84
Original Article
Korean Circulation J 2007;37:84-86
ISSN1738-5520
ⓒ 2007, The Korean Society of Circulation CASE REPORT
Cases of Right Ventricular Myocardial Infarction in Patients with an Absent or Hypoplastic Right Coronary Artery
Min-Seok Kim, MD, Jung-Kyu Han, MD, Sang-Eun Lee, MD, Song-Yi Kim, MD, Kyung-Woo Park, MD, Bon-Kwon Koo, MD and Hae-Young Lee, MD
Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Korea ABSTRACT
Two cases of myocardial infarction in the right ventricular (RV) wall, as well as the inferior wall, due to occlusion of the left circumflex coronary artery, with an absent or hypoplastic right coronary artery, are presented.(Korean Circulation J 2007;37:84-86)
KEY WORDS:Myocardial infarction;Right ventricle;Coronary vessel anomalies.
Introduction
A single or hypoplastic coronary artery is a rare cardiac anomaly. Because of the uncommon occurrence, it is difficult to make rapid management plan when myo- cardial infarction is developed. Coronary anomalies cause different collateral blood supply and it is important to know which of collateral vessels contributes the missing portion of the artery. We report our experiences in two patients with coronary anomalies and associated RV infacrtion which resulted in the disastrous clinical course and the difficulty making treatment plan.
Case
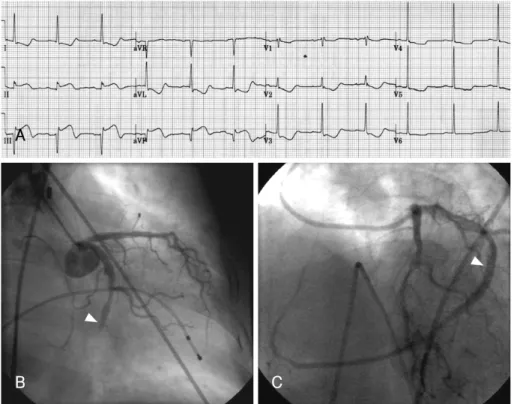
Case 1A 71-year-old female patient presented with acute onset of epigastric pain that had occurred 4 hours pre- viously. She had been managed for hypertension. On physical examination, her blood pressure was 142/96 mmHg and pulse rate 71 beats per minute. The electro- cardiogram(ECG) on admission showed ST segment ele- vation in leads II, III and aVF, with reciprocal change, consistent with acute myocardial infarction in the infe- rior wall(Fig. 1A). The ECG also showed sinus rhythm, but without any other arrhythmia, such as atrioventri-
cular block. A reverse electrocardiogram was not obtai- ned. Her plasma CK, LDH and CK-MB levels were 172, 193 and 12 IU/L, respectively. Percutaneous coronary intervention(PCI) was not immediately available, so thrombolytic therapy with urokinase was initiated. Howe- ver, no sign of reperfusion was observed until 1 hour after thrombolysis and the systolic blood pressure fell to 60 mmHg. On echocardiographic evaluation, despite in- ferior wall akinesia, the left ventricle showed a preserved systolic function, with an ejection fraction of about 50%, but the right ventricle showed the dilatation and akinesia, compatible with right ventricular myocardial infarction. Despite vigorous hydration, the hypotension persisted, and bradycardia developed, of about 40 beats per minute.
Thus, cardiac angiography was performed for rescue PCI. Coronary angiography revealed the culprit lesion of the totally occluded distal portion of the left circum- flex coronary artery(Fig. 1B); however, the ostium for the right coronary artery could not be found. PCI, with sten- ting on the left circumflex artery, revealed a markedly dominant left circumflex artery supplying the inferior wall, as well as the RV(Fig. 1C). However, soon after in- tervention, a rupture of the right ventricular myocardium occurred, and despite the operation, the patient regret- tably died.
Case 2
A 61-year-old male patient presented with chest dis- comfort that had occurred 3 hours previously. He had been managed for hypertension and had a previous hi- story of ischemic stroke. His initial blood pressure was 119/66 mmHg and pulse rate 69 beats per minute. The
Received:September 28, 2006 Accepted:October 31, 2006
Correspondence:Hae-Young Lee, MD,Department of Internal Medicine, Seoul National University College of Medicine, 28 Yeongeon-dong, Jong- no-gu, Seoul 110-744, Korea
Tel: 82-2-2072-0696, Fax: 82-2-3676-4103 E-mail: [email protected]
Min-Seok Kim, et al:Cases of RV Infarction in Patients with Coronary Anomalies·85
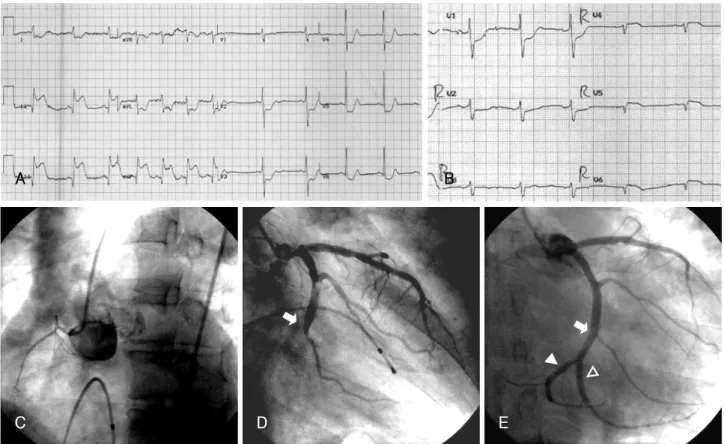
electrocardiogram on admission showed ST elevation in the inferior(Fig. 2A) as well as reverse precordial leads (Fig. 2B), consistent with acute myocardial infarction in the inferior wall as well as the RV wall. His plasma CK, LDH and CK-MB levels were 3890, 582 and 319 IU/L, respectively. Coronary angiography for primary PCI was performed, which showed a remarkable hypoplastic right coronary artery, with scant marginal branches(Fig. 2C) and a totally occluded left circumflex artery in the distal portion(Fig. 2D, arrow). A guidewire was successfully pas- sed to the distal part of the total occlusion, and a stent implanted(Fig. 2E, hollow arrowhead).
However, despite the restoration of antegrade flow, no improvement of his vital sign was observed, and hypo- tension with bradycardia was aggravated. Therefore, inotropic support with intravenous dobutamine was ini- tiated, at which time, junctional tachycardia occurred, consistent with reperfusion arrhythmia, and a small side branch of the circumflex artery to the inferior aspect of the interventricular septum was visualized. Another guide- wire was advanced and predilatation performed, which showed the proper distal part of the left circumflex artery supplying the AV node and RV wall(Fig. 2E, filled arrowhead). The branch artery, in which the former stent had been inserted, was revealed as the prominent 3rd obtuse marginal branch. An additional stent was im- planted into the true distal left circumflex coronary artery.
The final left coronary angiogram showed the successful
revascularization of the arteries supplying the inferior wall as well as the RV wall.
Discussion
A single or hypoplastic coronary artery is a rare cardiac anomaly,1-3) associated with the under-development of one entire coronary artery or its major branches. In both anomalies, two compensations for the missing portion of the artery occur. The single or dominant coronary artery may connect with the vascular coronary bed, where the orifice from the aorta is not developed sufficiently by the collateral vessels or may quickly divide into right or left branches, with the distribution; thereafter, being relatively normal.4)
It has been reported that these anomalies are often diagnosed at autopsy following sudden death due to stressful exercise. The cause of sudden death during exer- cise is known to be the result of an insufficient collateral supply to the area normally supplied when these ano- malies are not present. 5 However, when myocardial infarction in a single or dominant artery develops, the clinical course will be disastrous. The present cases show a RV infarction caused by an occlusion of the left circumflex coronary artery. The right coronary artery was absent or very hypoplastic; therefore, the branches from the left coronary artery supplied the right ventri- cle. Of course, although the results were that the patient A
B C
Fig. 1. Acute right ventricular myocardial infarction due to occlusion of a single coronary artery. A: the ECG on admission shows ST elevation in the inferior leads. B: initial coronary angiography of the left coronary artery shows occlusion of the distal portion of the left circumflex artery. C: final coronary angiography, following percutaneous coronary intervention, shows a markedly dominant left coronary circumflex artery extending to the right myocardium. Arrowhead indicates the previously occluded site. ECG: electrocardiogram, ST: the ST segment.
86·Korean Circulation J 2007;37:84-86
with a single coronary artery could not be saved, but the patient with a hypoplastic RCA could, cannot be generalized as the clinical outcome of each anomaly, as those rare anomalies delayed the clinical judgment as well as the adequate revascularization to the infarcted myocardium. 6 Moreover; in the latter case, the obtuse marginal(OM) branch was so prominent it was mis- judged as being the main circumflex artery.
In conclusion, when myocardial infarction in the inferior wall occurs, and no RCA orifice or only a hy- poplastic RCA is observed by coronary angiography, the possibility of an occlusion of the prominent left circum- flex artery, compensating for the right coronary artery, as well as the possibility of an accompanying infarction in the RV wall, should be considered.
REFERENCES
1) Lipton MJ, Barry WH, Obrez I, Silverman JF, Wexler L. Isolated single coronary artery: diagnosis, angiographic classification, and clinical significance. Radiology 1979;130:39-47.
2) Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn 1990;21:28-40.
3) Desmet W, Vanhaecke J, Vrolix M, et al. Isolated single coronary artery: a review of 50,000 consecutive coronary angiographies.
Eur Heart J 1992;13:1637-40.
4) Blake HA, Manion WC, Mattingly TW, Baroldi G . Coronary artery anomalies. Circulation 1964;30:927-40.
5) Fraisse A, Quilici J, Canavy I, Savin B, Aubert F, Bory M. Myo- cardial infarction in children with hypoplastic coronary arteries.
Circulation 2000;101:1219-22.
6) Choi KL, Kwon JI, Jung WH, et al. Stenting of an anomalous coronary artery in acute myocardial infarction. Korean Circ J 1998;28:1378-81.
Fig. 2. Acute right ventricular myocardial infarction due to occlusion of the left circumflex coronary artery, with a hypoplastic right coronary artery.
A: the ECG on admission shows ST elevation in the inferior leads. B: the ECG of the reverse precordial leads shows ST elevation in the reverse precordial leads (from V4R to V6R). C: initial coronary angiography of the right coronary artery showed a very hypoplastic right coronary artery, with scant acute marginal branches supplying the right ventricle. D: initial coronary angiography of the left coronary artery showed the totally occluded distal portion of the left circumflex artery (arrow). E: final coronary angiography, following percutaneous coronary intervention, shows a markedly dominant left circumflex artery extending to the right myocardium. The arrow indicates the previously occluded site, the filled arrowhead the proper distal part of the left circumflex artery supplying the AV node and RV wall and the hollow arrowhead the prominent 3rd obtuse marginal branch, misjudged as the main distal circumflex artery. ECG: electrocardiogram, ST: the ST segment, AV: atrioventricular, RV: right ventricular.
A B
C D E