서론
가슴 속 구조물들을 보호하는 역할을 하는 흉벽은 폐가 생리 학적 운동을 하는 데 기본이 되는 구조적인 골격의 역할을 하기 도 한다. 그래서 흉벽의 변형은 호흡기계에 제한적, 폐쇄적 폐 병변을 초래할 수 있다(1). 흉벽에 병변이 있을 때 증상은 촉지 되는 흉벽종괴, 발열, 흉통 등인데, 소아는 증상을 잘 표현하지 못하기 때문에 촉지되는 흉벽종괴를 주소로 하는 경우가 많다.
흉벽에 생기는 종양이나 소아 흉벽의 변이, 감염과 종양에 대 한 보고들이 있으나 소아에서 촉지되는 병변에 대한 보고들은 적다. 소아에서 촉지되는 흉벽질환은 선천성 병변, 외상, 감염, 액와부 림프절 종대, 연부조직 종양과 골종양 등이 있다(1-4).
병변들에 따라 성인과 유사하지만 소아에서 더 많이 호발하는 질환들이 있고, 흉골의 부분 전위(segmental dislocation)나 Bacillus Calmette-Guerin (BCG) 림프절염과 같이 소아에서만 볼 수 있는 질환들도 있다(5, 6).
다양한 질환들이 촉지되는 병변으로 나타날 수 있기 때문에 이학적 검사만으로는 이런 병변들을 진단하는 데 어려움이 있다
(2, 7). 종괴가 작을 경우는 일차적으로 초음파를 시행하나(6) 종괴가 크거나 동반된 뼈의 이상이나 흉곽의 구조적인 이상 여 부를 보기에는 제한점이 있다. Magnetic resonance (MR)는 해 상도가 뛰어나서 종양의 침범범위와 조직의 특성을 아는 데 유 용하나(2, 7) 촬영시간이 길어 소아에서는 진정을 요하는 경우 가 많고 CT보다 촬영이 용이하지 않다. 이에 비해 CT는 방사 선 노출의 부담이 있으나 MR보다 뼈 등 부가적으로 구조물을 이해하는 데 도움을 준다. 소아에서 촉지되는 흉벽병변들이 뼈 와 관련되는 변이와 질환이 많기 때문에 CT가 유용할 수 있다.
또한 종양 내부에 석회화가 있거나 지방성분이 있을 때 연부조 직 종양의 골침범을 보는 데 유용하다(3, 7).
이에 소아에서 촉지되는 흉벽병변으로 나타날 수 있는 질환 들을 분류하고 CT 영상소견을 기술하고자 한다.
정상변이
소아에서 전방 흉벽에는 여러 가지 변이들이 보일 수 있는데, Donnelly와 Frush (1)에 의하면 소아의 1/3에서 전방 흉벽에
J Korean Soc Radiol 2013;68(3):261-269
Received May 1, 2012; Accepted October 15, 2012 Corresponding author: Young Tong Kim, MD Department of Radiology, Soonchunhyang University College of Medicine, Cheonan Hospital,
31 Suncheonhyang 6-gil, Dongnam-gu, Cheonan 330-721, Korea.
Tel. 82-41-570-3515 Fax. 82-41-579-9026 E-mail: [email protected]
Copyrights © 2013 The Korean Society of Radiology
A wide variety of diseases manifest as palpable chest wall masses in children. These include normal variation, congenital anomalies, trauma, infection, axillary lymphade- nopathies, soft tissue tumors and bone tumors. Given that most of these diseases are associated with chest wall deformity, diagnosis is difficult by physical examination or ultrasonography alone. However, multi-detector CT with three dimensional recon- struction is useful in the characterization and differential diagnosis of palpable chest wall lesions. In this article, we review the spectrum of palpable chest wall diseases and illustrate their multi-detector CT presentation.
Index terms
Palpable Chest Wall Child CTMulti-Detector CT Findings of Palpable Chest Wall Masses in Children: A Pictorial Essay
1소아에서 촉진되는 흉벽종괴의 Multi-Detector CT 소견: 임상화보
1Chan Ho Park, MD
1, Young Tong Kim, MD
1, Hyun Sook Hong, MD
21Department of Radiology, Soonchunhyang University College of Medicine, Cheonan Hospital, Cheonan, Korea
2Department of Radiology, Soonchunhyang University College of Medicine, Bucheon Hospital, Bucheon, Korea
한다. 누두흉 또는 오목가슴은 흉골에 생기는 가장 흔한 선천 성 기형이지만 진단하는 데 어려움이 없다. 하지만 치우친 흉골, 전방 늑골과 늑연골의 현저한 돌출, 늑연골의 현저한 비대칭, 연골 주위 결절 등은 환자나 환자 보호자에 의해 촉지되어 병 원을 찾기도 한다(1-4). 또한 지방종증과 같이 비만과 관련하 여 피하지방에 지방이 축적되어 촉지되는 병변을 주소로 내원 하는 환자들이 드물지 않게 있다(8)(Fig. 5).
변이를 보인다고 하였다. 또한 소아에서 촉지되는 흉벽병변의 대부분이 정상적인 변이이다. 또한 정상변이 환자의 대부분은 통증이나 이학적 검사상 압통과 같은 증상이 없었다(1). 이러한 변이들은 치우친 흉골(tilted sternum), 전방 늑골과 늑연골의 현저한 돌출(prominent convexity of anterior rib or costal cartilage)(Figs. 1, 2), 늑연골의 현저한 비대칭(prominent asym- metric costal cartilage)(Fig. 3), 연골 주위 결절(parachondral nodule), 연부조직이나 뼈에 의한 흉강의 비대칭(asymmetric thoracic cavity)(Figs. 4, 5), 또는 누두흉이나 새가슴을 포함
Fig. 1. Anterior convexity of the right costal cartilage in a 10-year-old girl clinically diagnosed with rib tumor. Axial CT scan showing asym- metrically protruding right anterior chest wall (arrow).
Fig. 3. Asymmetrically protruding costal cartilage in a 12-year-old boy who visited the hospital for evaluation of chest wall deformity.
Axial CT scan illustrating asymmetrically protruding costal cartilage (open arrow) in left anterior chest wall.
Fig. 4. Asymmetric thoracic cavity due to protruding left chest wall in a 13-year-old boy with a 2-3 year history of palpable mass in the left chest wall. Axial CT scan shows that the left thoracic cavity is asym- metrically larger than the right thoracic cavity.
Fig. 5. Focal lipomatosis in a 12-year-old girl presenting with a poste- rior chest wall lump. Pre-contrast axial CT scan obtained with patient in prone position demonstrates prominent fat deposition (arrow- heads) in the midline of the posterior chest wall and no evident mass.
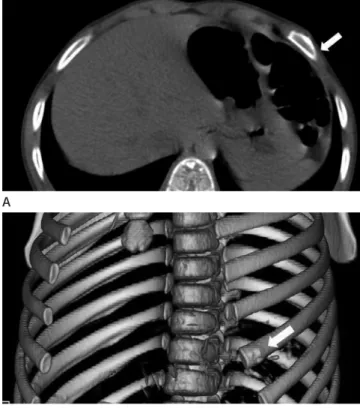
Fig. 2. Bony irregularity of the rib in a 4-year-old boy who presented with a palpable chest wall mass.
A, B. Axial (A) and three dimensional (B) images revealing irregular bony protrusion (arrow) in the anterior portion of the left rib.
A
B
나 갈비뼈에 생기는 화농성 골수염은 종종 주변의 연조직 덩어 리나 골막반응 등과 연관된다. 하지만 이런 소견들은 골파괴가 나타나지 않으면 흉부 X-선 사진에서 보이지 않는다. 골파괴 는 보통 골수염으로 인한 증상이 있는지 1~2주 이내에는 잘 나 타나지 않는다. 하지만 CT나 MR 영상은 쉽게 감염된 골 주위 의 연조직 덩어리를 찾을 수 있어 골파괴가 나타나기 전에 골수 염의 조기진단에 유용하며, 그 외 폐, 흉막, 종격동의 구조물을 평가하는 데 도움을 준다(2).
BCG 림프절염은 BCG를 접종한 후 가장 흔한 합병증으로 이러한 변이들은 임상적으로 큰 의미가 없지만 악성종괴의
가능성을 염두에 두어 소아에서 촉지되는 흉벽종괴가 있을 때 CT나 MRI 같은 영상검사를 시행해야 한다(1-4).
외상
소아의 흉벽은 성인에 비해 연골의 비율이 골화된 뼈의 비율 보다 높기 때문에 높은 탄성도를 가지고 있다. 소아 흉벽의 높 은 탄성도로 인해 외상의 후유증이 성인과는 다르게 나타난다.
첫째로, 빠른 속도의 교통사고로 인한 갈비뼈 골절이 소아에서 발생률이 성인에 비해 낮다. 둘째로, 이러한 사고로 인한 힘이 폐로 분산되기 쉬워 폐좌상이 잘 나타난다. 외상에 의한 혈종이 흉벽종괴로 나타날 수 있다(1).
흉골의 외상은 흔하지 않으며 흉골 부분 전위는 드물다. 흉 골에 외상이 발생하였을 때도 골절이 아닌 흉골의 전위가 보일 수 있다(Fig. 6). 흉골의 전위는 외상에 의해 소아에서만 보일 수 있는 병변으로 이런 경우에도 소아는 만져지는 흉벽종괴로 병원에 내원할 수 있다. 흉골병(sternal manubrium)의 아래 첫 번째 흉골의 몸통에 전위가 가장 잘 생기는데 이는 흉골병은 쇄골과 첫 번째 늑골에 잘 붙어있어 흉골병과 흉골접합부위에 힘이 가해질 때 첫 번째 흉골 몸통으로 힘이 다 전달되기 때문 이다. 흉통이나 숨이 차지 않는 한 수술을 권하지 않으며 부분 전위는 대부분 1년 이내에 원상태로 되돌아온다는 결과들이 보 고된다. 흉골의 부분 전위가 있을 때, CT에서는 첫 번째 흉골 몸통이 돌아간 것을 볼 수 있다(5).
CT는 외상에 의한 흉벽의 혈종, 골절, 흉골 부분 전위가 있을 때 단순 촬영 검사에 비해 병변의 정확한 진단이 가능하다(5).
감염성 질환
흉벽의 연부조직에 생긴 연조직염이나 농양이 소아에서 촉지 되는 흉부종괴로 나타날 수 있다. 포도상구균, 결핵, 녹농균, 방 사선균증, 아스페르길루스 등이 연조직염, 화농성 근염, 농양, 괴사성 근막염 등을 보일 수 있는 흉벽의 화농성 감염에 흔한 원인균들이다. 이 중에 황색 포도상구균과 결핵균이 가장 흔한 균이다(2, 4).
염증은 정도에 따라 연조직염(cellulitis), 육아 조직(granula- tion tissue), 농양을 형성하고 더 심하면 골 파괴와 함께 흉막 외 공간(extrapleural space)까지 침범할 수 있다. 농양의 특징 적인 소견은 중심부에 괴사에 의한 저음영과 조영증강되는 벽 을 보인다(Fig. 7). 폐의 감염(결핵, 진균감염)이나 농흉에 의한 이차적인 골수염의 형태로 나타나기도 한다(2)(Fig. 8). 흉골이
Fig. 7. An infected epidermal cyst in a 3-year-old boy who was born with a palpable mass on the left chest wall. Axial CT scan illustrating a protruded left chest wall due to abscess formation (arrow). Excisional biopsy confirmed the lesion as an epidermal cyst with inflammation.
Fig. 6. Sternal segmental dislocation in a 4-year-old boy presenting with seven-day history of chest wall lump.
A, B. Reformatted (A) and three dimensional (B) images revealing transverse oriented first segment (arrow) of the sternal body.
A
B
성하다가 피부궤양을 남기기도 한다(6). BCG 림프절염은 임 상병력과 초음파를 통해 대부분 진단되기 때문에 CT 영상소 견에 관한 보고가 별로 없다. CT에서는 종괴의 주변부에 조영 증강을 보이고 석회화를 동반할 경우 진단에 도움을 줄 수 있 다(Fig. 9).
액와부에 림프절종대
소아에서 림프절종대는 흔히 볼 수 있는데 경부에 가장 많이 생기고, 액와부와 서혜부 순으로 호발한다. 림프절종대의 원인 은 감염성, 비감염성, 악성으로 분류할 수 있으며 림프절은 기간, 침범부위, 크기에 따라 나뉠 수 있다. 양성의 가장 흔한 원인은 원인불명이 약 60%이며, 원인이 규명된 약 40% 중에서 전염단 핵구증(infectious mononucleosis)과 급성 감염성 림프절염이 가장 흔한 원인이었다(2, 9)(Fig. 10). 감염 중에서 인플루엔자 바이러스와 아데노바이러스는 경부에 양측성 림프절종대를 만 약 60~70%는 액와부에 생기고 약 30%는 쇄골상부에 생긴
다. BCG 림프절염과 결핵성 림프절염은 4주 이상의 기간을 갖고 있는 만성 림프절종대로 나타났으며 다발성이 조금 더 흔 하며 크기는 약 60%에서 1~2 cm이지만 4 cm까지도 커진 다. 화농성과 비화농성으로 구분하며 비화농성은 대부분이 문 제없이 수주 이내 자연치유되지만 화농성은 농루(sinus)를 형 Fig. 8. Chest wall abscesses in a 2-month-old girl.
A. Reformatted coronal image showing one abscess (arrows) in the right chest wall, and a further abscess (arrowheads) in the left supra- clavicular area. Staphylococcus aureus was isolated from the aspirated fluid in the abscess cavity, obtained by ultrasound-guided aspiration.
B. Chest radiograph 20 days later demonstrating permeative bone de- struction (open arrowheads) of the left clavicle, suggesting bone in- volvement of the surrounding abscess.
C. Axial bone setting CT scan clearly showing permeative bone de- struction (open arrow) of the left clavicle, with superior image quality to chest radiograph.
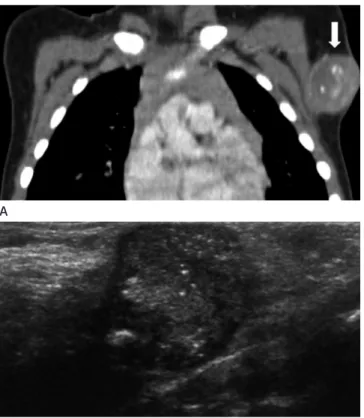
Fig. 9. BCG lymphadenitis in a 22-month-old boy who presented with persistent axillary mass of 7 months’ duration.
A. Coronal reformatted post-contrast image demonstrating a well- marginated, rim-enhancing mass with multiple internal calcifications (arrow) in the left axilla. This was confirmed as chronic granulomatous inflammation by excision.
B. USG showing a circumscribed oval hypoechoic mass with internal calcifications in the left axilla.
Note.-BCG = Bacillus Calmette-Guerin, USG = ultrasonography B
A
C
B A
인다. 조영증강 후 사진에서 균질한 전반적인 조영증강을 보인 다(2)(Fig. 13).
선천성 혈관기형은 정맥성, 림프성, 모세혈관성 기형을 포함 한다. 림프성 기형은 낭포성 활액종(cystic hygroma)과 림프관 종(lymphangioma)이라 불렸지만 최근에 림프성 기형으로 불리 며, 경부와 액와부에 흔히 볼 수 있다(Fig. 14). 몸 전체에 생길 들고 엡스타인-바 바이러스와 거대세포바이러스는 전신에 림
프절종대를 형성할 수 있다. 또한 전신성 홍반성 루푸스와 같은 자가면역질환에서도 액와부의 림프절종대를 보일 수 있다(9).
악성의 원인 중에서는 림프종이 약 70%로 가장 흔한 원인이었 고, 백혈병, 신경모세포종, 조직구증식증(histiocytosis), 횡문 근육종 등이 원인질환이었다(9). 쇄골상부에 림프절종대가 있 거나, 영상소견이나 혈액 검사에서 이상소견을 보이면서 3 cm 이상의 림프절종대가 4주 이상 지속될 때 악성일 가능성이 높 다고 하였다(9). 이와 같이 다양한 원인들에 의해서 림프절종대 가 보일 수 있지만 CT에서는 비특이적인 림프절종대로 보이기 때문에 감별이 쉽지 않다. 하지만 연조직염과 같이 염증이 동반 된 경우는 림프절 주변에 지저분하게 증가된 음영을 동반해 진 단에 도움이 된다(Fig. 10).
종양
흉벽은 근육, 뼈, 연골, 지방, 결합조직, 신경, 혈관, 림프관 등 으로 구성이 되어 있으며 이런 조직들에서 다양한 종양들이 생길 수 있다. 소아에서 흉벽에 발생하는 종양은 연부조직 종양과 골 종양으로 나뉠 수 있다(2).
연부조직 종양
소아 흉벽에서 발생하는 연부조직 종양 중에서 양성종양은 혈 관이상, 데스모이드, 과오종, 표피 봉입 낭종(epidermal inclu- sion cyst), 모기질세포종(pilomatricoma), 섬유종증(fibromato- sis) 등이 있다. 악성종양은 원발성으로 원시신경외배엽종양 (primitive neuroectodermal tumor or Askin tumor)과 횡문 근 육종이 가장 흔하고(2, 4), 전이성은 림프종(Fig. 11), 백혈병, 신경모세포종이 흔하다. 또한 유전질환인 신경섬유종증 제1형 에서 총상 신경섬유종(plexiform neurofibroma)이 흉벽종괴로 나타날 수 있다(Fig. 12).
혈관이상은 소아의 연부조직 종괴의 가장 흔한 원인이다. 혈 관이상은 혈관종과 혈관기형(vascular malformation)으로 나뉜 다. 혈관종은 소아에서 2~3%의 높은 빈도에서 보일 수 있고 저체중인 미숙아의 약 10%에서 보일 수 있다. 혈관종은 출생시 있을 수 있지만 수주 이내에 나타난다. 첫 수개월 후까지 급속한 내피의 성장(rapid endothelial growth)을 하다가 9~10개월에 안정화된다. 그리고 그 이후 7~10년까지 섬유지방성 조직(fi- brofatty tissue)으로 치환된다. 약 90%에서 퇴행해서 소실되지 만 약 10%는 커지기 때문에 치료를 필요로 한다. CT는 사지에 발생한 혈관종의 진단에는 필요하지 않으나 종격동에 발생한 경우 유용하며 보통 경계가 잘 그려지는 소엽모양의 종괴로 보
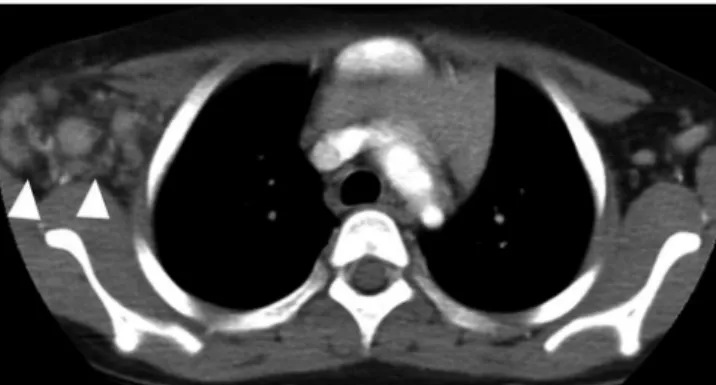
Fig. 10. Acute axillary lymphadenitis in a 6-year-old girl presenting with a two-week history of palpable, growing mass with pain and fe- ver on the right axilla. Axial CT scan illustrates enlarged lymph nodes (arrowheads) with fat infiltration in the right axillary area.
Fig. 11. Burkitt lymphoma in a 12-year-old boy, as diagnosed through biopsy of the abdominal mass. Axial CT scan showing an enhancing mass (arrow) in the right chest wall, and circumferential extensive pleural masses, suggesting a tumor implantation in the chest wall caused by tube thoracoplasty.
Fig. 12. Neurofibromatosis in a 12-year-old boy who had a palpable lesion in the right posterior chest wall. Axial CT scan revealing plexi- form neurofibromatosis (open arrowheads) in the right lower chest wall.
는 골분해 소견과 암죽가슴증이 동반된 것이 진단에 도움이 된 다(2, 4)(Fig. 15).
지방조직 종양은 소아의 연부조직 종양의 약 6%를 차지한 다. 양성은 지방종, 지방모세포종, 지방모세포종증이 있고 악 성은 지방육종이다. 지방종증은 비만인 소아에서 종종 만져지 는 병변으로 내원한다. 대칭적인 미만성 지방종증은 초음파로 쉽게 진단할 수 있으나 국소적인 지방종증과 같이 초음파에서 지방음영이 보이지만 종괴가 분명치 않을 때 CT가 도움이 된 다(8). 지방종이나 국소적인 지방종증은 내부의 결합 조직 중 격(connective tissue septa)에 의해 다양한 소견을 보여서, 초 음파의 진단율은 비교적 높지 않으며 민감도가 약 40~50%, 정확도가 50~60% 정도이다(8). CT에서 지방과 같은 음영을 보이는 종괴의 형태나 현저한 지방 축적을 보여 쉽게 진단할 수 있으며(Fig. 5), 지방종증과 같이 뚜렷한 종괴의 형태가 아 닌 경우 반대편과 쉽게 비교할 수 있다(2). 지방종은 소아의 연 부조직 종양의 4%를 차지하며 지방조직 종양의 66%를 차지 한다. 조직학적으로 정상적인 지방조직과 동일한 성숙된 지방 세포로 구성되지만 1/3에서 결합조직 중격과 석회화가 있다.
지방모세포종은 영아기와 초기 아동기에서 빨리 자라는 비교 수 있는데 약 75%는 두경부에 생기고, 나머지는 흉부와 사지에
나타날 수 있다. 크기는 다양하고 어느 연령에나 생길 수 있으며 천천히 자라지만 출혈이나 감염이 동반되면 갑작스럽게 커질 수 있다. 종종 흉벽에 혈관이나 림프관을 따라서 발생하는 종양으 로 보일 수 있으며 종격동을 침범하기도 한다. 림프관종증에서 Fig. 14. Lymphatic malformation in a 3-year-old girl who had showed a palpable mass on the left axilla one year before. She visited the hospital due to increasing mass size accompanied by pain. Post- contrast axial scan shows a cystic mass (open arrowheads) with no enhancing wall and a soft tissue mass in the left lateral chest wall.
Fig. 13. Infantile hemangioma in a 11-year-old boy admitted for a palpable mass four years ago.
A. Post-contrast axial CT scan (arterial phase) illustrating a lobulated mass (open arrow) without definite enhancement in the left anterior chest wall.
B. Post-contrast axial CT scan (delayed phase) showing diffuse ho- mogenous enhancing mass (open arrow) in the left anterior chest wall.
Fig. 15. Lymphangiomatosis in a 16-year-old boy.
A, B. Axial mediastinal and bone setting CT scan revealing a homoge- nous non-enhancing low density mass in the mediastinum (arrow) and expansile osteolytic lesions on the left side of the ribs (open ar- rows).
A A
B B
해 예후가 좋다. 지방육종은 CT에서 거의 대부분 불균질한 비 지방성 조직을 포함하고 있어 지방종과의 감별에 도움이 된다 (2, 4, 7).
횡문 근육종은 소아, 청소년이나 젊은 성인 등 45세 이하에서 흔히 발생하며 소아에서는 흔히 10세 이전에 발생한다. 두경 부, 비뇨생식계, 서혜부 및 사지연부조직에 흔히 발생하지만 드 물게 흉벽에도 발생한다(Fig. 17). 횡문 근육종은 흉벽에 급속 히 크기가 증가하는 종양으로 신경을 눌러 흉통을 유발한다.
20% 환자에서 뼈의 침범을 볼 수 있다. CT와 MR은 종양의 침범 범위를 보는 데 유용하다(2).
적 흔하지 않은 종양으로 지방조직 종양의 약 30% 정도이다.
조직학적으로 성숙정도가 다양한 지방세포로 이루어져 있다.
여아보다 남아에 흔하며 생후 3세 이전에 진단된다. 사지나 몸 통의 피하지방에 잘 생기지만 몸 어디에도 생길 수 있다(Fig.
16). 영상소견은 지방육종과 감별이 어려우나 소아에서 지방육 종이 아주 드물다. 지방육종은 주로 10대에 생기며 어른에 비 Fig. 17. Rhabdomyosarcoma in a 14-year-old boy who presented with one-week history of dyspnea, tachypnea and swelling of the chest wall. Axial CT scan demonstrating right anterior mediastinal and chest wall masses (arrow), and right axillary lymphadenopathy (open arrow). Note the right pleural effusion with enhancing pleural nodules and thickening.
Fig. 16. Lipoblastoma in a 9-month-old girl who was referred with an incidentally palpable mass.
A, B. Pre-contrast CT scan demonstrates a well-marginated fatty mass with inhomogeneous soft tissue lesion (arrow) in the right ante- rior chest wall.
Fig. 18. Langerhans cell histiocytosis in a 16-year-old boy.
A. Rib radiograph showing an eccentric osteolytic lesion (arrow) in the left 8th rib.
B, C. Axial and sagittal bone setting CT scan demonstrating the ec- centric osteolytic lesion (open arrow and open arrowhead) along the long axis of the left 8th rib.
A
B A
B
C
팽창되고 얇아지며 반투명 음영으로 보인다(2)(Fig. 18). 랑게 르한스세포조직구증은 비교적 드문 질병으로 대부분 소아에서 발생을 하며 종종 늑골을 침범한다. CT에서 팽창하는 골 용해 성 병변으로 흔히 보인다(Fig. 19). 골연골종은 뼈와 연골에 생 기는 양성종양 중 가장 많은 부분을 차지한다. 동맥류뼈낭종은 원발성으로 생기기도 하고 다른 종양의 이차적으로 생길 수 있 다. CT에서 뼈에 얇은 골막반응과 함께 여러 개의 낭성 팽창이 보이고 액체-액체층 소견이 보인다(2, 4)(Fig. 20).
악성종양에서 골파괴와 함께 연부조직 종괴를 형성하거나 양성종양에서 팽창할 때 촉지되는 종괴로 보일 수 있다. Wong 등(4)은 골종양 중 유잉육종과 골연골종(osteochondroma)이 흉벽종괴를 주소로 하였다고 한다. 하지만 흉막 외 공간내로 종괴가 형성될 때는 촉지되는 종괴로 나타나지 않는다. 소아에 서 가장 흔한 원발성 악성 골종양은 유잉육종이며, 림프종, 백 혈병, 신경모세포종에 의한 전이가 원발성 악성 골종양에 비해 더 흔하다(2, 4).
이러한 골종양들의 진단에 CT의 역할은 단순방사선촬영에 서 골의 겹침으로 인하여 잘 보이지 않았을 수 있는 미묘한 피 질골의 침범, 골막반응, 기질의 석회화 특성들에 대한 추가정 보를 줄 수 있다(2, 7).
참고문헌
1. Donnelly LF, Frush DP. Abnormalities of the chest wall in pediatric patients. AJR Am J Roentgenol 1999;173:1595- 1601
2. Jeung MY, Gangi A, Gasser B, Vasilescu C, Massard G, Wi- hlm JM, et al. Imaging of chest wall disorders. Radio- graphics 1999;19:617-637
3. Donnelly LF. Use of three-dimensional reconstructed heli- cal CT images in recognition and communication of chest wall anomalies in children. AJR Am J Roentgenol 2001;
177:441-445
4. Wong KS, Hung IJ, Wang CR, Lien R. Thoracic wall lesions in children. Pediatr Pulmonol 2004;37:257-263
5. Pawar RV, Blacksin MF. Traumatic sternal segment disloca- tion in a 19-month-old. Emerg Radiol 2007;14:435-437 6. Kim DY, Lee SW, Hwang JY. Ultrasonographic features of
BCG lymphadenitis. J Korean Radiol Soc 2005;52:31-36 7. Subhawong TK, Fishman EK, Swart JE, Carrino JA, Attar S,
Fayad LM. Soft-tissue masses and masslike conditions:
what does CT add to diagnosis and management? AJR Am 골종양
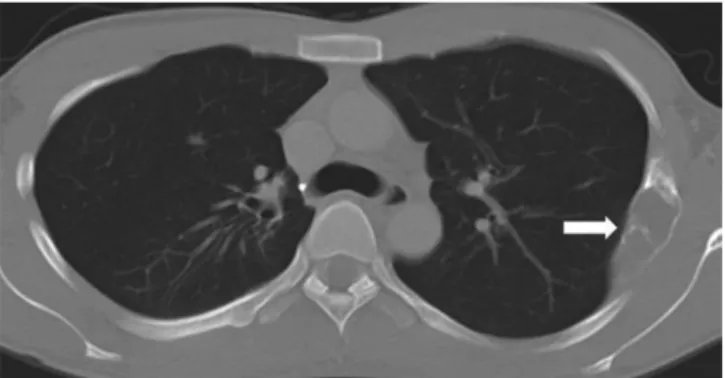
양성 골종양은 섬유형성이상(fibrous dysplasia), 골연골종, 동맥류뼈낭종(aneurysmal bone cyst), 랑게르한스세포조직구 증(Langerhans cell histiocytosis) 등이다. 섬유형성이상은 정상 골조직이 섬유성 조직과 미성숙한 골조직으로 대치되는 양성 섬유성 골성 질환으로 흉벽에 생기는 비신생물성 양성종양의 30%에 달한다. CT에서 부채꼴 모양 골내막에 의해 골피질이 Fig. 19. Fibrous dysplasia in a 18-year-old boy. Axial CT scan with bone setting demonstrating an expansile osteolytic lesion with cortical thinning and endosteal scalloping (arrow) in the left 4th rib.
Fig. 20. Aneurysmal bone cyst in a 13-year-old boy who presented with a palpable mass on the right chest wall one week ago.
A, B. Axial CT scans illustrating an expansile bone tumor (arrow) with fluid-fluid level (open arrow) in the anterior portion of the right rib.
The image with a narrow window width shows the fluid-fluid level more clearly (open arrowhead).
A
B
diology 2004;233:763-767
9. Nield LS, Kamat D. Lymphadenopathy in children: when and how to evaluate. Clin Pediatr (Phila) 2004;43:25-33 J Roentgenol 2010;194:1559-1567
8. Inampudi P, Jacobson JA, Fessell DP, Carlos RC, Patel SV, Delaney-Sathy LO, et al. Soft-tissue lipomas: accuracy of sonography in diagnosis with pathologic correlation. Ra-
소아에서 촉진되는 흉벽종괴의 Multi-Detector CT 소견: 임상화보
1박찬호
1· 김영통
1· 홍현숙
2정상변이에서부터, 선천성 병변, 외상, 감염, 액와부 림프절 종대, 연부조직 종양과 골종양 등의 다양한 질환들이 소아에서 촉지되는 흉벽종괴로 나타난다. 이들 종괴들의 상당수가 흉곽의 구조적인 변이를 동반하므로 이들 질환에서는 이학적 검 사나 초음파 소견만으로는 진단이 어렵다. 따라서 3차원 영상이 가능한 multi-detector CT가 촉지되는 흉벽병변의 특징을 평가하고 감별 진단하는 데 유용하다. 그래서 저자들은 소아에서 촉지되는 흉벽병변으로 나타날 수 있는 질환들을 분류하 고 영상소견을 알아보고자 한다.
1순천향대학교 의과대학 천안병원 영상의학과, 2순천향대학교 의과대학 부천병원 영상의학과