J Korean Soc Phys Med, 2016; 11(1): 53-60 http://dx.doi.org/10.13066/kspm.2016.11.1.53
Online ISSN:
Print ISSN:
2287-7215 1975-311X
Research Article Open Access
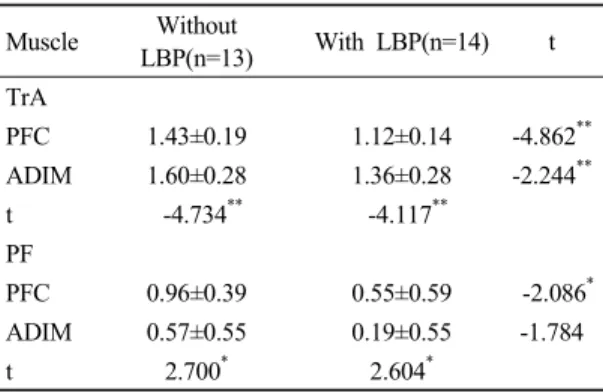
요통유무에 따른 복부 드로우인과 골반바닥근 수축훈련이 배가로근과 골반바닥근에 미치는 영향
전체 글
요통유무에 따른 복부 드로우인과 골반바닥근 수축훈련이 배가로근과 골반바닥근에 미치는 영향
수치
관련 문서
복장뼈,
반지층 (Basement Floor) 1층 (Ground Floor)... Nishizawa
고관절 : 관골의 관골구(acetabulum)과 femur head sacroiliac joint: sacrum + ilium.. pubic symphysis : pubic + pubic
Preoperative evaluation of pelvic lateral lymph node of patients with lower rectal cancer: comparison study of MR imaging and CT in 53 patients?.
Effects of Nitroglycerin(Ni) on Spontaneous Activity(S.A) and Oxytocin (OT) Induced Contractions in the Uterine Smooth Muscle. Data are expressed as mean
In the change of physical strength, The exercise group showed statistically significant differences in muscle strength(right), muscle strength(left),
The improvement factors of the performance showed significant increase in muscle strength, muscle endurance, cardiovascular endurance, power, agility and
In the health fitness category of the adult women who underwent instrument pilates exercise, they were statistically significant in muscle strength,
