대한외과학회지:제 68 권 제 1 호
□ 원 저 □
Vol. 68, No. 1, January, 2005
35
서 론
림프절의 전이 여부는 대장암의 병기를 결정하는 데 가 장 중요한 인자인데 통상적으로 림프절의 절제 후 헤마톡 실린-에오신(H&E) 염색을 이용하여 림프절의 전이 상태를 평가한다. H&E 염색으로 림프절의 전이유무를 정확하게 파악하는 것은 어렵기 때문에 면역조직화학적 검사가 병행 되기도 한다. 그러나 절제된 모든 림프절을 대상으로 연속 절편 및 면역조직화학적 검사를 하는 것은 많은 비용과 시 간이 소모될 것이다. 따라서 전체 림프절을 조사하는 것보 다는 원발 종양에서 처음으로 배출되는 감시림프절을 대상 으로 집중적인 조직검사를 시행하면 효과적으로 림프절의 전이 유무를 알 수 있을 것이다. 저자들은 대장암에서 감시 림프절 생검을 시행하여 그 유용성을 알아보고 전이가 없 는 감시림프절의 연속절편을 통해 미세전이를 검사하여 감 시림프절 생검의 민감도 및 위음성률을 알아보고자 본 연 구를 하였다.
방 법
2002년 3월부터 2003년 9월까지 결장 및 직장암환자 82 명을 대상으로 생체 외 lymphatic mapping 및 감시림프절 생 검을 하였다. 림프절 곽청술을 포함한 대장암 절제 후 5분
대장암에서 체외 감시림프절 생검의 의의
원광대학교 의과대학 외과학교실 및 1병리학교실
박 원 철․이 정 균․한 원 철1
Ex Vivo Sentinel Node Mapping in Colorectal Cancer
Won Cheol Park, M.D., Jeong Kyun Lee, M.D. and Won Cheol Han, M.D.1
Purpose: Lymph node analysis is essential for staging colorectal cancer. Intraoperative lymphatic mapping and sentinel lymphadenectomy remain to be investigated for most gastrointestinal neoplasms. Previous attempts to identify the sentinel node (SN) in solid tumors have used intraoperative techniques. This study describes a novel approach to identify the SN in colorectal cancer using ex vivo lymphatic mapping.
Methods: Eighty-two colorectal cancer patients underwent ex vivo lymphatic mapping and a sentinel lymph node biopsy using isosulfan blue dye following a standard surgical resection between March 2002 and September 2003. Within 5 minutes of resection, colorectal specimens were sub- mucosally injected with isosulfan blue dye in four quadrants.
Blue lymphatic channels were identified in the mesentery, and followed to the blue-stained SN(s), which were har- vested. The specimens were fixed in formalin and sub- sequently analyzed in the usual fashion. In patients with T1 or T2 tumors, which were blue-stained nodes, but negative to hematoxylin and eosin staining, were further analyzed by serial section and immunohistochemical staining (IHC).
Results: At least one SN was identified in 79 patients of the 82 patients (96.3%). The average number of SNs identified per patient and nodes in each colorectal cancer specimen were 3 (range, 1∼7) and 17.1 (range: 11∼47).
Thirty five patients had lymph nodes containing a metastatic disease. Thirteen patients had metastases in both sentinel and nonsentinel nodes. There were 7 sentinel lymph nodes as the only site of metastatic disease. In 15 patients the sentinel nodes were negative for disease, whereas the
nonsentinel lymph nodes contained a metastatic disease (false negative rate = 42.9%). The false negative rates of SN(s) metastasis in the 26 patients with T1 or T2 tumors were 16.7 and 7.7% by H&E and by serial section and IHC.
Conclusion: Ex vivo mapping of the colon is technically feasible, and may provide a useful approach to evaluate lymph node metastasis in patient with T1 or T2 colorectal cancers. (J Korean Surg Soc 2005;68:35-38)
Key Words: Ex vivo sentinel node mapping, Colorectal cancer 중심 단어: 체외 감시 림프절 생검, 대장암 ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Departments of Surgery, 1Pathology, School of Medicine, Wonkwang University, Iksan, Korea
책임저자:박원철, 전북 익산시 신용동 344-2
ꂕ 570-711, 원광대학교 의과대학 외과학교실 Tel: 063-850-1205, Fax: 063-855-2386 E-mail: [email protected]
접수일:2004년 6월 5일, 게재승인일:2004년 10월 2일 이 논문은 2004년도 원광대학교 교비지원에 의해서 연구됨.
36 대한외과학회지 : 제 68 권 제 1 호 2005
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
이내에 생염료(LymphazurinⓇ, USSC. Norwalk, USA) 1 mL 를 이용하여 병변 주위 4방향의 점막하층에 각각 0.25 mL 의 생염료를 주입하였다. 생염료 주입 후 장간막에서 가장 먼저 청색으로 착색되는 림프절을 찾아 절제하고 그 위치 를 기록하였다. 절제된 감시 림프절 및 대장 조직은 통상적 인 H&E 염색을 하였다. H&E 조직검사상 T1, T2 에서 전이 가 없는 감시림프절을 대상으로 40μm 간격으로 3부위 각 각 2개씩 절편을 만든 후, H&E와 cytokeratin 면역조직화학 적 염색을 하여 미세전이 유무를 관찰하였다. 면역조직화 학적 염색 일차 항체는 high and low molecular-weight cyto- keratin (Clone AE1/AE3, ZyMed)을 사용하였다.
결 과
환자의 평균 연령은 61.8세(범위 40∼83)였고, 남자가 50 명, 여자가 32명이었다. 조직학적 병기는 T1 3명, T2 23명, T3 56명이었다. 평균 감시 림프절의 수는 3개(범위 1∼5)였
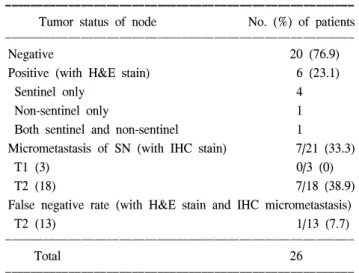
고 평균 체취된 림프절의 수는 17.1개(범위 11∼47)였다 (Table 1). 감시림프절 체취는 총 82명 중 79명(96.3%)에서 성공하였고, 3명은 찾지 못했는데 3명 모두 T3이었다. 감시 림프절을 찾은 79명 중 35명(44.3%)이 림프절 전이가 있었 는데 이 중 15명(false negative rate: 42.9%)은 감시 림프절 전이 없이 림프절에 전이가 있었고, 7명(20.0%)은 감시 림 프절에만 전이가 있었다. 감시림프절 전이의 위음성률은 T1 0명(0/0, 0%), T2에서 1명(1/6, 16.7%), T3에서 14명(14/29, 48.3%)으로 T 병기가 높을수록 의의 있게 높았다(P=0.02) (Table 2). T1, T2에서 전이가 없는 21명에서 감시림프절을 대상으로 연속절편 및 면역조직화학적 검사를 시행한 결과 T1 0 (0/3)명, T2 7 (7/18)명(38.9%)에서 미세전이가 발견되 었고. 미세전이를 포함하면 위음성률은 T2에서 1명(1/13, 7.7%)이었다(Table 3).
고 찰
악성 흑색종과 유방암 환자에서 최소 침습적인 감시림프 절 절제는 림프절의 전이가 없는 환자에서 불필요한 림프 절 절제를 하지 않아 림프 부종, 신경손상 및 운동제한 등의 합병증을 감소시킬 수 있는 장점이 있다고 보고되었다.(1,2) 일반적으로 대장암에서 림프절의 절제 범위와 합병증과의 관계는 관련이 없다고 보고되고 있으나 직장암에서는 수술 후 성기능 장애 및 배뇨장애가 보고되고 있다.(3,4) 수술 가 능한 대장암의 가장 중요한 예후 인자는 림프절의 전이 여 부인데 림프절의 전이가 없을 경우 대장암 특히 직장암에 서도 광범위 림프절 절제를 생략하고 감시림프절을 포함한 최소한의 림프절 절제만 시행하면 수술 후 출혈, 성기능 및 비뇨기 합병증을 감소시킬 수 있을 것이다.
수술시 림프절의 전이 여부나 범주를 정확히 알기 어렵 Table 1. Clinicopathologic feature of patients
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
Features Results
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
No. of cases 82
Sex
male:female 50:32
Mean age, year (range) 61.8 (40∼83)
T stage
T1 3 (3.7%)
T2 23 (28.0%)
T3 56 (68.3%)
Mean no. of lymph nodes (range) 17.1 (11∼47) Mean no. of sentinel nodes (range) 3.0 (1∼5) ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Table 2. Distribution of metastasis in sentinel and non-sentinel lymph nodes
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ Tumor status of node No. (%) of patients ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Negative 44 (55.7)
Positive 35 (44.3)
Both sentinel and non-sentinel 13 (37.1)
Sentinel only 7 (20.0)
Non-sentinel only (false negative) 15 (42.9) False negative
T1 (0) 0
T2 (6) 1/6 (16.7)
T3 (29) 14/29 (48.3)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Total 79
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Table 3. Distribution of metastasis in sentinel and non-sentinel lymph nodes in T1, T2 tumors
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ Tumor status of node No. (%) of patients ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Negative 20 (76.9)
Positive (with H&E stain) 6 (23.1)
Sentinel only 4
Non-sentinel only 1
Both sentinel and non-sentinel 1
Micrometastasis of SN (with IHC stain) 7/21 (33.3)
T1 (3) 0/3 (0)
T2 (18) 7/18 (38.9)
False negative rate (with H&E stain and IHC micrometastasis)
T2 (13) 1/13 (7.7)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Total 26
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
박원철 외 : 대장암에서 체외 감시림프절 생검의 의의 37 ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 기 때문에 수술 후 림프절 전이 유무를 확인하고 있는데
수술 중 림프절의 전이 여부를 알 수 있다면 수술의 범위를 정할 수 있을 것이다. 최근에는 내시경적 점막절제술이 시 도되고 있는데 림프절의 전이 여부를 정확히 알 수 없는 것이 그 한계이다. 또한 복강경보조 하에 대장암 수술을 시 행하는데 수술시 림프절 전이 여부를 알 수 있다면 불필요 한 림프절 절제를 하지 않아도 될 것이다. 그러나 현실적으 로 대장암에서 감시림프절을 정확하게 찾는 것은 여러 가 지 불편한 검사를 시행해야 하고 그 정확도에도 차이가 있 는 것으로 보고되고 있다.(5-7)
감시림프절을 찾는 방법은 99mTc sulfur colloid를 이용하 는 방법과 생체염료를 이용하는 방법 등이 이용되고 있으 며 악성 흑색종과 유방암에서는 이 두가지 방법을 같이 사 용할 때 감시림프절을 발견하는 율이 높다고 보고되고 있 다.(8,9) Merrie 등(10)은 대장암 환자에서 99mTc sulfur colloid 와 생체염료를 같이 사용하여 감시림프절 생검을 시행한 결과 26명의 환자 중 23명(88%)에서 감시림프절을 발견하 였다고 보고하였다. 대장암에서 감시림프절을 찾기 위해
99mTc sulfur colloid를 이용하는 방법은 수술 2시간 전에 내 시경을 이용하여 99mTc sulfur colloid를 주사해야 하고 장비 가 준비되어져야 하므로 환자 및 의사의 불편함이 뒤따른 다.(11,12) Wood 등(5)은 75명의 대장암 환자를 대상으로 생 체염료를 이용한 lympahtic mapping (LM)을 하였는데 in vivo LM 64명 중 56명(88%)에서 감시림프절을 찾았고 ex vivo LM으로 8명 중 7명(88%)에서 감시림프절을 찾을 수 있었다고 보고하였다. Wong 등(13)은 대장암 환자를 대상 으로 생체염료를 이용한 ex vivo LM으로 26명의 환자 중 24명에서 감시림프절을 찾을 수 있었다고 보고하였다. 저 자들은 림프절 곽청술을 포함한 대장 절제 후 5분 이내에 생체염료를 주입하는 방법을 이용하여 총 82명 중 79명 (96.3%)에서 감시림프절을 찾았다. 이 방법은 림프절 절제 를 시행 한 후 생체 염료를 주사하기 때문에 림프절 절제를 시행하기 전에 생체염료를 암세포 주위에 주사함으로 인한 암세포의 확산 가능성을 피할 수 있고 비교적 쉽게 감시림 프절을 찾을 수 있다.(13)
H&E 염색에서 전이가 없는 경우 약 20%에서 면역조직 화학적 염색을 시행하면 미세전이가 발견된다고 보고되는 데 절제된 모든 림프절을 대상으로 연속절편과 면역조직화 학적 염색을 시행하면 비용과 노력이 더 들게 된다.(14-16) 따라서 감시림프절만을 대상으로 연속절편 및 면역조직화 학적 염색을 시행하면 더 효과적으로 림프절의 전이유무를 알 수 있을 것이다. 본 연구에서는 감시림프절의 미세전이 가 T1, T2에서 33%에서 발견되었는데 미세전이와 환자의 예후와의 관계는 아직 논란이 있고 더 연구해야 할 것으로 생각한다. 유방암에서는 생체염료를 종양 주위에 주사하거 나 유륜 하에 주사하거나에 상관없이 감시림프절의 위치가 대부분 액와 부위에 존재하는 것으로 보고되고 있으나 위
장관은 다양한 림프 경로를 가지고 있기 때문에 감시림프 절의 위치가 다양하게 존재할 수 있다.(11,17,18) 따라서 위 장관 종양은 유방암에 비해서 skip metastasis가 비교적 높게 보고되고 있지만 T1, T2에서는 아주 낮게 보고되고 있다.
본 연구에서 T1, T2에서 감시림프절 전이 없이 림프절 전이 가 있는 위음성률이 25.0%였고 면역조직화학적 염색에 의 한 미세전이를 포함할 경우 9.1%였다. 따라서 T1, T2 에서 감시림프절만을 대상으로 연속절편 및 면역조직화학적 검 사를 시행하면 림프절 전이를 효과적으로 발견할 수 있다 고 생각하며 향후 더 많은 증례를 대상으로 연구해야 할 것이다.
결 론
대장암에서 체외 lymphatic mapping과 감시림프절 생검은 쉽고, T병기가 증가할수록 감시림프절의 위음성률이 높아 지므로 T1, T2를 대상으로 감시림프절 생검을 시행하면 림 프절의 전이여부를 효율적으로 파악할 수 있다고 생각되나 향후 T1, T2의 더 많은 증례를 대상으로 연구해야 할 것이 다.
REFERENCES
1) Morton DL, Wen DR, Wong JH, Economou JS, Cagle LA, Storm FK, et al. Technical details of intraoperative lymphatic mapping for early stage melanoma. Arch Surg 1992;127:392- 9.
2) Giuliano AE, Kirgan DM, Guenther JM, Morton DL. Lym- phatic mapping and sentinel lymphadenectomy for breast can- cer. Ann Surg 1994;220:391-8; discussion 398-401.
3) Matsuoka N, Moriya Y, Akasu T, Fujita S. Long-term outcome of urinary function after extended lymphadenectomy in patients with distal rectal cancer. Eur J Surg Oncol 2001;27:165-9.
4) Maeda K, Maruta M, Utsumi T, Sato H, Toyama K, Matsuoka H. Bladder and male sexual functions after autonomic nerve- sparing TME with or without lateral node dissection of rectal cancer. Tech Coloproctol 2003;7:29-33.
5) Wood TF, Saha S, Morton DL, Tsioulias GJ, Rangel D, Hutchinson W Jr, et al. Validation of lymphatic mapping in colorectal cancer: in vivo, ex vivo, and laparoscopic tech- niques. Ann Surg Oncol 2001;8:150-7.
6) Bilchik AJ, Saha S, Wiese D, Stonecypher JA, Wood TF, Sostrin S, et al. Molocular staging of early colon cancer on the basis of sentinel node analysis: a multicenter phase II trial.
J Clin Oncol 2001;19:1128-36.
7) Paramo JC, Summerall J, Wilson C, Cabral A, Willis I, Wodnicki H, et al. Intraoperative sentinel lymph node map- ping in patients with colon cancer. Am J Surg 2001;182:40-3.
8) Morton DL, Thompson JF, Essner R, Elashoff R, Stern SL,
38 대한외과학회지 : 제 68 권 제 1 호 2005
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Nieweg OE, et al. Validation of the accuracy of intraoperative
lymphatic mapping and sentinel lymphadenectomy for early- stage melanoma: a multicenter trial. Ann Surg 1999;230:453- 65.
9) Choi UJ, Park WC, Lee KM, Yoon KJ. Occult micrometastasis of sentinel lymph node in node-negative breast cancer. J Ko- rean Surg Soc 2001;61:379-86.
10) Merrie AE, van Rij AM, Phillips LV, Rossaak JI, Yun K, Mccall JL. Diagnostic use of the sentinel node in colon cancer.
Dis Colon Rectum 2001;44:410-7.
11) Kitagawa Y, Watanabe M, Hasegawa H, Yamamoto S, Fujii H, Yamamoto K, et al. Sentinel node mapping for colorectal cancer with radioactive tracer. Dis Colon Rectum 2002;45:
1476-80.
12) Arnaud JP, Bergamaschi R, Schloegel M, Ollier JC, Haegele P, Grob JC, et al. Progress in the assessment of lymphatic spread in rectal cancer. Rectal endoscopic lymphoscintigraphy.
Dis Colon Rectum 1990;33:398-401.
13) Wong JH, Steineman S, Calderia C, Bowles J, Namiki T. Ex vivo sentinel node mapping in carcinoma of the colon and rectum. Ann Surg 2001;233:515-21.
14) Cutait R, Alves VA, Lopes LC, Cutait DE, Borges JL, Singer J, et al. Restaging of colorectal cancer based on the identi- fication of lymph node micrometastases through immunope- roxidase staining of CEA and cytokeratins. Dis Colon Rectum 1991;34:917-20.
15) Greenson JK, Isenhart CE, Rice R, Mojzisik C, Houchens D, Martin EW Jr. Identification of occult micrometastases in pericolic lymph nodes of Dukes’B colorectal cancer patients using monoclononal antibodies against cytokeratin and CC49.
Correlation with long-term survival. Cancer 1994;73:563-9.
16) Broll R, Schauer V, Schimmelpenning H, Strik M, Woltmann A, Best R, et al. Prognostic relevance of occult tumor cells in lymph node of colorectal carcinoma: an immunohisto- chemical study. Dis Colon Rectum 1997;40:1465-71.
17) Tsioulias GJ, Wood TF, Morton DL, Bilchik AJ. Lymphatic mapping and focused analysis of sentinel lymph nodes upstage gastrointestinal neoplasms. Arch Surg 2000;135:926-32.
18) Kosaka T, Ueshige N, Sugaya J, Nakano Y, Akiyama T, Tomita F, et al. Lymphatic routes of the stomach demon- strated by gastric carcinoma with solitary lymph node metas- tasis. Surg Today 1999;29:695-700.