266
책임저자:홍성화, 서울시 동대문구 회기동 1번지
130-702, 경희의료원 외과 Tel: 02-958-8264, Fax: 02-966-9366 E-mail: [email protected]
접수일:2007년 4월 18일, 게재승인일:2007년 5월 14일 본 논문의 요지는 2006년 대한외과학회 추계학술대회에서 포스 터 발표되었음.
담관내 유두상 점액 종양
경희대학교 의과대학 외과학교실, 1병리학교실
박선진ㆍ권택수ㆍ주선형ㆍ김윤화1ㆍ이상목ㆍ홍성화
Intraductal Papillary Mucinous Neoplasm of the Bile Ducts
Sun Jin Park, M.D., Taek Soo Kwon, M.D., Sun Hyung Joo, M.D., Youn Wha Kim, M.D.1, Sang Mok Lee, M.D.
and Sung Wha Hong, M.D.
Intraductal papillary mucinous neoplasms of the bile ducts (IPMNs-B) are uncommon lesions that are characterized by innumerable papillary fronds that contain fine vascular cores, enriched mucin production and bile duct dilatation. IPMNs-B are histologically similar to intraductal papillary mucinous ne- oplasms of the pancreas and they are occasionally asso- ciated with hepatolithiasis. IPMNs-B are considered to be rel- atively low- grade malignancy and they merit consideration for aggressive surgery. Thus, early and precise diagnosis is important to maximize patient survival. From July 2002 to March 2006, we identified four patients with IPMNs-B at our hospital. In three patients, intrahepatic or extrahepatic bile duct stones were associated with their condition. Computed tomography and magnetic resonance cholangiography were done in all four cases and this demonstrated marked dilata- tion of the biliary tree. Endoscopic retrograde cholangiog- raphy was done in two cases and a large amount of mucin that was draining from the patulous orifice of the duodenal papilla was seen on endoscopy. However, two cases were initially misdiagnosed as intrahepatic cholangiocarcinoma or choledochal cyst with intrahepatic bile duct stones. All the cases underwent ipsilateral hemihepatectomy with caudate lobectomy. Histologically, one case showed to be adenoma, one case was borderline and two cases were invasive adenocarcinoma. (J Korean Surg Soc 2007;73:266-271) Key Words: Intraductal papillary mucinous neoplasms of the
bile ducts, Low-grade malignancy, Hepatolith- iasis
중심 단어: 담관내 유두상 점액 종양, 저등급 악성, 간 내담석증
Departments of Surgery and 1Pathology, College of Medi- cine, Kyung Hee University, Seoul, Korea
서 론
이미 잘 알려진 췌관내 유두상 점액 종양(Intraductal pap- illary mucinous neoplasm of the pancreas)은 다량의 점액을 분비하고 관내 성장을 하는 유두상 종양을 특징으로 하는 질환이다. 임상적, 조직학적으로 이와 매우 유사하면서 담 관 상피에서 유래하는 담관내 유두상 점액 종양(Intraductal papillary mucinous neoplasm of the bile ducts)은 드문 질환으 로서 최근 진단 기술의 발달로 보고가 증가하고 있으며, 대 부분의 보고는 한국, 대만, 일본 등의 동아시아 국가에서 이 루어지고 있다. 담관내 성장형 간내담관암(Intraductal growth type intrahepatic cholangiocarcinoma), 담관 유두종증(Biliary papillomatosis), 점액을 생성하는 간내담관암(Mucin-produc- ing intrahepatic cholangiocarcinoma) 등은 담관내 유두상 점 액 종양과 유사한 질환이라고 할 수 있다.(1-3) 담관내 유두 상 점액 종양은 점막에 국한되어 악성도는 낮지만 후기에 이르면 침윤 암종으로 발전할 수 있고, 담관암과는 달리 수 술적 절제 후 높은 생존율을 기대할 수 있으므로 정확한 조기 진단이 중요하다.(4,5) 저자들은 4예의 담관내 유두상 점액 종양을 경험하였기에 이를 보고하는 바이다.
증 례
남자가 2예, 여자가 2예로 남녀비는 1:1이고 평균 연령 은 59세(범위, 46∼69세)였다. 임상 증상은 우상복부 동통이 2예, 고열이 3예, 황달이 3예에서 있었다(Table 1). 과거 병력 상 3예에서 담낭절제술을 시행 받았고 2예에서 간내담석증 의 기왕력이 있었으며, 1예에서 총담관담석증이 술 전 검사 로 발견되었다. 컴퓨터 단층 촬영과 자기공명 담췌관 조영 술에서 간 내 담관 또는 간외 담관의 확장된 소견이 4예에서 관찰되었고, 그 중 2예에서는 담관 내 종괴가 관찰되었으며,
박선진 외:담관내 유두상 점액 종양 267
Table 1. Clinicopathologic features of 4 patients with IPMN-B
Case 1 Case 2 Case 3 Case 4
Age 58 46 69 62
Sex M F M F
History Hepatolithiasis Hepatolithiasis CBD stone
Cholecystectomy Cholecystectomy Cholecystectomy
Symptoms/signs Fever Jaundice Fever Fever
Abdominal pain Weight loss Abdominal pain
Jaundice
ERCP No Yes No Yes
MRCP Yes Yes Yes Yes
Cholangiographic Dilatation in IHD (L>R) Dilatation in LIHD Diffuse dilatation in IHD Dilatation in LIHD
findings and CBD and CBD and CBD
Multiple small filling defects Amorphous filling defect Multiple small filling defects in CHD Mucin drainage CT findings Dilatation in LIHD Dilatation in LIHD Diffuse dilatation in IHD Dilatation in LIHD
and CBD and CBD and CBD
Suspicious mass in LIHD Small mass in LIHD Mass in CHD CBD stones
IHD stones Multiple LN enlargements
Initial impression Hepatolithiasis & choledochal cyst IPMN-B or mucinous CC Klatskin tumor IPMN-B
Operation L Hemihepatectomy L Hemihepatectomy R Hemihepatectomy L Hemihepatectomy
Pathology IPMN-B carcinoma, invasive IPMN-B borderline IPMN-B carcinoma, invasive IPMN-B adenoma
Type of epithelium Pancreaticobiliary Gastric Intestinal Gastric
Outcome Alive, 42 months Recurred, 7 months Alive, 15 months Alive, 10 months
Died, 13 months
IPMN-B = intraductal papillary mucinous neoplasm of the bile ducts; CC = cholangiocarcinoma; IHD = intrahepatic duct; CHD = common hepatic duct; CBD = common bile duct; L = left; R = right; adenoca = adenocarcinoma; LN = lymph node; IPMN-B carcinoma = intraductal papillary mucinous carcinoma.
2예에서 간 내 또는 간외 담석증이 관찰되었다(Fig. 1, 2).
내시경적 역행성 담도 조영술은 2예에서 시행되어 십이지 장 유두의 팽창된 모습과 다량의 점액 배출, 그리고 담도에 서 무정형의 결손 음영이 관찰되었고(Fig. 3), 이 중 1예에서 담즙 검사상 간흡충(Clonorchis sinensis) 감염이 확인되었다.
수술 전 영상검사에서 담관내 유두상 점액 종양이 의심된 경우는 2예가 있었고, 1예에서 간내담석증을 동반한 총담 관낭이 의심되었으며, 1예는 간내담관암으로 의심되었다.
수술은 4예에서 간엽절제술(좌엽절제술 3예, 우엽절제술 1예)과 미상엽절제술, 그리고 총담관절제술 및 림프절절제 술을 시행하였다. 병리학적 소견은 육안으로 모든 예에서 담관이 심하게 확장되어 있었으며, 강내로 다양한 크기의 두상의 종괴가 돌출되어 있고 점액이 차 있었다. 조직학적 으로 유두상의 종괴는 2예에서는 위형세포, 1예는 장형세 포, 그리고 1예는 췌담관형세포로 구성되어 있었다. 다양한 형태의 이형성증을 가지고 있었는데, 1예는 저등급의 이형 성증을 가진 선종, 1예는 고등급의 이형성증을 가진 경계성 종양, 2예는 기질 내 침윤을 보이는 암종이었다. 수술 후 3 예에서 각각 10개월, 15개월, 42개월째 추적 관찰 중이며, 1예에서는 수술 후 7개월째 다발성 골전이가 의심되고 액 와림프절의 전이가 발견되었으나 치료 거부 후 13개월 째
사망하였다.
고 찰
담관에서 발생하는 신생물 중에서 관 내 성장을 하는 유 두상 종양(Intraductal papillary neoplasm of the bile duct)은 미세한 섬유혈관 중심(fine fibrovascular cores)을 갖는 담관 의 비정형 상피의 유두상 성장을 특징으로 하며 빈번하게 다량의 점액을 생성하기도 한다.(6,7) 이러한 담관내 유두상 종양 중에서 점액을 다량 분비하는 종양에 대한 개념이나 명칭은 아직까지 확립되어 있지 않지만, 현재로서는 담관 내 유두상 점액 종양(Intraductal papillary mucinous neoplasm of the bile ducts)이라는 용어가 가장 흔하게 사용되고 있 다.(8)
담관내 유두상 점액 종양은 미세한 섬유혈관 중심을 감싸 는 수많은 엽상의 유두상 주름(frondlike papillary infoldings) 을 특징으로 한다.(9) 서서히 성장하면서 점막 표면을 따라 퍼지는 경향을 띠며 후기에는 담관벽을 침습하기도 하는 데, 이형성에서 침윤 암종에 이르기까지 다양한 조직학적 소견을 갖는다.(4,7) 종양은 부스러지기 쉽고 탈락하는 경향 을 띠어서 담석증이나 재발성 화농성 담관염으로 오인할
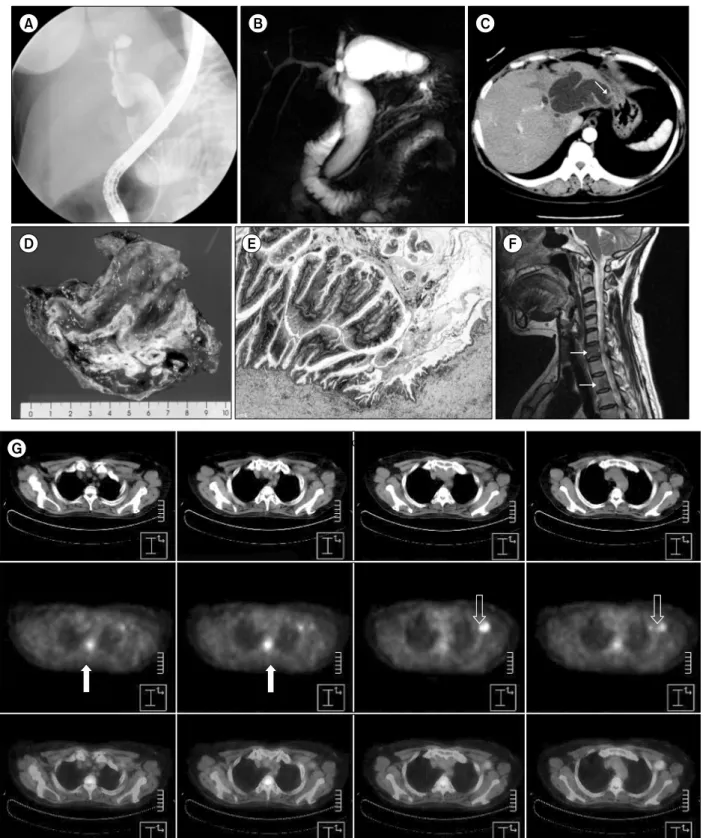
Fig. 1. A 46-year-old woman who presented with jaundice and had a previous history of hepatolithiasis. (A) ERCP shows dilatation of the extrahepatic bile duct and amorphous filling defect. (B) Coronal MRCP image shows marked dilatation of the extrahepatic bile ducts and aneurysmal dilatation of the left intrahepatic bile ducts. (C) CT image shows marked dilatation of the left intrahepatic bile ducts and a suspicious mass in dilated duct (arrow). (D) The resected specimen shows the markedly dilated hepatic ducts with focal nodular mass containing mucin products. (E) Microphotograph shows papillary growth of tumor tissues composed of gastric type epithelium with high grade dysplasia. Stromal invasion is not noted. (H&E stain, ×100) (F), (G) Postoperatively, cervical MR image and PET show multiple bone metastases (arrows) and axillary lymph node metastasis (open arrow).
Fig. 1. Continued.
박선진 외:담관내 유두상 점액 종양 269
수 있는 담관 폐색을 일으킬 수 있고,(5,9,10) 다량의 점액이 담즙의 흐름을 방해하여 이로 인해 폐색성 황달이 일어나 고 담관염이나 담석으로 악화될 수 있다.(1)
담관내 유두상 점액 종양은 이미 잘 알려진 췌관내 유두 상 점액 종양(intraductal papillary mucinous neoplasm of the pancreas)과 매우 유사하다. 즉, 유두상 표면을 갖는 종양의 관 내 성장과 점액의 과분비, 그리고 담관의 이차적인 확장 및 수반되는 임상증상뿐만 아니라 침윤성 선암과의 연관성 은 서로 공통되는 특징이다.(5,8,11) 이것은 담관과 췌관이 발생학적 기원이 공통되기 때문이라고 생각되는데,(12) Zen 등(13)은 두 가지 종양에서 점액핵심단백(mucin core protein)과 cytokeratin의 발현 형태가 유사하다고 하였으며, 관내 유두상 점액 종양이 담관과 췌관에서 동시에 발견되 었다는 보고도 있다.(14,15)
아직까지 담관내 유두상 종양을 분류하는 확립된 기준은 없으나, Chen 등(6)은 담관 상피의 비정형 정도에 따라 4가 지 형태로 분류하였는데 1형은 경도의 이형성을 갖는 경우, 2형은 고도의 이형성, 3형은 상피내암과 미세침윤암, 그리 고 4형은 침윤암을 보이는 경우이다. 3형은 담관내 성장형 간내담관암(intraductal growth type of intrahepatic cholangio- carcinoma)과 상응한다고 할 수 있고, 4형은 기질 침습을 갖
는 담관내 성장형뿐만 아니라 담관내 유두상 선암의 요소 를 갖는 종괴형성형(mass-forming type)과 담관침윤형(peri- ductal infiltrating type) 간내담관암까지 포함된다고 하였다.
본 연구자들은 췌관내 유두상 점액 종양에 대한 세계보건 기구의 분류를 바탕으로,(16) 선종(IPMN-B adenoma), 경계 성 종양(IPMN-B boderline), 그리고 침윤이 없는 상피내암 (intraductal papillary mucinous carcinoma, noninvasive, IPMN- B carcinoma, noninvasive)과 침윤암(IPMN-B carcinoma, inva- sive)으로 분류하였다.
간내담석증과의 연관성이 보고되고 있는데, Nakanuma 등 (7)은 담관내 유두상 종양은 간내담석증과 원발성 경화성 담관염, 그리고 간의 기생충증 등의 담관의 만성 염증성 질 환에서 더욱 빈번하게 발생한다고 하였고, Chen 등(6)은 만 성 증식성 담관염과 말초 담관 폐색이 간내담석증을 동반 한 담관내 유두상 종양에서 더욱 빈번하게 관찰되므로 장 기간의 만성 염증이 담관내 유두상 종양의 발생과 연관될 수 있다고 하였다. 또한 Yeh 등(17)은 담관내 유두상 점액 종양의 64∼100%에서 간내담석증이 동반되었다고 하였고, Zen 등(13)은 간내담석증 환자의 면역조직화학 검사에서 간내담석증의 23%에서 담관내 유두상 종양이 관찰되었다 고 하였다.
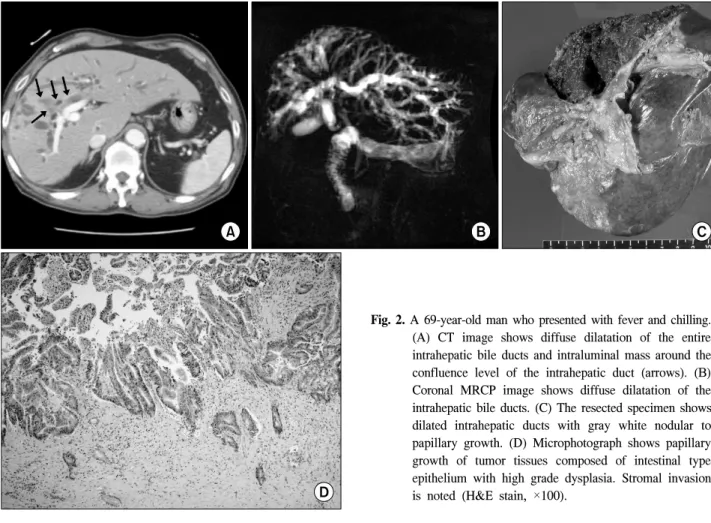
Fig. 2. A 69-year-old man who presented with fever and chilling.
(A) CT image shows diffuse dilatation of the entire intrahepatic bile ducts and intraluminal mass around the confluence level of the intrahepatic duct (arrows). (B) Coronal MRCP image shows diffuse dilatation of the intrahepatic bile ducts. (C) The resected specimen shows dilated intrahepatic ducts with gray white nodular to papillary growth. (D) Microphotograph shows papillary growth of tumor tissues composed of intestinal type epithelium with high grade dysplasia. Stromal invasion is noted (H&E stain, ×100).
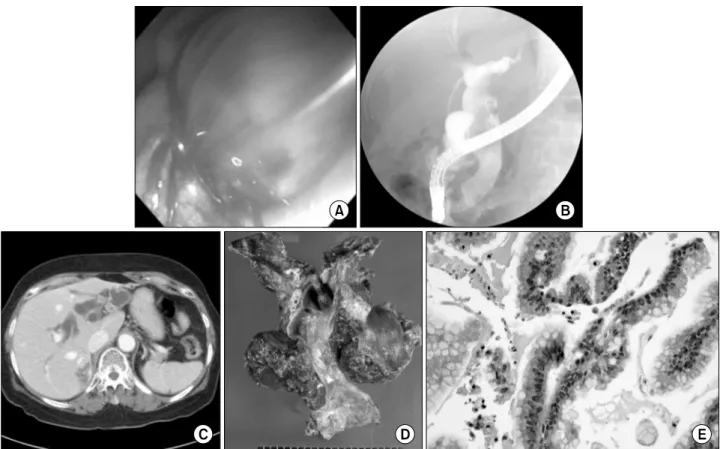
Fig. 3. A 62-year-old woman who presented with pain in the right upper abdominal quadrant, fever and jaundice 5 years after undergoing cholecystectomy for cholelithiasis. (A) Endoscopic image shows a large amount of mucin from the papilla. (B) ERCP image shows severe dilatation of the extrahepatic bile ducts and amorphous filling defects. (C) CT image shows dilatation of the left intrahepatic bile ducts. (D) The resected specimen shows markedly dilated lumen without definite mass. (E) Microphotograph shows mucin-containing gastric type epithelium with low grade dyplasia (H&E stain, ×200).
영상학적 검사에서 담관내 유두상 점액 종양은 확장된 담관안에서 편평하거나 결절 또는 폴립 등의 여러가지 형 태의 종괴로 관찰될 수 있으나 종양의 크기가 비교적 작거 나 무경형(sessile)이거나 점막표면을 따라 분포하는 경우에 는 어떤 영상검사로도 종양을 관찰하기가 어렵거나 불가능 할 수 있다.(18-20) 종양의 위치 확인은 수술적 치료에 있어 필수적이므로 확장된 담관의 철저한 검사는 꼭 필요하다.
따라서 의심되는 종양이 영상 검사에서 관찰되지 않을 때 에는 담도경 검사가 시행될 수 있다.(4,5) 만약 영상학적 검 사나 담도경으로도 종양을 관찰할 수 없을 경우에는 확장 된 담관을 포함하는 간 분절이나 구역을 절제해야 할 것이 다.(8) 점액은 초음파에서는 담즙처럼 일반적으로 무에코이 고, 컴퓨터단층촬영이나 자기공명영상에서도 물과 동일하 게 보이므로, 이런 영상검사에서 점액의 존재를 발견하는 것은 어렵다.(8,19,21) 그러나 내시경적 역행성 췌담관조영 술이나 경피경간담관조영술에서 점액은 확장된 담관 안의 다수의 길다란 선형이나 난원형, 또는 무정형의 음영결손 으로 관찰될 수 있다.(5,19,21) 또한 내시경 검사에서 십이지 장 유두로부터 점액이 배출되는 것이 관찰된다면 담관이나
췌장에서 점액을 생성하는 종양의 진단적 소견이라고 할 수 있다.(5,8,9) 초음파나 컴퓨터단층촬영 또는 자기공명영 상에서 간내담관뿐만 아니라 간외담관까지도 매우 확장된 소견을 관찰할 수가 있는데, 이것은 종양 자체 혹은 탈락된 종양파편이나 끈끈한 점액이 담즙의 흐름을 방해하고, 다 량으로 분비된 점액이 십이지장 유두에서 차단되므로 종양 의 원위부와 근위부가 모두 늘어나기 때문이다.(8,9,19,21) 담관은 미만성으로 대칭적으로 늘어날 수도 있지만, 병변 이 있는 간구역에서 비대칭적으로 심하게 확장되는 국소적 인 낭성변화, 즉 동맥류처럼 늘어날 수도 있다.(19-21) 종양의 성장이 느리고 림프절 전이가 상대적으로 드물지 만 점액 등으로 인한 급성 증상은 조기에 나타나고 재발하 는 경향을 보이므로 다른 담관암에 비해 절제율이 높고 수 술 후 장기 생존율을 기대할 수 있다.(5,17) 따라서 적극적 인 수술적 치료가 요구된다고 하겠다. Kim 등(5)은 85%의 근치적 절제율과 8∼42개월의 추적관찰기간 동안 87%의 생존율을 보고하였다. Yeh 등(17)은 1형과 2형은 100%의 생 존율을 보였고, 3형과 4형은 1년, 3년, 5년 생존율이 각각 100%, 33%, 17%와 56%, 32%, 14%였으며, 1형, 2형, 3형에
박선진 외:담관내 유두상 점액 종양 271
서는 림프절 전이가 없었고 림프절 전이가 있었던 4형은 전이의 유무에 따라 각각 12.1±5.1개월과 39.0±6.7개월의 생 존율을 보고하였다.
요약하면 담관내 유두상 점액 종양은 담관 상피에서 관 내 성장을 하는 유두상 종양으로 다량의 점액을 분비하고 간내담석증 등의 간의 만성염증성질환과 동반되는 경우가 흔하다. 이형성에서 침윤암까지 다양한 조직학적 소견을 보일 수 있지만, 일반적으로 점막에 국한되고 후기에 이르 러서 담관벽을 침윤하는 경도의 악성도를 보이는 종양이 다. 조기 진단과 다른 질환과의 감별진단이 중요하며, 수술 적 절제로 장기 생존율을 기대할 수 있겠다.
REFERENCES
1) Chen MF, Jan YY, Chen TC. Clinical studies of mucin- producing cholangiocellular carcinoma: a study of 22 histo- pathology-proven cases. Ann Surg 1998;227:63-9.
2) Shibahara H, Tamada S, Goto M, Oda K, Nagino M, Nagasaka T, et al. Pathologic features of mucin-producing bile duct tumors: two histopathologic categories as counterparts of pancreatic intraductal papillary-mucinous neoplasms. Am J Surg Pathol 2004;28:327-38.
3) Suh KS, Roh HR, Koh YT, Lee KU, Park YH, Kim SW.
Clinicopathologic features of the intraductal growth type of peripheral cholangiocarcinoma. Hepatology 2000;31:12-7.
4) Kim YS, Myung SJ, Kim SY, Kim HJ, Kim JS, Park ET, et al. Biliary papillomatosis: clinical, cholangiographic and cho- langioscopic findings. Endoscopy 1998;30:763-7.
5) Kim HJ, Kim MH, Lee SK, Yoo KS, Park ET, Lim BC, et al. Mucin-hypersecreting bile duct tumor characterized by a striking homology with an intraductal papillary mucinous tumor (IPMT) of the pancreas. Endoscopy 2000;32:389-93.
6) Chen TC, Nakanuma Y, Zen Y, Chen MF, Jan YY, Yeh TS, et al. Intraductal papillary neoplasia of the liver associated with hepatolithiasis. Hepatology 2001;34:651-8.
7) Nakanuma Y, Sasaki M, Ishikawa A, Tsui W, Chen TC, Huang SF. Biliary papillary neoplasm of the liver. Histol Histopathol 2002;17:851-61.
8) Lim JH, Yoon KH, Kim SH, Kim HY, Lim HK, Song SY, et al. Intraductal papillary mucinous tumor of the bile ducts.
Radiographics 2004;24:53-66; discussion 7.
9) Lim JH, Yi CA, Lim HK, Lee WJ, Lee SJ, Kim SH. Radio- logical spectrum of intraductal papillary tumors of the bile ducts. Korean J Radiol 2002;3:57-63.
10) Chow LT, Ahuja AT, Kwong KH, Fung KS, Lai CK, Lau JW.
Mucinous cholangiocarcinoma: an unusual complication of hepatolithiasis and recurrent pyogenic cholangitis. Histopathology 1997;30:491-4.
11) Zen Y, Fujii T, Itatsu K, Nakamura K, Minato H, Kasashima S, et al. Biliary papillary tumors share pathological features with intraductal papillary mucinous neoplasm of the pancreas.
Hepatology 2006;44:1333-43.
12) Sadler TW. Langman's Medical Embriology. Baltimore:
Williams & Wilkins; 1985.
13) Zen Y, Sasaki M, Fujii T, Chen TC, Chen MF, Yeh TS, et al. Different expression patterns of mucin core proteins and cytokeratins during intrahepatic cholangiocarcinogenesis from biliary intraepithelial neoplasia and intraductal papillary neoplasm of the bile duct--an immunohistochemical study of 110 cases of hepatolithiasis. J Hepatol 2006;44:350-8.
14) Joo YH, Kim MH, Lee SK, Seo DW, Yoo KS, Min YI, et al. A case of mucin-hypersecreting intrahepatic bile duct tumor associated with pancreatic intraductal papillary mucinous tumor. Gastrointest Endosc 2000;52:409-12.
15) Ishida M, Seki K, Honda K, Kimura T, Katayama K, Hirose K, et al. Intraductal mucinous tumors occurring simultaneously in the liver and pancreas. J Gastroenterol 2002;37:1073-8.
16) Hruban RH, Takaori K, Klimstra DS, Adsay NV, Albores- Saavedra J, Biankin AV, et al. An illustrated consensus on the classification of pancreatic intraepithelial neoplasia and intraductal papillary mucinous neoplasms. Am J Surg Pathol 2004;28:977-87.
17) Yeh TS, Tseng JH, Chiu CT, Liu NJ, Chen TC, Jan YY, et al. Cholangiographic spectrum of intraductal papillary mucinous neoplasm of the bile ducts. Ann Surg 2006;244:248-53.
18) Kokubo T, Itai Y, Ohtomo K, Itoh K, Kawauchi N, Minami M. Mucin-hypersecreting intrahepatic biliary neoplasms.
Radiology 1988;168:609-14.
19) Lee JW, Han JK, Kim TK, Kim YH, Choi BI, Han MC, et al. CT features of intraductal intrahepatic cholangiocarcinoma.
AJR Am J Roentgenol 2000;175:721-5.
20) Lim JH, Kim YI, Park CK. Intraductal mucosal-spreading mucin-producing peripheral cholangiocarcinoma of the liver.
Abdom Imaging 2000;25:89-92.
21) Yoon KH, Ha HK, Kim CG, Roh BS, Yun KJ, Chae KM, et al. Malignant papillary neoplasms of the intrahepatic bile ducts: CT and histopathologic features. AJR Am J Roentgenol 2000;175:1135-9.