https://doi.org/10.12997/jla.2017.6.2.97
pISSN 2287-2892 • eISSN 2288-2561
JLA
Double Right Coronary Arteries Originated from Separate Ostia with Total Occlusive Lesion in One of the Two Right Coronary Arteries
Jaehoon Chung, Hack-Lyoung Kim, Woo-Hyun Lim, Jae-Bin Seo, Joo-Hee Zo, Myung-A Kim, Sang-Hyun Kim
Division of Cardiology, Boramae Medical Center, Seoul National University College of Medicine, Seoul, Korea
Double right coronary arteries (RCA) are very rare congenital anomalies of coronary artery. We report a case of double RCA with total occlusion, incidentally found by collateral flows. A 71-year-old patient underwent percutaneous coronary intervention of left coronary arteries for angina, and the presence of double RCA was missed at initial coronary angiography (CAG). About 20 months later, second CAG was performed due to recurrent angina, and the CAG showed newly developed collateral flow suggesting the presence of the other missed RCA. There was a total occlusion at missed RCA and the lesion was successfully revascularized with drug eluting stent. If there was no collateral flow, the other RCA could not be found and its critical lesion could not be managed properly. Our case suggests that collateral flow can be a useful clue in detecting coronary anomaly. Besides, it is important to fully understand coronary anatomy, not to miss uncommon coronary lesion.
(J Lipid Atheroscler 2017 December;6(2):97-101)
Key Words: Congenital heart disease, Acute coronary syndrome, Percutaneous coronary intervention
Received:
Revised:
Accepted:
July 10, 2017 August 16, 2017 September 21, 2017
Corresponding Author: Sang-Hyun Kim, Division of Cardiology, Department of Internal Medicine, Boramae Medical Center, Seoul National University College of Medicine, 20 Boramae-ro 5-gil, Dongjak-gu, Seoul 07061, Korea Tel: +82-2-870-2216, Fax: +82-2-870-3866, E-mail: [email protected]
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
INTRODUCTION
The prevalence of congenital anomalies of coronary artery has been reported to be 0.6%-1.3% of the patients undergoing invasive coronary angiography (CAG).1-3 Among congenital coronary anomalies, the double right coronary arteries (RCA) are very rare. It has been reported that the incidence of double RCA was 0.01% in general population during CAG.4 Herein, we report a case of double RCA from different ostia, which presented as an angina due to total occlusive lesion in one of the two RCAs.
CASE REPORT
A 71-year-old male visited emergency department due to two days of exercise induced chest pain. He had hypertension and 40 pack-year of smoking history. On his physical examination, there was a grade IV mid-systolic ejection murmur at right upper sternal border radiating to right neck. At presentation, cardiac enzymes were elevated (Troponin I 1.51 ng/mL [normal range: ≤0.04 ng/mL], creatinine kinase-MB 6.4 ng/mL [normal range:
≤6.3 ng/mL]), and abnormal Q waves in V1 to V3 with nonspecific ST-T segment changes in V5 and V6 were
Fig. 1. Patient’s electrocardiogram at first presentation.
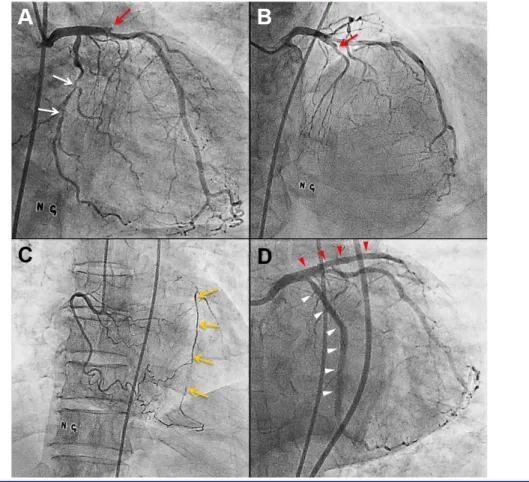
Fig. 2. Coronary angiography at initial presentation. (A and B) Total occlusion of proximal left anterior descending artery (LAD) (red arrow) and significant stenosis in left circumflex artery (LCX) (white arrows), (C) Right coronary artery with collateral flow (yellow arrows) to LAD, and (D) revascularized LAD (red arrow heads) and LCX (white arrow heads) after percutaneous coronary intervention with drug eluting stents.
shown in electrocardiography (ECG) (Fig. 1). In trans- thoracic echocardiography, left ventricular ejection
fraction was 45% by biplane method, and there were regional wall motion abnormalities suggesting multi-
Fig. 3. Patient’s electrocardiogram at second presentation.
Fig. 4. Coronary angiography at the second presentation. (A and B) Left coronary angiogram showing collateral arteries to right coronary artery (RCA) territory (yellow arrows), (C) detected total occlusive lesion in distal segment of the missed RCA (red arrow), and (D) revascularized missed RCA after percutaneous coronary intervention with drug eluting stents (white arrow heads).
vessel territory ischemia: mid to apical septal and anterior wall contractions were akinetic with wall thinning, and
mid anterolateral wall and apical lateral wall contractions were hypokinetic. Moderate degree of aortic valve stenosis
was also observed. As acute coronary syndrome (ACS) was suspected, urgent invasive CAG was performed. In CAG, there was chronic total occlusion in proximal left anterior descending artery (LAD), and multiple significant stenosis in distal left circumflex artery (LCX) (Fig. 2A and 2B). RCA was relatively hypo-plastic, but there was no significant stenosis and good collateral flows to LAD was observed (Fig. 2C). Based on ECG, echocardiography and CAG findings, LCX was suspected as culprit vessel rather than LAD for the event. Thus, percutaneous coronary intervention (PCI) for LCX was done firstly, and then PCI for LAD was also done successfully with drug-eluting stents (Fig. 2D). The patient was discharged from the hospital one day after PCI with free of symptom, and received regular follow-up every three months with medications including aspirin, clopidogrel, beta-blocker, and statin.
About 20-month later, the patient visited outpatient department earlier than scheduled with newly developed chest pain and dyspnea in daily activity which had begun one week ago. ECG change was not significant compared with previous ECG (Fig. 3), and cardiac enzyme levels were not elevated. In transthoracic echocardiography, there were newly developed hypokinetic motion of basal to mid inferior walls of left ventricle, and previous moderate degree aortic stenosis progressed to severe degree. The left ventricular ejection fraction was decreased from 45% to 38%. To rule out coronary lesion, invasive CAG was performed. In CAG, left coronary angiogram showed no significant change except new collateral flow from LAD to RCA, and course of collateral flow was not matched to previously observed RCA (Fig. 4A and 4B).
We reviewed previous CAG and found that the previously observed RCA course was not matched to general RCA.
It flowed to right ventricular wall. It was variant of right ventricular branch which originated from aorta with separate ostium (Fig. 2C). We had misjudged this right ventricular branch as hypoplastic RCA. Overall, these findings suggested the existence of true RCA with separate
ostium. After cautious manipulation of catheter, the RCA ostium was found. CAG showed total occlusion at distal segment of newly found RCA (Fig. 4C). PCI for the RCA was done successfully with drug-eluting stents (Fig. 4D).
As patient refused surgical aortic valve replacement or transcatheter aortic valve replacement, the patient discharged one day after PCI and are on regular follow-up without symptom.
DISCUSSION
Congenital coronary anomalies are present about 1%
of the general population undergoing CAG. In one study enrolling 126,595 patients, rate of congenital coronary anomalies is 1.6% but, no case of a double RCA was reported.3 Another study with 7,400 patients, 0.46% had congenital coronary anomalies and there was just one case of double RCA.4 Several terms were used including
“double right coronary artery”, “duplicated right coronary artery”, “dual right coronary artery” and “split right coronary artery”. Nonetheless, there is no scientific consensus over the definition and correct diagnosis of a double RCA.5 Chien et al. divided double RCA into two groups based on whether the double RCA originated from a single ostium or from separate ostia. To our best knowledge, a total of 18 cases of double RCA from separate ostia have been reported since first report by Guepta et al.
in 1987.6,7 As it is very rare coronary anomaly, the correct diagnosis of double RCA based on conventional CAG is challenging, and thus, further imaging tests such as computed tomography are frequently needed.8 Most of congenital coronary anomalies are considered benign. But, some may be associated with serious complications, such as ACS, ventricular arrhythmias, congestive heart failure and sudden cardiac death.9-11 In this case, the patient had ACS due to total occlusion of one of the RCA with collateral from LAD. Fortunately, missed RCA could be detected by collateral vessels showing different flow direction than
we expected, and the patient escaped the danger by successful revascularization. It is important for the inter- ventional cardiologist to keep in mind this abnormality, in order to avoid wrong diagnosis and inadequate treat- ment, especially in case of abnormal course of arterial flows. And if we have paid more attention to abnormal course of previously observed RCA, we could have found significant coronary lesion before occurrence of ACS. This case suggests that collateral flow can be useful as a clue to detect coronary anomaly. Besides, fully aware of coronary anatomy is important, not to miss uncommon coronary lesion.
REFERENCES
1. Garg N, Tewari S, Kapoor A, Gupta DK, Sinha N. Primary congenital anomalies of the coronary arteries: a coronary: arteriographic study. Int J Cardiol 2000;74:
39-46.
2. Topaz O, DeMarchena EJ, Perin E, Sommer LS, Mallon SM, Chahine RA. Anomalous coronary arteries: angio- graphic findings in 80 patients. Int J Cardiol 1992;34:
129-138.
3. Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography.
Cathet Cardiovasc Diagn 1990;21:28-40.
4. Harikrishnan S, Jacob SP, Tharakan J, Titus T, Kumar VK, Bhat A, et al. Congenital coronary anomalies of origin
and distribution in adults: a coronary arteriographic study. Indian Heart J 2002;54:271-275.
5. Chen YF, Chien TM, Chen CW, Lin CC, Lee CS. Double right coronary artery or split right coronary artery? Int J Cardiol 2012;154:243-245.
6. Chien TM, Chen CW, Chen HM, Lee CS, Lin CC, Chen YF. Double right coronary artery and its clinical implications. Cardiol Young 2014;24:5-12.
7. Gupta SK, Abraham AK, Reddy NK, Moorthy SJ.
Supernumerary right coronary artery. Clin Cardiol 1987;
10:425-427.
8. Soydinc S, Sari I, Davutoglu V. The dilemma in diag- nosing double right coronary artery: contribution of multidetector computed tomography. Int J Cardiol 2008;
126:132-133.
9. Basso C, Maron BJ, Corrado D, Thiene G. Clinical profile of congenital coronary artery anomalies with origin from the wrong aortic sinus leading to sudden death in young competitive athletes. J Am Coll Cardiol 2000;35:1493- 1501.
10. Davis JA, Cecchin F, Jones TK, Portman MA. Major coronary artery anomalies in a pediatric population:
incidence and clinical importance. J Am Coll Cardiol 2001;37:593-597.
11. Ozeren A, Aydin M, Bilge M, Dursun A, Onuk T. Athero- sclerotic double right coronary artery and ectasia of left coronary arteries in a patient with presented acute coronary syndrome and ventricular tachycardia. Int J Cardiol 2005;102:341-343.