowel obstruction by mesh migration after umbilical hernia re- pair. Ann Ital Chir 2007;78:59-60
25. Ellis H. The causes and prevention of intestinal adhesions. Br J Surg 1982;69:241-243
26. Myrhe-Jensen O, Larsen SB, Astrup T. Fibrinolytic activity in serosal and synovial membranes. Arch Pathol 1969;88:623-630 27. Ghagremani GG, Jimenez MA, Rosenfeld M, Rochester D. CT di-
agnosis of occult incisional hernias. AJR Am J Roentgenol 1987;148:
139-142
28. Martin LC, Merkle EM, Thompson WM. Review of internal her- nias: radiographic and clinical findings. AJR Am J Roentgenol 2006;
186:703-717
29. Rutkow IM. General surgical operations in the United States. Arch Surg 1979 to 1984;121:1145-1149
30. Sufian S, Matsumoto T. Intestinal obstruction. Am J Surg 1975;130:
9-14
31. Chang SS, Shan YS, Lin YJ, Tai YS, Lin PW. A review of obturator hernia and a proposed algorithm for its diagnosis and treatment.
World J Surg 2005;29:450-454
32. Megibow AJ, Wagner AG. Obturator hernia. J Comput Assist Tomogr 1983;7:350-352
33. Agrawal GA, Johnson PT, Fishman EK. Multidetector row CT of superior mesenteric artery syndrome. J Clin Gastroenterol 2007;41:62-65
34. Konen E, Amitai M, Apter S, Garniek A, Gayer G, Nass S, et al. CT angiography of superior mesenteric artery syndrome. AJR Am J Roentgenol 1998;171:1279-1281
35. Sarr MG, Bulkley GB, Zuidema GD. Preoperative recognition of intestinal strangulation obstruction: prospective evaluation of diag- nostic capability. Am J Surg 1983;145:176-182
36. Bizer LS, Liebling RW, Delany HM, Gliedman ML. Small bowel obstruction: the role of nonoperative treatment in simple intestinal obstruction and predictive criteria for strangulation obstruction.
Surgery 1981;89:407-413
37. Balthazar EJ, Birnbaum, BA, Megibow AJ, Gordon RB, Whelan CA, Hulnick DH. Closed-loop and strangulating intestinal obstruc- tion: CT signs. Radiology 1992;185:769-775
38. Fischer JK. Computed tomographic diagnosis of volvulus in intesti- nal malrotation. Radiology 1981;140:145-146
39. Gale ME, Gerzof SG, Kiser LC, Snider JM, Stavis DM, Larsen CR, et al. CT appearance of afferent loop obstruction. AJR Am J Roentgenol 1982;138:1085-1088
40. Kim HC, Han JK, Kim KW, Kim YH, Yang HK, Kim SH, et al.
Afferent loop obstruction after gastric cancer surgery: helical CT findings. Abdom Imaging 2003;28:624-630
대한영상의학회지 2008;58:283-295
다중검출기CT를 이용한 소장폐쇄평가1
1한양대학교 의과대학, 한양대학병원 영상의학과
2한양대학교 의과대학, 한양대학교 구리병원 영상의학과
이지혜・송순영・조온구・고병희・김용수2
소장폐쇄는 임상에서 흔히 접하며 그 진단은 임상증상과 환자의 과거력, 영상의학 소견을 종합하여 내리게 된다.
소장폐쇄가 의심되는 환자에서 폐쇄부위와 원인결정은 적절한 치료의 기본이다. 영상검사로 복부단순촬영을 흔히 시행하지만 그 정확도가 낮아 복부전산화단층촬영(CT)을 소장폐쇄의 진단에 필수검사로 시행하고 있다. 최근 다중 검출기전산화단층촬영기(MDCT)가 많이 보급되어 고해상도의 단면영상을 얻을 수 있고 삼차원영상프로그램을 통 한 영상의 다면재구성이 가능해졌다. 이 종설에서는 소장폐쇄의 원인, 부위, 및 이들과 동반된 합병증진단에 MDCT 검사와 다양한 삼차원재구성영상의 유용성을 기술하고자 한다.