Minimally Invasive Cardiac Surgery versus Conventional Median Sternotomy for Atrial Septal Defect Closure
6
0
0
전체 글
(2)
(3)
(4)
(5)
(6)
수치
관련 문서
► See the article “Reversibility of Pulmonary Hypertension Following Surgical Atrial Septal Defect Closure in Children with Down Syndrome” in volume 27 on page 247... In an
The 2-dimensional (2-D) echocardiography in right parasternal long axis view revealed right atrial (RA) dilation (Fig. 3A) and interventricular septal flatten- ing to
Minimal, minimally invasive transforaminal lumbar interbody fusion (MI-TLIF); Open, conventional open surgery... 1-5,15) 반면에, 최소침습적 경추간공 요추 추체간
► See the article “Early to Mid-Term Follow-Up Outcomes of Percutaneous Closure of Atrial Septal Defects Using Recent Generation Devices: a Single-Center Experience” in volume 49
Iatrogenic VSD following concomitant septal myectomy with AVR is not a common complication, and may warrant closure. A po- tential mechanism leading to iatrogenic VSD following
The different deployment method in atrial septal defect (ASD) patients with central defect and anterosuperior (AS) rim defect. With sufficient rims, 87% of procedure was
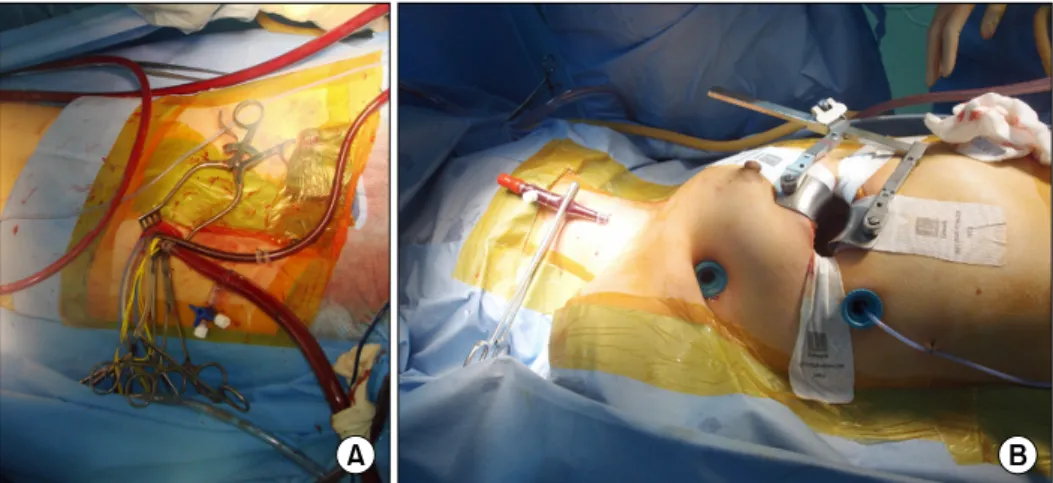
Background: This study aims to evaluate whether or not the method of right vertical axillary minithoracotomy (RVAM) is preferable to and as reliable as conventional
The PVRIs after closure with fenestration were over 3.0 Wood units*m 2 in 11 patients (64.7%), and their pre-closure PVRI, mPAP with oxy- gen, and pre-closure Qp/Qs values
