액와는 액와동정맥, 상완신경총 및 림프절이 포함된 상완과 흉벽 사이의 피라미드 형태의 공간으로 다양한 질환이 발생할 수 있다. 액와림프절 종대는 유방암의 전이가 원인인 경우가 많으므로 양성과 악성을 감별하고 조직학적 검사 여부를 결정 하는 것은 매우 중요하다. 액와림프절 종대는 초음파검사로 진 단할 수 있으며 초음파유도 세침검사나 핵생검으로 확진할 수 있다. 저자들은 액와림프절 종대로 나타난 다양한 질환들을 병 리 소견과 비교하고 조직 검사 여부를 결정하는데 도움이 되고 자 한다.
액와림프절 검사방법
액와림프절은 소흉근을 기준으로 세부분으로 나뉘는데 Level I은 소흉근의 하외측면의 하방부위 이며 level II는 소 흉근의 후방 부위이고 level III 는 소흉근의 내측면의 상방이 다(1). 유방촬영술에서 정상 액와림프절은 다양한 크기의 난 원형의 결절로 중심 지방을 가지는 지방문이 보인다. 비정상 액와림프절은 크기가 2 cm 이상이고 높이와 폭이 1.5 이하로 둥글거나 불규칙모양을 가지고 지방문의 소실과 증가한 음영 을 보인다. 그러나 5 cm 이상의 정상 림프절이나 5 mm 이하 의 전이성 림프절도 있을 수 있어 림프절의 크기나 모양으로 양성과 악성을 감별하는 것은 어렵다(1-3). 또한, 유방촬영술 은 커진 림프절이 포함되지 않을 수 있어 신뢰할만한 검사법은
아니다. 초음파검사에서 정상 액와림프절은 얇은 피질과 상대 적으로 큰 지방문을 가지며 지방문 내에 단일 동정맥을 가진다 (Fig. 1). 비정상 액와림프절은 크기가 크고 두껍고 편심성으 로 팽창된 피질을 가지고 지방문이 작거나 소실되어 보인다.
색도플러 초음파검사에서는 지방문에 과혈류를 보이며 악성세 포 침윤으로 폐문 혈관이 파괴되어 주변 혈관들이 커지는 비정 상적인 비문혈류(nonhilar blood flow)를 보이나 이런 소견은 반응성 림프절 종대나 염증에 의해서도 발생할 수 있다(1, 4, 5) (Fig. 2A). 그러므로 초음파검사의 림프절 종대는 양성과 악성 종대가 중복되는 소견을 보일 수 있어 초음파 유도 세침 검사나 핵생검이 유용한 방법이다(1, 5) (Fig. 2B). 액와림프 절의 초음파 유도하에 세침검사나 핵생검은 덜 침습적인 검사 방법으로 유방암 환자에서 전이성 림프절을 예측하는데 높은 민감도, 특이도와 음성예측도를 가진다(5, 6). 세침검사를 사 용한 세포의 확인은 덜 침습적이고 저렴하며 편리한 방법이지 만 시술자의 경험과 경험이 풍부한 세포병리학자가 있어야 하 므로 많은 병원에서 시행하기에는 제한이 있다. 핵생검 역시 안전하고 빠르게 시행될 수 있으며 시술자에게 덜 의존적이고 더 많은 조직을 얻어 면역학적 염색법으로 검사를 시행할 수 있다(5). CT는 림프절 종대를 평가하는데 가장 유용한 방법이 지만 전이를 평가하는 데 있어 믿을만한 림프절 종대의 크기가 정해져 있지 않으며 다양한 민감도와 특이도를 가진다. PET- CT 나 유방 MRI를 이용하는 평가 방법도 시도되고 있으나 제 한적이다.
액와림프절의 다양한 질환의 영상소견과 병리적 소견의 비교
1류근호∙장윤우∙김형환2∙이동화3∙권귀향∙최득린∙황정화∙양승부4
액와림프절 종대는 다양한 양성과 악성 질환들이 원인이 될 수 있으며 염증성 림프절 종대와 전이성 림프절 종대가 대표적이다. 전이성 림프절 종대는 유방암 환자에 매우 중요한 예후 인자 이므로 악성 림프절 종대의 영상의학적 특징을 알고 검사 여부를 결정하는 것은 매우 중요하다.
최근 들어 초음파 유도하에 액와림프절 종대의 조직 검사법이 악성 림프절 종대를 진단하는데 유용하게 사용되고 있다. 저자들은 다양한 질환들로 인한 액와림프절 종대의 영상소견을 병리 적인 소견과 비교하여 특징적인 소견을 알아보고 조직검사의 여부를 결정하는 데 도움이 되고 자 한다.
1순천향대학교병원 영상의학과
3순천향대학교병원 병리과
2천안순천향병원 영상의학과
4구미순천향병원 영상의학과
이 논문은 2009년 11월 13일 접수하여 2010년 1월 17일에 채택되었음.
양성 림프절 종대
반응성 종대 (Reactive Hyperplasia of Lymph Node) 반응성 림프절종대는 염증, 교원 혈관 질환, 육아종성 질환, 후천성 면역 결핍증 이나 실리콘림프절병증 등의 다양한 원인 에 의해 생기며 전신성 질환에 동반되어 생길 경우 양측성 반 응성 종대로 발생한다(2).
결핵 (Tuberculosis)
결핵에 의한 림프절 종대는 두경부나 쇄골하 림프절의 종대 가 흔하며 액와부 종대는 드물다. 결핵에 의한 림프절 종대는 치유되었을 때 석회화를 보일 수 있으며 유방촬영술에서 크기
가 크고 거친 석회화를 동반한 고밀도의 림프절 종대는 결핵성 림프절 종대를 시사할 수 있다(Fig. 3). 유방촬영술에서 석회 화를 동반한 림프절 종대는 결핵성 림프절 외에 석회화성 전 이, 류마티스관절염 치료에 생긴 금침전물 혹은 유방성형 후 삽입된 실리콘의 파열 등을 고려할 수 있다(7). 초음파에서는 크기가 큰 피질의 비후와 지방문의 소실을 보이는 다수의 림프 절 비대를 보이며 내부에 농양을 형성하기도 한다(Fig. 4A).
전이성 림프절 종대, 림프종, 감염성 림프절 종대와 감별할 수 없으나 석회화가 보이거나 융합된 농양형태의 림프절 종대가 보이면 의심할 수 있고 초음파 유도하 조직검사 등을 통한 병 리 검사가 필수적이다.병리소견은 건락괴사와 상피양세포를 보인다(8) (Fig. 4B).
기꾸치병 (Kikuchi’s Disease)
기꾸치병은 1972년 처음 기술되었으며 조직학적으로 괴사
A B
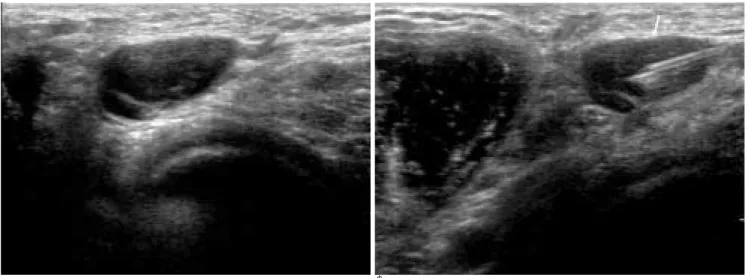
Fig. 2. Reactive hyperplasia of lymph node in a 38-year-old women.
A. Ultrasonography shows enlarged lymph node with eccentrical thickening of cortex and small sized fatty hilum.
B. Ultrasonography guided 20G needle aspiration was performed and pathology reveals reactive hyperplasia of lymph node (white arrow).
Fig. 1. Axillary ultrasonography finding of normal lymph node. Normal lymph node has a smooth, hypoechogenic, thin cortex (white arrow) with a centrally located, preserved rela- tively large sized fatty hilum.
Fig. 3. Tuberculosis in a 50-year-old women.
Mammography shows calcified lymph nodes (black arrows) in both axilla that are possible of sequale of old pulmonary tuber- culosis correlated with past history.
A B Fig. 4. Tuberculosis in a 46-year-old women.
A. Ultrasonography shows abnormal multiple, hypoechoic enlarged lymph nodes (white arrow) with loss of hilar echogenecity.
B. Photography reveals chronic granulomatous inflammation with caseous necrosis (H & E).
A B
C
Fig. 5. Kikuchi disease in a 40-year-old women.
A. Ultrasonography demonstrates a well-circumscribed, round or oval, hypoechogenic masses (white arrows) in left axilla.
Sonoguided biopsy was performed using 14G needle.
B. Contrast enhanced CT with MPR reconstruction image shows several homogeneous enhancing lymph nodes (white arrow) in left axilla.
C. Photography of the biopsied lymph node demonstrates plump histiocytes intermixed with nuclear debris and lymphocytes.
There is an absence of neutrophils and plasma cells (H & E).
성 림프절염으로 특징지어진다. 임상적으로 젊은 여성에서 통 증이 있는 경부 림프절 종대가 흔하며 액와, 복부, 흉부, 골반 등의 림프절 종대도 보일 수 있다. 지속적인 발열, 체중감소, 피부발진, 소화기 증상을 보이나 1-4개월 내에 저절로 호전된 다. 초음파에서는 균질 혹은 비균질 에코의 종괴로 지방문이 유지되어 있으며 동심성 피질 비후를 보이나 비특이적이며 전 이성 림프절과의 감별이 어려워 조직학적 확진이 요구된다(9) (Fig. 5A). CT에서는 균질한 조영증강을 보이며 림프절 주위 지방의 소실을 보일 수 있다(10) (Fig. 5B). 조직학적으로 기 꾸치병은 피질이나 피질 주면의 괴사와 림프절 정상구조의 완 전한 소실을 보이나 과립구(granulocyte), 형질 세포(plasma cell)혹은 호산구(eosinophil)는 보이지 않는다(10) (Fig.
5C).
캐슬만병 (Castleman’s Disease)
캐슬만병은 1956년에 처음 기술된 원인을 알 수 없는 드문 양성 림프증식성 질환이다. 자주 생기는 부위는 종격동이며 액 와부에 발생하는 경우는 약 2%로 드물다. 임상적으로는 국소 성(localized)과 미만성(disseminated)으로 나누며 병리적으 로 초자혈관형(hyaline vascular type)과 형질세포형 (plasma cell type)으로 나뉘는데 91%는 초자혈관형으로 나
타난다. 초음파소견은 단일형의 저에코 종괴이며 색도플러초 음파를 시행하였을 때 혈류의 증가세를 보인다(Fig. 6A). CT 에서는 균일한 조영증강의 종괴로 보인다(Fig. 6B). 병리소견 은 초자혈관형은 잘 발달한 초자 혈관변화를 가지는 종자중심 (germinal center)이 현저하며 형질세포형은 여포간 조직 (interfollicular tissue) 내에 미만성 형질세포(plasma cell) 의 증식을 보인다(Fig. 6C). 영상의학적으로 비특이적인 소견 을 보이므로 조직학적인 확진이 필요하다(11).
톡소포자충증 (Toxoplasmosis)
톡소포자충증은 세포 내 원충인 톡소포자충(Toxopla- smosis gondii)의 감염으로 고양이가 숙주로 알려져 있다. 태 반을 통과하는 감염에 의한 선천적 감염이나 다른 원인에 의한 후천적인 감염에 의해 발생할 수 있으며 임상적으로는 안구의 맥락망막염이 흔하나 증상이 없거나 전신적인 감염을 보일 수 있다(12). 후천적 감염일 경우 경부 림프절 종대가 가장 흔하 며 후두골하방, 쇄골상방, 액와, 서혜부 및 종격동의 림프절 종 대를 보일 수 있다. 증상이 없다면 림프절 종대는 림프종과 유 사하게 보일 수 있으며 액와절 림프절 종대는 유방암의 전이와 도 감별하여야 한다. 초음파 소견은 경계가 분명하고 내부 괴 사가 없으며 균질한 저에코를 보여 비특이적이다(Fig. 7A).
A B
C
Fig. 6. Castleman’s disease in a 65-years-old women
A. Ultrasonography shows several well-circumscribed, ovoid, hy- poechogenic lymph nodes (white arrows) in left axilla.
B. Contrast enhanced CT scan shows the multiple, conglomerated, enlarged lymph nodes (white arrow) with homogeneous enhance- ment in left axilla, level I.
C. Photograph of a histopathologic specimen shows lymphoid fol- licles with stroma of hyperplastic capillaries, venules, and arteri- oles. In the germinal center, there is concentric layering of the multinucleated and pleomorphic follicular lymphocytes around the hyalinized central vessel (H & E).
색도플러에서는 림파절 괴사가 없으므로 지방문의 혈류가 보 인다(13) (Fig. 7B). 병리적으로는 반응성 림프소포 과다형성 (reactive follicularl hyperplasia), 상피모양 조직구종 (epithelioid histiocytes)의 불규칙한 군집 단핵구모양 세포
(monocytoid cell)에 의한 잔기둥글(trabecular sinus)과 피 막하 국소 팽창의 소견을 보인다(Fig. 7C) (12, 13).
A B
C
Fig. 7. Toxoplasmosis in a 44-year-old women
A. Ultrasonography shows enlarged lymph node with cortical thickening and fatty echogenicity in lymph node (white arrow) in hilar portion of left axilla.
B. Color Doppler sonography shows increased hilar vascularity of lymph node.
C. Photography reveals multiple small sized epithelioid granulo- mas (H & E).
A B
Fig. 8. Metastatic lymphadenopathy from breast cancer in a 76-year-old women
A. Ultrasonography shows about 1cm sized, enlarged lymph node (white arrow) with loss of fatty hilum and cortical thickening in right axilla.
B. Contrast-enhanced CT scan shows enhancing LN (white arrow) in right axilla (level I).
악성 림프절 종대
유방암 전이
액와림프절은 유방암에서 가장 흔하게 전이되는 부위로 림 프절 전이 여부는 예후를 결정하는 가장 중요한 인자이다. 초 음파에서 보이는 림프절의 피질 두께, 크기, 모양 및 비문 혈류 를 사용하여 수술 전 림프절 전이를 평가하였을 때 민감도는 35-95%로 다양하게 보고되었다(5, 6). 폐문의 소실은 93%의 양성예측도를 보이나 민감도는 33%로 보고되었다(14). 림프 절 피질의 두께도 림프절 전이를 평가하는 중요한 예측 인자이 며 2.3 mm에서 3 mm를 기준으로 하는 연구들이 있으며 절 대적인 피질의 두께보다는 림프절 단경에 대한 피질의 상대적
인 두께를 측정하는 것이 민감도의 특이도를 모두 만족하게 한 다는 보고가 있다(5, 6).
초음파에서 림프절의 장단경의 비가 1.5이하이거나 편심성 (eccentric)으로 피질의 두꺼워지거나 지방문의 소실을 보이 는 경우 전이성 림프절 종대로 여겨진다(4) (Fig. 8A, 9A).
색도플러 초음파에서 주변부 혈류와 구불거리는 이상형태의 신생혈관들이 악성에서 더 보인다는 보고도 있다(1, 4, 15).
하지만 동심성(contentric) 피질을 가지는 경우 림프절 전이 를 배제할 수 없으므로 초음파 유도 하 액와부 림프절 세침검 사나 핵생검이 전이성 림프절을 평가하는데 이용될 수 있다.
유방암 수술 전 초음파 유도하에 세침검사을 통해 액와림프절 의 전이를 먼저 확인함으로써 감시 림프절을 절개를 따로 시행 할 필요성이 줄어들 수 있으며 보조적 항암치료의 적응증이 될
A B
Fig. 9. Metastatic lymphadenopathy breast cancer in a 37-year-old women
A. Sonography shows enlarged lymph nodes (white arrow) in axilla with subcutaneous and skin nodules (white arrowheads).
B. A enhanced CT scan with MPR reconstruction image shows conglomerated axillary lymph nodes (white arrows) (level I,II and III) with low-density necrotic portions, representing metastases.
A B
Fig. 10. Metastatic lymphadenopathy from breast cancer in a 54-year-old women
A. Sonography shows an enlarged lymph node (white arrow) between the pectoralis major and minor mulscle (Rotter’s node).
B. A multiplanar reformation (MPR) reconstruction image shows metastatic lymph nodes (white arrows) in left axilla level I, II.
Identifying enlarged Rotter’s node can be important because metastases can give rise to chest wall invasion.
A B
Fig. 11. Metastatic lymphadenopathy from melanoma in a 45-year-old women
A. Ultrasonography shows a lobulated heterogeneous hypoechoic mass (white arrow) and daughter nodules in left axillar.
B. Contrast-enhanced CT scan with MPR reconstruction image shows multiple conglomerated, heterogeneously enhanced masses (white arrow) in left axillar.
A
B
Fig. 12. Axillary metastatic lymphadenopathy from primary breast malignant lymphoma in a 43-year-old women
A. Ultrasonography shows lobulating, heterogeneous and hy- poechogenic mass (white arrow) in right axilla.
B. 18F FDG PET CT shows multiple FDG uptake right breast masses (white arrowhead) (SUV 22) and huge right axillary lym- phadenopathies (white arrow) with FDG uptakes.
C. Pathology revealed diffuse proliferation of large atypical lym- phocystes compatible with diffuse large B-cell lymphoma (H&
E).
C
수 있다(16). 감시림프절 생검에서 전이로 판명된 경우 액와부 박리를 시행하는데 수술 전 림프절 전이가 확인된다면 감시림 프절 생검을 시행할 필요가 없어지므로 수술시간을 줄이는 데 도움이 된다(5, 6). CT에서는 편심성으로 불규칙한 피질의 모 양과 장단경의 비가 2 이하는 경우 악성 림프절을 나타내는 중 요한 소견으로 여겨진다(17) (Fig. 8B, 9B). 흉근 내 림프절 (Rotter’s node)은 유방암 환자의 약 10%에서 침범된다(18) (Fig. 10A, B).
유방암 외 악성 전이
대부분의 선암(adenocarcinoma)이 액와림프절로 전이될 수 있으며 폐암, 갑상선암, 위암, 대장암과 췌장암이 전이된다.
악성흑색종은 피부나 볼 점막에서 발생하나 약 5%는 피부 외 에서 발생한다. 액와부위 원발성 흑색종은 드물며 액와부가 침 범되는 경우 다른 부위 흑색종에서 전이된 경우가 더 많다 (19). 유방암 이외의 악성종양의 림프절 전이의 초음파나 CT 의 영상의학적인 소견은 유방암의 전이성 림프절과 감별점은 없다(Fig. 11A, B).
악성림프종
유방의 원발성 악성림프종은 0.1~0.5%로 매우 드물게 보 고되며 다른 부위의 림프종 전이에 의한 이차적 림프종이 더 많다. 유방의 원발성 림프종의 진단은 병리적 확진, 유방조직 과 림프절 침윤이 가까이 존재하며 전신성 림프종이나 이전의 유방 외 림프종이 배제되어야 한다. 유방 촬영에서는 경계가 잘 그려지는 단일 혹은 다발성 결절을 보이며 액와부에 일측성 혹은 양측성으로 군집된 액와부 림프절 종대와 지방문의 소실 을 보인다. 초음파에서는 경계가 잘 그려지는 둥글거나 계란모 양의 균질한 저음영의 종괴로 보이며 낭성괴사로 인해 저음영 의 가낭성 형태로 나타날 수 있다(8) (Fig. 12A). FDG PET- CT 영상은 림프종의 병기와 추적검사에 도움이 된다(20) (Fig. 12B). 유방의 악성림프종은 비호치킨림프종이 대부분 이며 T세포림프종보다 B세포림프종이 더 흔하다(21) (Fig.
12C).
결 론
액와부 림프절종대는 양성 및 악성의 다양한 질환들에 의해 생기며 영상소견은 유사하게 보이므로 감별이 어렵다. 액와림 프절이 둥글고 지방문의 소실을 보이며 피질이 편심성으로 두 꺼워진 종대를 보이더라도 영상 소견은 양성질환과 악성 전이 를 감별하는데 비특적이므로 초음파 유도하의 세침검사나 생 검 등을 통한 조직학적 확진이 요구된다.
참 고 문 헌
1. Abe H, Schmidt RA, Sennett CA, Shimauchi A, Newstead GM. US- guided core needle biopsy of axillary lymph nodes in patients with breast cancer: why and How to do it. Radiographics 2007;27:S91-
S99
2. Lee JY, Kim EK, Kim MJ, Youk JH, Oh KK. Imaging findings of palpable benign masses in axilla. J Korean Soc Med Ultrasound 2006;25:21-29
3. Shetty MK, Carpenter WS. Sonographic evaulation of isolated ab- normal axillary lymph nodes identified on mammography. J Ultrasound Med 2004;23:63-71
4. Yang WT, Chang J, Metreweli C. Patients wit breast cancer: differ- ences in color Doppler flow and gray-scale US features of benign and malignant axillary lymph nodes. Radiology 2000;215:568-573 5. Abe H, Schmidt RA, kulkarni K, Sennet CA, Mueller JS, Newstead
GM. Axillary lymph nodes suspicious for breast cancer metastasis:
sampling with US-guided 14-gauge core-needle biopsy-clinical ex- perience in 100 patients. Radiology 2009;250:41-49
6. Deurloo EE, Tanis PJ, Gilhije KG, Muller SH, Kro¨ger R, Peterse JL, et al. Reduction in the number of sentinel lymph node procedures by preoperative ultrasonography of the axilla in breast cancer. Eur J Cancer 2003;39:1068-1073
7. Muttarak M, Pojchamarnwiputh S, Chaiwun B. Mammographic features of tuberculous axillary lymphadenitis. Australas Radiol 2002;46:260-263
8. Kim HJ, Kim KW, Park YS, Chung DJ, Cho YJ, Hwang CM, et al.
Spectrum of axillary disorders (Excluding metastasis from breast cancer): radiolgical and pathological correlation: a pictorial essay. J Korean Radiol Soc 2007;57:583-594
9. Youk JH, Kim EK, Ko KH, Kim MJ. Sonographic features of axil- lary lymphadenopathy caused by kikuchi disease. J Ultrasound Med 2008;27:847-853
10. Kwon SY, Kim TK, Kim YS, Lee KY, Lee NJ, Seol HY. CT findings in kikuchi disease: analysis of 96 cases. AJNR Am J Neuroradiol 2004;25:1099-1102
11. Bui-Mansfield LT, Chew FS, Myers CP. Angiofollicular lymphoid hyperplasia (Castleman’s disease) of the axilla. AJR Am J Roentgenol 2000;174:1060
12. Eapen M, Mathew CF, Aravindan KP. Evidence based criteria for the histopathological diagnosis of toxoplasmic lymphadenopathy. J Clin Pathol 2005;58:1143-1146
13. Ridder GJ, Boedeker CC, Lee TK, Sander A. B-mode sonographic criteria for differential diagnosis of cervicofacial lymphadenopathy in cat-scratch disease and toxoplasmosis. Head Neck 2003;25:306- 312
14. Shin JH, Choi HY, Moon BI, Sung SH. In vitro sonographic evalua- tion of sentinel lymph nodes for detecting metastasis in breast can- cer: comparison with histopathologic results. J Ultrasound Med 2004;23:923-928
15. Bedi DG, Krishnamurthy R, Krishnamurthy S, Edeiken BS, Le Petross H, Fornage BD, et al. Cortical Morphologic features of axil- lary lymph nodes as a predictor of metastasis in breast cancer: in vitro sonographic study. AJR Am J Roentgenol 2008;191:646-652 16. Sapino A, Cassoni P, Zanon E, Fraire F, Croce S, Coluccia C, et al.
Ultrasonographically-guided fine-needle aspiration of axillary lymph nodes: role in breast cancer management. Br J Cancer 2003;88:702-706
17. Uematsu T, Sano M, Homma K. In vitro high resolution helical CT of small axillary lymph nodes in patients with breast cancer: corre- lation of CT and histology. AJR Am J Roentgenol 2001;176:1069- 1074
18. Oran I, Memis A, Ustun EE. Ultrasonographic detection of inter- pectoral (Rotter’s) node involvement in breast cancer. J Clin Ultrasound 1996;24:519-522
19. Easson AM, Rotstein LE, Mccready DR. Lymph node assessment in melanoma. J Surg Oncol 2009;99:176-185
20. Schaefer NG, Hany TF, Taverna C, Seifert B, Stumpe KD, von Schulthess GK, et al. Non-Hodgkin lymphoma and Hodgkin dis- ease:coregistered FDG PET and CT at staging and restaging-do we need contrast-enhanced CT? Radiology 2004;232:823-829
21. Uesato M, Miyazawa Y, Gunji Y, Ochiai T. Primary non-Hodgkin’
s lymphoma of the breast: report of a case with special reference to 380 cases in the japaneses literature. Breast Cancer 2005;12:154- 158
J Korean Soc Radiol 2010;62:501-509
Address reprint requests to : Yun-Woo Chang, M.D., Department of Radiology, Soonchunhyang University Hospital 22 Daesakwan-gil, Yongsan-gu, Seoul 140-743, Korea.
Tel. 82-2-709-9396 Fax. 82-2-709-3928 E-mail: [email protected]
Radiologic Findings of Various Diseases of the Axillary Lymph Node with Pathologic Correlations
1Guen Ho Ryu, M.D., Yun-Woo Chang, M.D., Hyung Hwan Kim, M.D.2, Dong Wha Lee, M.D.3, Kui Hyang Kwon, M.D., Deuk Lin Choi, M.D., Jung Hwa Hwang, M.D., Seung Boo Yang, M.D.4
Departments of 1Radiology, 3Pathology, Soonchunhyang University Hospital Departments of Radiology, 2Soonchunhyang Cheonan Hospital, 4Soonchunhyang Gumi Hospital
Axillary lymphadenopathy has multiple variable pathologic conditions such as a malignant or benign condi- tion. It is important that we determine the radiologic findings of malignant lymphadenopathy and in turn de- termine the further course of evaluation for the lesion, because metastatic axillary lymphadenopathy repre- sents an important prognostic factor. Recently, an ultrasonographic-guided axillary lymph node biopsy has been widely used as a diagnostic tool. We discuss the radiologic and pathologic findings of variable axilla dis- eases and outline the specific findings for determining the results of a lymph node biopsy.
Index words :Axilla
Lymphatic system Radiography