심근경색증을 유발한 좌심방 점액종 1예
4
0
0
전체 글
(2) 당 94회, 호흡수는 분당 24회, 체온 37.8℃였다. 심음. 적인 T wave inversion이 있었고(Fig. 1) 심 초음파. 은 규칙적이고 심잡음은 들리지 않았고 호흡음은 정상. 검사 상 심실 구혈률은 40%로 좌심실의 전중격의 심첨. 이었다. 심전도상 Ⅱ, Ⅲ, aVF와 V2에서 V6까지 대칭. 부와 하벽의 중간하부에서 무운동 소견을 보였으며 좌 심방에 3.85×1.75 cm 크기의 점액종이 관찰되었다(Fig. 2). 응급실에서 시행한 혈액 검사상 creatine kinase치 는 264U/L로 MB isoenzyme분절은 9 U/L, Troponin (+)였으며 이후 추적 검사상 creatine kinase와 MB isoenzyme분절 모두 감소하는 양상이었다. 내원 2일 후 환자는 갑작스런 양안의 시력 저하가 발생하였고, 뇌 자기 공명 검사 상 우측 대뇌 후두엽과 시상에 급성 뇌. Fig. 1. Marked symmetric T wave inversion in II, III, aVF and precordial leads V2-V6.. 경색 소견이 있었고 우측 소뇌와 시상에 과거 뇌경색에 의한 뇌연화 소견을 보였다(Fig. 3). 내원 4일 후 관상 동맥 조영술상 좌전하행지 원위부의 갑작스런 완전 폐 쇄와 우측 관상동맥의 후하행분지 원위부의 아전 폐쇄 소견을 보였다(Fig. 4). 환자는 내원시부터 항응고제 등 을 이용한 보전적 치료 후, 뇌경색 및 심근경색에의한 증상 완화되어 좌심방 절개술과 중격 절제술로 점액종 을 제거하는 수술을 시행하였고 현재 흉통이나 의식소 실의 재발 없이 경과관찰 중으로 추적 심초음파 검사상 좌심실 전중격과 하벽의 무운동 소견도 호전되었다.. 고 Fig. 2. Two-dimensional transthoracic echocardiogram. Parasternal long axis view showed a 3.85×1.75 cm sized homogenous hyperechoic mass (white arrow) arising within LA chamber. LA: left atrium.. A. 찰. 좌심방의 점액종은 심장에서 발생하는 가장 흔한 종 양으로 심장과 심낭에 관련된 모든 종양의 약 25%를. B. Fig. 3. Brain MRI showed high signal intensity in right occipital lobe and thalamus (white arrow) in T2WI (A) and diffusion (B) image, which represent acute infarction. MRI: magnetic resonance imaging.. 513.
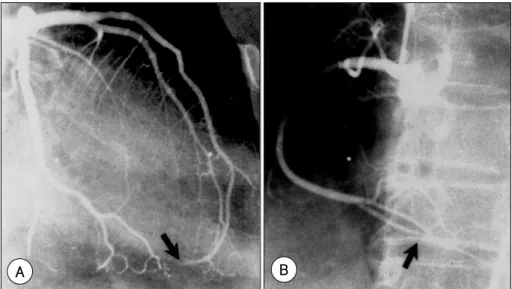
(3) B. A. Fig. 4. Left coronary angiogram (AP caudal view) showed an abrupt occlusion (arrow) of distal left anterior descending artery due to the fragment of myxoma (A). Right coronary angiogram (RAO cranial view) showed a subtotal occlusion (arrow) of PDA branch due to the fragment of myxoma (B).. A. B. Fig. 5. Scanty cellular tumor with abundant amorphous extracellular matrix are attached to the endocardium by a broad base (A). Scattered collections of myxoma cells in various groupings within abundant amorphous extracellular matrix (B). 1-3). 차지한다.. 점액종의 일반적인 임상 양상은 주로 뇌. 1)6). 크기, 위치, 부착 부위 등을 알 수 있다.. 심방 점액. 혈관과 말초혈관에 관련된 전신 색전증과 좌심방에서. 종의 관상동맥 색전증의 진단은 관상동맥 조영술에서. 좌심실로의 혈류 이동을 막는 승모판 협착의 증상과 비. 심근경색과 연관된 관상동맥 내의 색전에 의한 갑작스. 1-5). 슷한 심장 내 폐쇄의 형태로 나타난다.. 이러한 환자. 런 완전 폐쇄와 filling defect 소견이 보이면 진단할 수 5)7)8). 들에서 심초음파를 이용해 좌심방 점액종을 진단하는. 있다.. 데 심초음파를 통해 점액종의 진단 뿐 아니라 점액종의. 률은 0.006%로 이처럼 극히 낮은 유병률은 대동맥의. 514. 점액종의 합병증 중 관상동맥 색전증의 발생. Korean Circulation J 2004;34(5):512-515.
(4) 혈류의 방향과 관상동맥 기시부의 방향이 일반적으로. 행 관동맥에 같이 발생한 색전증은 보고 된 바 없다. 이. 직각을 이루어 색전이 관상동맥 내로 유입될 가능성이. 에 저자 등은 좌심방 점액종이 관상동맥의 좌전하행지. 떨어지는 것과 심장의 수축기 동안 관상동맥 기시부가. 원위부와 우 관동맥의 후하행분지 원위부로 색전증을. 열린 대동맥 판막들에 의해 보호되는 것, 그리고 관상. 일으켜 전중격과 하벽 심근 경색증이 발생된 환자를 경. 동맥으로 혈액의 유입이 대부분의 혈류가 이미 관상동. 험하였기에 문헌 고찰과 함께 보고 하는 바이다.. 맥 기시부를 지난 이완기에 이루어지는 것 등으로 설명 3)4). 하고 있다.. 4). 그리고 Panos 등 은 우측 관상동맥의. 색전증이 좌측 관상동맥 색전증에 비해 2배 정도 많은 것으로 보고하였는데 이것은 대동맥내 혈류에 대한 우 측 관상동맥 기시부의 위치가 비교적 색전증을 더 잘 일으킬 수 있기 때문인 것으로 설명하고 있다. 국내에 9). 서는 1998년 이 등 에 의해 관동맥 조영술상 정상인 환자에서 급성 심근경색의 원인이 점액종에 의한 색전 으로 추정되는 증례를 보고하였다. 본 예는 심전도상 Ⅱ, Ⅲ, aVF와 V2에서 V6까지 대칭적인 T wave inversion이 있었고, 심초음파 검사상 전중격부와 하벽부 의 무운동, 그리고 관동맥 조영술 상 우관동맥과 좌전 하행 관동맥의 거의 말단부위에 폐쇄 소견을 확인 할 수 있어 점액종의 색전에 의한 급성심근경색으로 진단 하였다. 심근효소 수치가 다소 낮은 것은 아마도 색전 증이 우관동맥과 좌전하행 관동맥의 거의 말단부위에 폐쇄를 일으켰기 때문으로 생각된다.. 요. 약. 심방 내 점액종의 전신 색전증은 비교적 흔하나, 관 상동맥 색전증은 극히 드물고 특히 우관동맥과 좌전하. 중심 단어:점액종;색전증;심근 경색증. REFERENCES 1) Rhim HY, Youn HJ, Park JW, Kim HY, Jeon HK, Lee SW,. Kim YH, Lim SH, Jung HO, Chang KY, Seung KB, Kim CM, Chae JS, Kim JH, Hong SJ, Choi KB. Clinical experience of cardiac myxoma. Korean Circ J 1999;29:1317-23. 2) Reynen K. Cardiac myxomas. N Engl J Med 1995;333:1610-7. 3) Lehrman KL, Prazon GB, Ullyot D. Atrial myxoma presenting as acute myocardial infarction. Am Heart J 1985;110: 1293-5. 4) Panos A, Kalangos A, Sztajzel J. Left atrial myxoma presenting with myocardial infarction: case report and review of the literature. Int J Cardiol 1997;62:73-5. 5) Tomita Y, Endo T, Takano T, Hayakawa H, Sugisaki Y. Extensive hemorrhagic mypcardial infarction associated with left atrial myxoma. Cardiology 1992;81:384-8. 6) Abascal VM, Kasznica J, Aldea G, Davidoff R. Left atrial myxoma and acute myocardial infarction: a dangerous duo in the thrombolytic agent era. Chest 1996;109:1106-8. 7) Rath S, Har-Zahav Y, Battler A, Agranat O, Neufeld HN. Coronary artery embolus from left atrial myxoma. Am J Cardiol 1984;54:1392-3. 8) Tanabe J, Williams RL, Dietrich EB. Left atrial myxoma: association with acute coronary embolization in an 11 years old boy. Pediatrics 1979;63:778-81. 9) Lee JM, Lee HS, Jun EJ, Youn HJ, Chung WS, Oh YS, Kim CM, Kim JH, Choi KB, Hong SJ, Lee KY, Shim SI. A case report of myocardial infarction in myxoma patient with normal coronary arteries. Korean Circ J 1998;28:1624-9.. 515.
(5)
수치

관련 문서
(A and B) Total occlusion of proximal left anterior descending artery (LAD) (red arrow) and significant stenosis in left circumflex artery (LCX) (white arrows), (C) Right
Left coronary angiogram with cranial angulation (AP cranial) view shows 60% stenosis of the mid left an- terior descending artery.. 5) 본 증례의 경우 에서도 환자는
One Case of Left Anterior Descending Artery Fistula-Right Ventricle Complicating Rotablator Atherectomy with Spontaneous Occlusion in a Following Coronary Angiogram Rak Kyeong Choi,
Selective right coronary angiogram D shows a left circumflex artery arrow arising as a terminal extension of right coronary artery.. A:RAO view, B:AP view with cranial angulation,
(A) Angiography showed abrupt occlusion and extravasated dye mate- rial of right popliteal artery (arrow).. (B) Post
Coronary angiogram shows significant stenosis of left main, left anterior descending, and left circumflex coronary arteries.. 감소된
(A–C) Coronary angiography before the stent insertion and balloon dilation shows chronic total occlusion of the left anterior descending artery (white arrow), left circumflex
(A) (Blank arrow) Coronary angiogram with AP caudal view revealed tight stenosis of the ostium of the left main coronary artery... Taka- yasu's arteritis: a
