대 한 방 사 선 의 학 회 지 1992; 28(6) : 881~887
Journal of Korean Radiological Society, November, 1992
퍼1 암 환자에서 폐절제술후 흉부 CT 소견
원자력병원 진단방사선과
이아라 • 도영수 • 이병흐I
•
번홍식 • 김기환 • 진수일 • 조재일* • 심영목*- Abstract-
Chest CT Findings after Pneumonectomy for Lung Cancer
Ah Ra Lee, M.D., Young 800 Do, M.D., Byung Hee Lee, M.D., Hong 8ik Byun, M.D., Kie Hwan Kim, M.D., 800 Yil Chin, M.D., Jae Il Zo, M.D*., Young Mok 8im, M.D*.
Department of Diagnostic Radiology, Korea Caηcer Ceη ter Hospital
Evaluation of postpneumonectomy space (PPS) by CT in patients with lung cancer for operation-related complication or tumor recurrence is critical, but often difficult. We retrospectively analysed CT scans of 38 patients who underwent pneumonectomy for lung cancer. CT scans were obtained on 7-1 Oth post-operative day for baseline image and at varying intervals of 2 to 24 months thereafter. U sual postoperative findings in patients without complication included mediastinal shifting, changes in subpleural space, changes in parietal pleura, and herniation of contralateral lung.
Four patients had postoperative complications including empyema (n = 3) and bronchopleural fistula (n = 2).
Twelve patients showed findings of tumor recurrence such as lymph node metastasis, local recurrence, and pericardial and contralateral pleural effusion.
By comparing follow-up CT with baseline CT
,
we were able to detect carly cancer recurrence and postoperative complications. Our results indicate that serial chest CT play an important role in the evalua tion of the patients who underwent pneumonectomy for lung cancerIndex Words: Lung, neoplasm 60.3216
Lung, postoperative change 60.45 Lung, CT 60.1211
서 론 을 시 행 한 후 post-pneumonectomy space(이 하 PPS)
가 전체적으로 균질한 음영 증가를 보이며, 수술후 종격 동의 전이로 PPS 또는 종격동에 발생하는 합병증이나 재 폐암 환자에 있어서 전산화 단충 촬영(CT)은 수술전 발의 발견에 어려움이 많다. 이에 저자들은 폐절제술후 병기 결정과 수술후 추적 검사 등에 널리 이용되어왔다 추적검사 중 정상적으로 보일 수 있는 CT소견을 분석하 (1-9) . 수술후 재발 또는 합병증의 조기 진단은 향후 환 였고 이를 기초로 수술후 합병증이나 재발의 CT 소견을 자 치료에 중요한 역할을 하여 추적 검사로 단순 흉부 촬 분석하기 위하여 본 연구를 시행하였다.
영등의 고식적 요법을 이용하기도 하였으나, 전폐절제술
*원자력병원 흉부외과
*Dφartment 01 Thoracic Surgery, Korea Caηcer Center Hospital
이 논문은 1992 년 7 월 31일 접수하여 1992 년 10월 5 일에 채택되었음.
- 881-
수술후 재발이나 합병증 등의 비정상 추적 CT소견을 보 인 환자가 16명이다. 수술후 재발로 판명된 12명중 조직 검사로 3명이 확진되었고 나머지 9명은 방사선학적, 임상 적 추적 검사로 확진하였으며, 합병증이 있었던 4명은 모 두 임상적으로 확진하였다.
CT 는 9800 scanner(GE Medical System, Milwau- kee) 로、 Rayvist 300@(68. 3% of meglumine iog licate, Schering Korea) 150ml로 조영 증강후 흉곽 입 구에서 상복부까지 10mm 간격, 10mm 두께로 스캔하 였다. CT의 분석은 수술후 7-10일째에 CT를 시행하여 이를 기준으로 하고(기초 CT) 그후 2-24개월간 약 6개 월 간격으로 CT를 시행하여(추적 CT), 수술후 재발 또 는 합병증이 있었던 경우의 CT를 비정상 추적 CT, 없었 던 경우를 정상 추적 CT라 정의하고 이들을 각각 후향적 으로 분석하였다.
정상추적 CT 소견은 1) 종격동의 이동(shifting), 2)
결 과
정상 추적 CT 소견
38명의 환자중 추적 CT에서 정상적 술후 소견을 보인 환자는 22예로 Table 1 과 같은 해부학적 변화가 관찰되 었다. 모든 예에서, 추적 CT에서 PPS에 균질의 삼출액 이 관찰되 었고 PPS의 용적은 수술후 추적 기간과 무관하 게 감소하였다. 좌, 우 폐절제술에 따른 종격동의 변화를 보면, 좌폐절제술을 시행한 13명의 환자는 모두 좌측으로 의 종격동 구조물의 단순 이동(transfer)을 보인 반면 우 폐절제술을 받은 9명중 5명은 우측으로 종격동 구조물의 회전을 동반한 회전 이동(rotation)이 (Fig. 1), 3 명은 단순 이동이 관찰되었고 나머지 한명에서는 종격동의 이 동이 관찰되지 않았다. PPS에는 용적이 점차 줄어들면서
a b
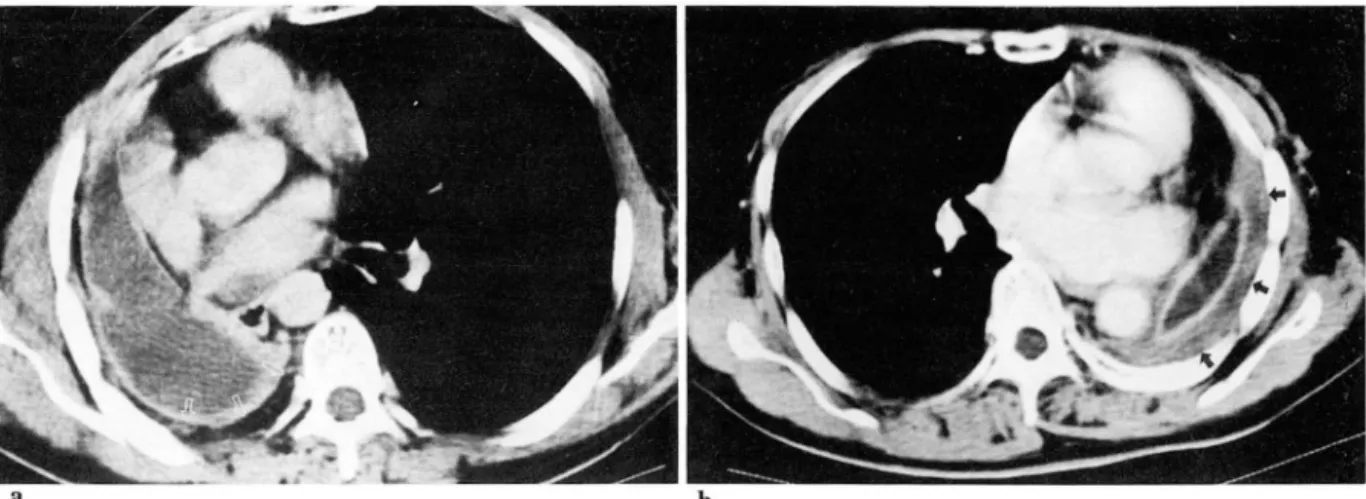
Fig.1. a. 59-year-old man with left pneumonectomy showing mediastinal shift. CT scan obtained 10 months after pneumonectomy shows mediastinal transfer to left side. Note clockwise rotation ofthe aortic arch showing anteroposterior direction of its long axis.
b. 55-year-old man with right pneumonectomy shows mediastinal shift. CT scan obtained 12 months after pneumonectomy shows mediastinal rotation to right side. N ote counter-clockwise rotation of the aortic arch showing transverse direction of its long axis
이아라 외 : 폐암 환자에서 폐절제술후 흉부 CT
a b
Fig.2. a. 55-year-old man with right pneumonectomy showing irregular parietal pleural enhancement and f1uid collection in PPS. CT scan obtained after 12 months after pneumonectomy shows fat accumulation in subpleural space (arrows)
b. 60-year-old woman with left pneumonectomy showing soft tissue accumulation in subpleural space (ar- rows) on CT scan obtained 16 months after pneumonectomy
Fig. 3. 47-year-old man with left pneumonectomy showing [at accumulation in retrosternal space (ar- rows). CT scan obtained 14 months after pneumonectom y shows no evidence of herniation of contralateral lung.
늑막하강에 2-5mm 두께의 지방과 연조직이 각각 또는 함께 축적되는 변화가 관찰되었다(Fig.2). 벽측 늑막의 변화는 1예를 제외하고 3-10mm의 불규칙한 늑막(벽측 늑막) 비후와 균질한 조영증강이 벽측늑막에서 관찰되었 다(Fig. 2). 22예중 21예에서 반대쪽 폐의 과다팽창을 통 반한 후흉골강(retrosternal space)을 통한 폐 전이가 있었는데 한 예에서는 후흉골강에 과다한 지방이 축적되 어 반대편 폐의 전이가 관찰되지 않았다(Fig.3).
Table 1. Normal Post-pneumonectomy Findings (N = 22)
1. Parietal Pleural Thickening
<5mm 11
5-10mm 10
Negative 2. Mediastinal Shift
Rotation Transfer
4 13 Rt
Lt 5 0 3. Subpleural Space
Fat Soft tissue Both Negative
?J n。Qι 。4
4. Lung Herniation Anterior Negative
21
비정상 추적 CT 소견
수술후 비정상 추적 CT 소견으로 재발이 12예, 수술후 합병증이 4예에서 관찰되었다(Table 2)
수술후 폐암의 재발은 12예에서 있었다. 임파절 전이는
단경 1. 5C111 이상의 입파절 종대가 종격동 임파절 3예,
쇄 골 상 부 임 파 절 (supracJavicular node) 1예, 후 횡 격 막 임 파 절 (retrocrural node) 1예 가 관 찰 되 었 다 (Fig.
4). 국소 재발은 4예에서 관찰되었다. 이들은 폐절제술을
- 883 -
a b
Fig. 4. CT scan obtained 10 months after pneumonectomy showing lymph node metastasis as evidence of recurrence.
a. 57-year-old woman with left pneumonectomy shows newly developed lymph node enlargement in mediastinum (arrows).
b. 55-year-old man with left pneumonectomy shows enlarged lymph node in right retrocrural space.
a
Fig 5. 55-year-old man with left pneumonectomy showing local recurrence of malignancy.
a. Baseline CT scan obtained one month after pneumonectomy.
b. CT scan obtained 6 months after pneumonectomy shwos irregularly enhancing soft tissue density (ar rows) adjacent to surgical stur매, d빽lacing PPS laterally.
Table 2. Abnormal Post-pneumonectomy Findings 시행한 절단부 주위에서 심장과 PPS사이에 5cm 이상의 (N = 16)
불균질의 연조직으로 관찰되었으며 연조직에 의한 주위 구조물의 이동이 3예에서 관찰되었다(Fig. 5) 심막 삼출 액과 반대펀 늑막 삼출액이 각각 5예, 2예씩 있었고(Fig.
6) 이들 재발 소견들이 둘 이상 함께 관찰되었던 예가 6 예였다.
수술후 합병증이 관찰되었던 4예 중 1예는 기관지늑막 루와 농흉이 함께 있었고 2예는 농흉을, 1명은 기관지늑 막루를 보였다. 농흉은 수술후 감소되었던 PPS의 용적이 증가하여 종격동 구조물을 중앙으로 전이시키고 늑막의
1. Recurrence
Local Recurrence LN Enlargement
Mediastinal Node Supraclavicular Node Retrocrural Node Pericardial EfI‘uSlOn
Contralateral Pleural Effusion 2. Complication
Empyema
Bronchopleural Fistula
4
(3) (1) (1)
4 3
이아라 외 : 폐암 환자에서 폐절제술후 흉부 CT
a b
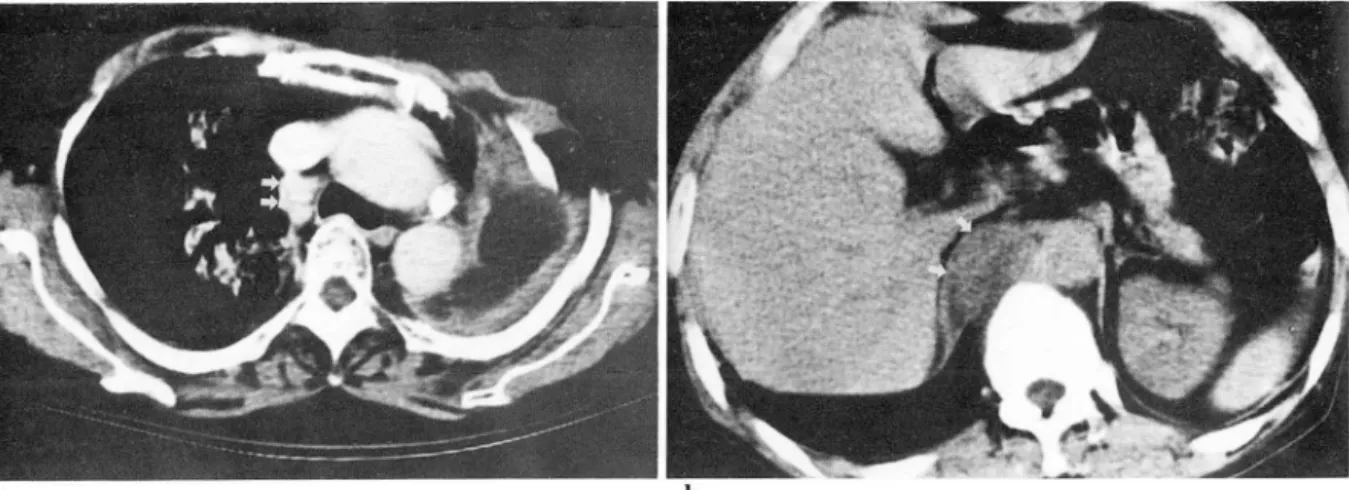
Fig. 6. 44-year-old man with right pneumonectomy showing evidence of recurred malignancy a. Baseline CT scan obtained 10 days after pneumonectomy.
b. CT scan obtained 6 months after pneumonectomy shows pericardial and contralateral (left) pleural effusion
a b
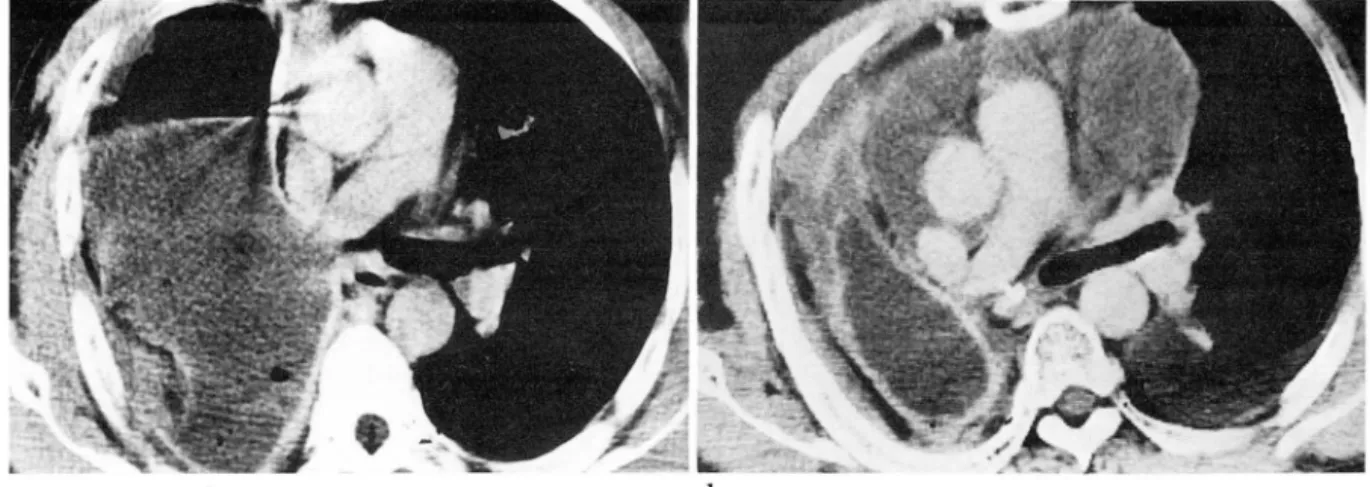
Fig. 7. 66-year-old man with right pneumonectomy showing empyema as postoperative complication a. Baseline CT scan obtained 1 month after pneumonectomy shows concave mediastinal border of parietal pleura
b. CT scan obtained 9 months after pneumonectomy shows rather increased volume of PPS and conveX mediastinal border of parietal pleura with regular enhancement
균질한 비후와 조영제 증강이 관찰되었다(Fig.7). 기관 지늑막루는 PPS에 균질의 삼출액외에 다양한 크기의 다 수의 공기수면상(air-fluid leve J)으로 관찰되었다(Fig
8 ) .
고 "'E르 ~
을 빨리 발견하여 적절한 치료를 하는 것이 매우 중요하 며 단순 촬영만으로는 불충분하다.
폐절제술후 동측 흉강 내에는 공기와 삼출액이 차고 공 기는 점차 흡수되며 삼출액만이 남게된다. 이 삼출액의 양도 점차 감소하여 수술후 대개 8-24개월이 지니면 종 격동 이동, 횡격막 상승, 늑골간의 협소로 인해 PPS의 용 적 감소와 함께 반대쪽 폐의 과다 팽창과 이동이 나타난 다. Biondetti등은 수술한 쪽과 수술하지 않은 쪽 폐 의 폐암 환자의 수술적 요법은 가장 널리 사용되고 있으며 전후 직경을 비교하여 퇴축 비율(retraction index)을 부가적인 방사선 요법이나 화학 요법으로 생존율을 높일 계산하였고 이것과 반대쪽 폐의 이동과의 유의한 연관성 수 있다(3, 5, 8). 이를 위하여는 수술후 합병증이나 재발 을 보여주었다(3).
a b
Fig. 8. 55-year-old man with left pneumonectomy showing bronchopleural fistula as postoperative com- plication.
a. Plain chest PA obtained 10 months after pneumonectomy shows newly developed multiple air-f1uid levels in PPS.
b. CT scan obtained at the same time shows air-f1uid Ievels in PPS.
수술후 정상 종격동의 이동을 분석하여 보면 우폐절제 술을 시행하였을때 종격동이 우측으로 회전하여 대통맥궁 이 전두면(frotal plane)과 일치하며, 좌폐절제술을 시행 하였을 때 종격동의 화측으로의 이동을 보여 대동맥궁이 시상변 (sagittal plane)과 일치한다고 Biondetti등이 보 고하였다(3). 저자들의 경우 우폐절제술후 9례 중 5례에 서 종격동의 우측 회전이 관찰되었고 좌폐절제술을 시행
한 13예 모두에서 종격동의 좌측 이동이 관찰되었다(Fig.
1, Table 1).
Biondetti 등은 반대편 폐의 이통이 좌폐절제술후에는 전방 또는 후방으로의 전이가 유사한 빈도를 보인 반면, 우폐절제술후에는 모두 전방으로의 전이를 보였다고 하였 으며, 이를 대동맥의 위치와 연관된 것으로 설명하였다 (3, 9), 그러나 저자들의 경우는 좌, 우폐에 상관없이 거 의 전 예에서 전측폐 전이를 보였고 좌폐절제술을 시행한 한 예에서만 이동이 없었는데 이는 후흉벽강내의 지방 침 착에 의한 것이었다.
폐절제술후 정상적으로 벽측 늑막이 불균질하게 두꺼워 지며 조영제 증강후 비교적 균질한 조영 증강이 관찰되었 는데, 이는 벽측 늑막의 표면적 감소와 섬유아세포 증식 에 의한 섬유화가 그 원인으로 생각된다. 또한 폐절제술 후 정상적으로 늑막하강에 2-5mm의 지방 축적이 관찰 되었는데 이는 입등, Waite 등이 만성 늑막염증에서 관 찰된다고 보고하였으며 그 정확한 기전은 알려져있지 않 다(10 ← 12).
폐절제술후 정상적인 PPS의 종격동측면(mediastinal border)은 좌, 우에 관계없이 또 수술 후 경과된 시간에
관계없이 오목한 면(c oncave margin)을 보이나 PPS내 에 이차적 감염으로 인한 농흉이 생겼을 경우 PPS의 확 장과 종격동쪽 늑막(mediastinal pleura)의 융기(bulg
ing) , 그리고 종격동 구조물의 중앙 또는 수술하지 않은
쪽으로의 재이동을 초래한다(1,6, 7). 저자들의 경우 농흉 이 있었던 3예에서 모두 이러한 소견을 보였고 이와 함께 벽측 늑막의 균일한 조영증강이 보였다. 이는 정상적인 PPS에서 벽측 늑막이 불규칙한 비균형질의 조영 증강을 보인것과 대조적인 소견이다(Fig.4) 또다른 수술후 합 병증으로 기관지늑막루가 있었는데 이때는 PPS에 새로 이 공기의 음영이 나타나므로 단순 흉부 촬영등의 고식적 인 방사선학적 방법에 의해서도 비교적 쉽게 발견할 수 있었다(Fig.5).
폐암 수술후 재발은 국소 재발과 임파절 전이로 가장 많이 나타나는 것으로 알려져 있다(2, 4, 5, 9). Abadir 등 은 재발 환자의 부검에서 국소 재발(50-88%), 종격동 임 파절 전이(77-86%), 그외 반대편 폐, 원격성 임파절, 뇌 등으로의 전이가 있었음을 발표하였다(9). 국소 재발의 경우 불균질의 연조직이 PPS의 문합 부위 근처에 나타나 는데, 저자틀의 경우 수술 직후 시행한 CT 를 기준으로 하고 일정기간의 추적 검사를 통해 수술 직후 관찰되지 않던 5cm 이상의 연조직이 추적 CT 검사에서 관찰되어 수술후 섬유화와 감별할 수 있었다(Fig. 6). Glazer등에 의하면 재발 환자 12명중 국소 재발이 2예 임파절 전이가
11예이었고 침범된 임파절은 우폐절제술의 경우 전기관
임 파 절 (pretracheaJ) 과 기 관 분 기 하 부 임 파 절 (subcar-
inaJ)이 많았고, 좌폐절제술의 경우 기관분기하부, 대동
맥 외측(J ateral aortic). 대동맥폐동맥개창(aorticopul
monary window), 전기관(pretracheail 임파절의 순으 로 나타났다(4), 저자들의 경우는 대부분 종격동내 임파 선을 가장 많이 침범하였으며 그 외에 후횡격막 임파절과 쇄골 상부 임파절로의 전이가 각각 한예씩 있었다(Fig.
7).
폐암으로 폐절제술을 시행한 환자의 경우 재발이 대부 분 종격동 내에서 관찰되기 때문에 확진을 위한 외과적 수술 또는 조직검사가 거의 시행되고 있지 않아 대부분 방사선학적 추적검사로 진단되고 있다. 따라서 수술후 추 적 정상 CT의 소견에 친숙하는 것이 재발의 조기 발견에 중요하다.
결론적으로 CT는 폐절제술후 재발 및 합병증의 평가 에 중요한 검사로 지속적인 추적 CT검사가 필요하며 정 확한 평가를 위해 수술후 7-10일째에 기초 CT를 시행 하여 추적 CT와 비교하는 것이 필요할 것으로 생각된다.
참고문헌
1. Heater K
,
Revzani L,
Rubin JM. CT evalua- tion of empyema in the postpneumonectomy space. AJR 1985;145:39-402. Peters JC, Desai KK. CT demonstration of postpneumonectomy tumor recurrence. AJR 1983; 141:259-262
3. Biondetti PR, Fiore D, Sartori F, Colognato A, Ravasini R
,
Romani S. Evaluation of the post-이아라 외 : 폐암 환자에서 폐절제술후 흉부 CT pneumonectomy space by computed tomogta- phy. JCAT 1982;6:238-242
4. Glazer HS, Aronberg DJ, Sagel SS, Emami B U tility of CT in detecting postpneumonectomy carcmoma recurrence‘ AJR 1984;142:487-494 5. Spjut
HJ
, Mateo LE. Recurrent and metastatic carcinoma in surgically treated carcinoma of lung: An autopsy survey. Cancer 1965;18 1462-14666. Kerr WF. Late-onset post-pneumonectomy em- pyema. Thorax 1977 ;32: 149-154
7. Zumbro JI J r., Treasure R, Geiger JP, Green DC. Empyema after pneumonectomy. Ann Thor Surg 1973;15:615-620
8. Heitzman ER. Computed tomography of the chest: current perspectives. AJR 1981;136:2-12 9. Abadir R, Muggia FM. Irradiated lung cancer.
An autopsy snalysis of spread pattern. Radiology 1975;114:427-430
10. ImJG, Webb WR, Rosen A, Gamsu G. Costal pleura: Appearances at high-resolution CT Radiology 1989; 171:125-131
11. ImJG, Webb WR, Han MC, ParkJH. Apical opacity associated with pulmonary tuberculosis:
High-resolution CT findings. Radiology 1991; 178:727-731
12. Waite RJ, Carbonneau RJ, Balikian JP, U mali CB, Pezzella AT, Nash G. Parietal pleural changes in empyema:Appearance at CT.
Radiology 1990; 175’145-150