288
서 론
췌관내 유두상 점액종양(intraductal papillary mucinous tumor, IPMT)은 1982년 Ohhashi 등(1)이 점액으로 가득찬 주 췌관의 확장과 점액의 과분비로 인한 십이지장 팽대부의 확장을 특징으로 하는 질환을 점액 분비 췌종양(mucus- secreting pancreatic cancer)으로 처음 보고한 이래로, 1996년 WHO의 정의에 의해 IPMT로 표기되기까지 점액 과분비 종 양(mucus-hypersecreting tumor), 점액 생성 종양(mucin-pro- ducing tumor), 점액성 췌관 확장증(micinous ductal ectasia), 췌관내 유두상 종양(intraductal papillary neoplasm)등 다양한 이름으로 불리워 왔다.(2) 비록 췌관 내에서 진행하고 침윤 경향이 적어 예후가 좋은 췌장 종양으로 알려져 있으나, adenoma부터 invasive carcinoma까지 다양한 spectrum의 종 양을 포함하고 있고, 전이 및 재발의 예가 비교적 많이 보고 되고 있으므로 진단 및 치료에 있어 많은 논란이 있는 실정 이다. 특히 병변의 위치에 따라 분지췌관형 병변의 경우 주 췌관형 병변에 비해 덜 침습적이고 예후가 좋은 것으로 보 고되고 있어,(3-6) 경우에 따라서 3 cm 이하의 분지췌관형 병변의 경우 외과적 절제 없이 지속적인 관찰 또는 축소수 술의 정당성에 대해 주장하기도 한다.(6) 따라서 본 논문은 분지췌관형 IPMT의 임상적 특징과 수술적 치료결과를 알 아보고 이를 토대로 적절한 치료방침을 제시하고자 본 연 구를 시행하였다.
분지 췌관형 췌관내 유두상 점액종양의 외과적 치료
성균관대학교 의과대학 삼성서울병원 외과 정준철․조성호․최성호․최동욱․김용일
(J Korean Surg Soc 2006;70:288-293)
Key Words: Pancreas, Intaductal papillary mucinous tumor (IPMT), Branch duct type, Recurrence 중심 단어: 췌장, 췌관내 유두상 점액종양, 분지췌관
현, 재발
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Department of Surgery, Samsung Medical Center, Sung- kyunkwan University School of Medicine, Seoul, Korea
Surgical Management for Intraductal Papillary Mucinous Tumor (IPMT) of the Pancreas Con- fined to Branch Duct
Jun Chul Chung, M.D., Sung Ho Jo, M.D., Seong Ho Choi, M.D., Dong Wook Choi, M.D. and Yong Il Kim, M.D.
Purpose: Intraductal papillary mucinous tumor (IPMT) of the branch duct type has been reported that it is associated with less aggressive histologic features than the main duct type.
The purpose of this study was to evaluate the clinico- pathologic features and the optimal management of branch duct type IPMT.
Methods: From October 1994 to November 2004, 30 cases who underwent operations with branch duct type IPMT were reviewed retrospectively. Clinicopathologic findings and late results of treatment were studied in 20 cases of the benign (adenoma, borderline malignancy) group and in 10 cases of the malignant (carcinoma in situ, invasive carcinoma) group.
Results: There were statistically significant difference in the 3 factors (mural nodule (P=0.030), diameter of the main pancreatic duct (P=0.036), main location of the tumor (P=
0.031)). There was no statistically significant difference in th survival analysis between the main duct type IPMT including combined type IPMT and the branch duct type IPMT (P=0.572), but there was significant difference between the benign group and the malignant group of the branch duct type IPMT (P=0.049).
Conclusion: The long-term follow up result of the branch duct type IPMT is similar to that of the main and combined duct type IPMT. Therefore, it is not safe just to monitor the branch duct type IPMT. Our results suggest that surgery is certainly the gold standard treatment for the branch duct type IPMT. And after operation, close long term follow up with appropriate treatment is necessary due to tumor recurrence.
책임저자:최성호, 서울특별시 강남구 일원동 50번지
ꂕ 135-710, 성균관대학교 의과대학 삼성서울병원 외과 Tel: 02-3410-3469, Fax: 02-3410-0040
E-mail: [email protected]
접수일:2005년 8월 29일, 게재승인일:2005년 12월 5일
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
방 법
1994년 10월부터 2004년 12월까지 삼성서울병원에서 IPMT로 수술을 시행받은 59명의 환자 중 분지췌관형 병변 으로 확진된 30예를 대상으로 후향적 분석을 시행하였다.
병변의 아형은 Kuroda(7) 분류에 따라 주췌관형(main duct type), 분지췌관형(branch duct type) 및 혼합형(combined type)으로 나누었고, 병리학적 소견은 WHO classification에 따라 adenoma, borderline malignancy, carcinoma in situ, in- vasive carcinoma 등 4 type으로 분류하였다. 우선 분지췌관 형 병변의 임상 및 병리학적 특징과 재발 및 생존율을 알아 보기 위해 주췌관형과 혼합형 병변을 한 군으로 묶어 두 군간의 차이를 분석하였고, 이 중 분지췌관형 병변에 대하 여 adenoma와 borderline malignancy를 양성군으로, carci- noma in situ와 invasive carcinoma를 악성군으로 묶어 양성 및 악성에 따른 임상 및 병리학적 특징과 생존율을 비교분 석하였다. 통계 분석은 SPSS 11.5 for Windows를 이용하여 t-test, chi-square test로 검정하였고, 생존분석에는 Kaplan- Meier method 및 log-rank test를 사용하여 P-value가 0.05 이 하인 경우를 통계학적으로 유의하다고 판정하였다.
결 과
1) IPMT의 아형에 따른 임상양상 및 병리학적 특성 분 석
주췌관형과 혼합형 병변을 한 군으로 묶어 분지췌관형 병변과의 임상 및 병리학적 특징을 비교한 결과, 당뇨를 동 반한 경우(P=0.037), 십이지장 팽대부의 확장소견이 보이는 경우(P=0.003), mucin을 분비하는 경우(P=0.013), 주췌관의 확장이 있는 경우(P<0.001)에 주췌관형과 혼합형인 경우가 많았으나, 나이, 성별, 임상증상, 종양 표식자인 CA19-9과 CEA, 알코올 섭취유무, 흡연유무, 종양의 위치 및 크기, 병 리소견에 따른 두 군간의 차이는 없었다(Table 1).
2) 분지췌관병변의 양, 악성에 따른 임상양상 및 병리 학적 특성 분석
분지췌관형 병변은 총 30예로 adenoma 8예(26.7%), bor- derline malignancy 12예(40.0%), carcinoma in situ 6예(20.0%), invasive carcinoma 4예(13.3%)였다. Adenoma와 borderline ma- lignancy를 양성군으로, carcinoma in situ와 invasive carci- noma를 악성군으로 묶어 임상 및 병리학적 특징을 비교한 결과, mural nodule을 동반하는 경우(P=0.030), 주췌관의 확 장이 있는 경우(P=0.036), 종양이 췌두부에 위치하는 경우 (P=0.031)에 악성인 경우가 많았으나, 환자의 나이, 성별, 임 상증상, 종양 표식자인 CA19-9과 CEA, 알코올 섭취유무, 흡연유무, 당뇨 유무, 십이지장 팽대부의 확장유무, mucin
분비유무, 종양의 크기는 두 군 간에 차이가 없는 것으로 나타났다(Table 2).
3) 외과적 치료
모든 분지췌관형 병변에 대하여 수술을 시행하였다. 수 술은 병변의 위치에 따라 췌두부십이지장절제술 7예, 유문 보존 췌두부십이지장절제술 12예, 원위부 췌장절제술 5예 를 시행하였고, 종양의 크기가 14 cm였던 1예와 주췌관이 8 mm 이상으로 전반적으로 늘어나 있었던 4예, 췌장에 염 증이 심하여 주변조직과 유착이 심했던 1예에서 췌전절제 술이 시행되었다(Table 3).
4) 수술 후 재발
IPMT로 수술을 받은 모든 환자는 복부 전산화단층촬영을 통하여 정기적으로 외래 추적 관찰을 시행하였고, 5예에서
Table 1. Clinicopathologic features of intaductal papillary muci- nous tumor (IPMT)
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ Main duct and Branch duct
P-value combined type (n=29) type (n=30) ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Male:female 20:9 20:10 0.850
Age (mean±SD*) 60.7±10.6 57.0±8.6 0.065
Chief complaint 0.919
Adominal pain 16 (55.2%) 11 (36.7%) Jaundice 2 (6.9%) 1 (3.3%) Body weight loss 1 (3.4%) 1 (3.3%) Serum tumor marker
(mean±SD)
CA19-9 (U/ml) 100.4±199.1 43.1±91.3 0.174
CEA (ng/ml) 2.8±2.1 1.8±0.9 0.191
Diabetics (%) 57.1 30 0.037
Current drinker (%) 44.4 41.4 0.817
Current smoker (%) 40.7 41.4 0.961
Patulous papilla (%) 75.0 34.6 0.003
Mucin excretion (%) 60.7 26.9 0.013
Diameter of the
12.5±4.9 5.1±2.5 <0.001 MPD† (mm)±SD
Tumor size (cm)±SD 4.9±3.5 3.5±3.0 0.090
Main location of the tumor 0.001
Head 17 (58.6%) 11 (36.7%)
Uncinate process 1 (3.5%) 13 (43.3%) Body or tail 11 (37.9%) 6 (20.0%)
Pathology 0.367
Adenoma 4 (13.8%) 8 (26.7%) Borderline malignancy 9 (31.0%) 12 (40.0%) Carcinoma in situ 9 (31.0%) 6 (20.0%) Invasive carcinoma 7 (24.2%) 4 (13.3%) ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
* = standard deviation; † = main pancreatic duct.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
재발을 확인할 수 있었다. 병변은 주췌관형이 3예, 분지췌 관형이 2예로 조직 소견상 모두 carcinoma in situ였고, 재발 부위로는 간의 다발성 전이 1예, 췌장국소재발 2예, 주위 림 프절 전이 및 복막파종이 2예에서 나타났다. 췌장국소재발 환자들에게 항암치료 및 방사선치료를 시행하였으나 대증 적 요법을 시행한 나머지 재발환자와 더불어 추적기간 중 모두 사망하였다(Table 4).
5) 생존 분석
대상 환자 전체의 평균 추적 관찰 기간은 23.7개월(2∼80 개월)로 사망한 환자는 모두 10예에서 있었다. 이 중 IPMT 와 관계없이 사망한 환자가 5예에서 있었는데 이들은 패혈 증, 흉부 대동맥류 파열, 진행성 위암, 교액성 장폐색, 대장 암의 간전이로 인해 각각 1, 2, 6, 19, 25개월에 사망하였다.
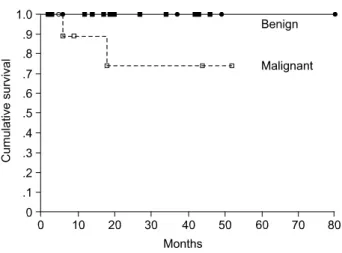
Kaplan-Meier 방법을 이용하여 생존분석을 시행한 결과 주 췌관형 및 혼합형 병변인 경우와 분지췌관형 병변인 경우 5년 생존율은 각각 79.5%, 90.8%로 분지췌관형 병변에서 다
소 높게 나타났으나 통계학적으로 두 군 간의 차이는 없었 고(P=0.537)(Fig. 1), 분지췌관형 병변 중 양성 및 악성에 따 른 5년 생존율은 각각 100.0%, 74.1%로 양성인 경우 생존율 이 유의하게 높았다(P=0.049)(Fig. 2).
고 찰
췌관내 유두상 점액종양은 1982년 Ohhashi 등(1)이 점액 으로 가득 찬 주췌관의 확장, 주췌관과 연결된 낭성병변, 점 액에 의해 열린 십이지장 팽대부 및 폐쇄성 췌장염을 시사 하는 증상 등 4가지 조건을 제시하며 처음 기술하였고, 전 산화 단층촬영과 내시경적 역행성 담췌관 조영술 등 영상 의학적 진단의 도움에 의해 점차 이 질환의 보고가 증가되 고 있다.
점액 과분비 종양(mucus-hypersecreting tumor), 점액 생성 종양(mucin-producing tumor), 점액성 췌관 확장증(micinous ductal ectasia), 췌관내 유두상 종양(intraductal papillary neoplasm) 등 다양한 이름으로 불리워 온 이 종양은 최근 췌장 낭성병변에 대한 많은 연구가 진행됨에 따라 일반적 인 췌장암 또는 췌장 낭성 종양과 달리 특징적인 임상양상 을 나타내는 주췌관 병변임이 밝혀지게 되었고,(2) 1996년 WHO에 의해 IPMT로 분류 정의되었다.
이 종양의 흥미로운 점은 비교적 느린 성장과 드문 전이 로 인해 췌장암에 비해 예후가 좋은 것으로 보고되고 있는 Table 2. Clinicopathologic features of branch duct type intaductal
papillary mucinous tumor (IPMT)
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
Benign Malignant
P-value
(n=20) (n=10)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Male:female 15:5 5:5 0.171
Age (mean±SD*) 57.8±7.5 55.6±10.6 0.480
Chief complaint 0.077
Adominal pain 9 (45.0%) 2 (20.0%) Jaundice 0 (0.0%) 1 (10.0%) Body weight loss 0 (0.0%) 1 (10.0%) Serum tumor marker
(mean±SD)
CA19-9 (U/ml) 33.0±71.2 64.3±126.4 0.572
CEA (ng/ml) 1.7±0.9 2.0±0.8 0.482
Diabetics (%) 35.0 20.0 0.398
Current drinker (%) 47.4 30.0 0.367
Current smoker (%) 47.4 30.0 0.367
Mural nodule (%) 0.0 30.0 0.030
Patulous papilla (%) 38.9 25.0 0.492
Mucin excretion (%) 27.8 25.0 0.883
Diameter of the
3.7±1.8 5.8±2.6 0.036
MPD†(mm)±SD
Tumor size (cm)±SD 3.2±2.8 4.1±3.4 0.270
Main location of
0.031 the tumor
Head 5 (25.0%) 6 (60.0%) Uncinate process 13 (65.0%) 1 (10.0%) Body or tail 2 (10.0%) 3 (30.0%)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
* = standard deviation; † = main pancreatic duct.
Table. 3 Types of operation for intaductal papillary mucinous tumor (IPMT)
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ Main duct type/ Branch duct Types of operation
combined type type ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Whipple's procedure 5 7
PPPD* 3 12
Distal pancreatectomy 10 5
Total pancreatectomy 11 6
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
* = pylorus-preserving pancreaticoduodenectomy.
Table 4. Charateristics of the cases with tumor recurrence ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
Survival/
Sex/age Duct type Pathology Site
duration (mo) ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
M/57 Main CIS* Pancreas Dead/13
M/32 Main CIS Intra-abdominal LN Dead/14
M/66 Main CIS Pancreas Dead/31
F/58 Branch CIS Intra-abdominal LN Dead/6
F/74 Branch CIS Liver Dead/18
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
* = carcinoma in situ.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
점과,(8) 병리학적 특성상 adenoma에서 invasive carcinoma로 발전하는 adenoma-carcinoma sequence를 뒷받침하는 종양으 로 생각되어지기 때문이다.(9)
이 종양은 중년 여성 및 체부 또는 미부에 호발하는 점액 성 낭성 종양과는 달리 고령 남성 및 췌두부에 호발하는 주췌관 병변으로(10) 복통 및 췌장염증상부터 당뇨, 체중감 소 등 다양한 증상을 보일 수 있으나, 종양 표지자와 병변과 의 연관성은 없는 것으로 알려져 있다. 본 연구에서도 종양 의 위치는 두부와 구상돌기에 많았고 남자에서 호발하였으 나 종양표지자와 병변과의 연관성은 없는 것으로 나타났 다. 췌장염증상은 대부분 만성췌장염 소견을 보이는데, 이 는 췌관의 점액으로 인해 췌관압이 상승함에 따라 나타나 는 것으로 여겨지고 있고,(15,16) 당뇨 또한 종양의 성장과 점액의 저류에 의해 췌관이 막히면서 발생하는 것으로 알 려져 있으며,(16,17) 황달의 경우 5∼25%에서 보이는데 점 액의 저류에 의해 총담관이 막히거나, 일부는 종양이 직접 총담관을 침범하여 발생한다고 생각되어지고 있다.(15,17) 방사선적으론 전산화 단층 촬영과 내시경적 역행성 담췌 관 조영술을 통해 진단 및 병변의 위치와 모양을 파악하는 데 큰 도움을 받을 수 있고, 특히 내시경적 역행성 담췌관 조영술을 통해 확장된 십이지장 팽대부와 점액분비, 확장 된 주췌관 및 분지췌관, 병변 내 점액이나 고형결절에 의한 충만 결손 등을 확인할 수 있다. 전산화 단층 촬영을 통하여 늘어난 주췌관 또는 분지췌관 및 때때로 고형 결절을 볼 수 있고, Barbe 등은 CT, ERCP, EUS의 정확도를 각각 72%, 83%, 94%로 보고하였다.(18) 최근 MRCP의 사용이 늘고 있 는 바 Sugiyama 등(19)은 MRCP가 병변의 위치파악과 ERCP 의 역할을 대신할 수 있는 장점이 있으나, 낭성병변과 췌관 과의 연결을 확인할 수 없고, 유두부에서의 점액배출 확인
이 어렵다는 한계를 보고하기도 하였다. 그 외에도 경구 경 팽대부 췌관경(peroral transpapillary pancreatoscopy), 내시경 적 췌조직 검사와 췌액 세포검사(endoscopic pancreatic biopsy with pancreatic juice cytology), 수술 중 초음파(IOUS) 가 도움이 될 수 있다.(20)
육안적 소견으로 Tagaki 등(21)은 주췌관의 확장과 종양 이 주췌관 안에만 있는 주췌관형과 종양이 췌관의 가지에 있는 분지췌관형의 2가지로 분류하였고, Furukawa 등(11)은 주췌관이 전반적으로 확장된 형태, 주췌관이 국소적으로 확장된 형태, 분지췌관이 낭성변화된 형태, 분지췌관이 확 장된 형태의 4가지 형으로 분류하였다. Kuroda(7)는 종양이 주췌관에 위치하고 주췌관의 확장을 동반한 주췌관형(main duct type)과, 종양이 분지췌관에 위치하고 분지췌관만 확장 된 소견을 보이는 분지췌관형(branch duct type) 및 두 가지 형태가 복합적으로 존재하는 혼합형(combined type)의 세 가 지 형태로 분류하였다.
Shimamura 등(12)은 낭성병변의 크기와 주췌관 확장 정 도의 기준을 3.0 cm, 1.0 cm로 하여 그 이하이면 양성병변이 라 하였고, 특히 3.0 cm 이하의 분지췌관 병변은 예후가 아 주 좋다고 보고하였다.
한편 IPMT의 발생장소에 따른 악성도를 예측하려는 연 구가 진행되었는데 기존의 보고들에 의하면 분지췌관형 병 변인 경우 악성인 경우가 드물고 예후가 좋은 것으로 나타 났다.(3-6) 특히 Terris 등(3)은 13예의 분지췌관형 병변 중 2예에서 carcinoma in situ이고 나머지는 양성병변이었다고 발표하였고, Kobori 등(6)은 16예의 분지췌관형 병변에서 1 예만 췌장실질 침범이 있고, 4예는 악성병변이지만 췌장 실 질 침범이 없는 상태이므로 분지췌관형 병변에서 축소수술 의 정당성에 대해 주장하였다. 그러나 본 연구에서는 30예 Fig. 1. Survival curve according to the ductal type of intaductal
papillary mucinous tumor (IPMT). The branch duct type IPMT tended to have better survival than the main duct type IPMT and combined type IPMT, but this was not statistically significant (P=0.537).
Fig. 2. Survival curve according to the histologic type of branch duct type IPMT. The benign branch duct type IPMT tended to have better survival than the malignant branch duct type IPMT (P=0.049).
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 의 분지췌관형 병변 중 6예에서 carcinoma in situ, 4예에서
invasive carcinoma 소견을 보였고, 이는 주췌관형 및 혼합형 병변에 비해 큰 차이를 보이지 않았다. 또한 재발 및 예후에 있어서도 분지췌관형 병변의 우월성을 입증할 수 없었다.
조직학적 소견으로 상피세포의 이형성에 따라 adenoma, borderline malignancy, carcinima in situ, invasive carcinoma 등 4가지 형으로 나누어 볼 수 있으나,(13) 한 종양에서도 부위 에 따라 각기 다른 정도의 이형성을 볼 수 있고, 다발성일 수 있기 때문에 광범위한 검색 후 진단을 내리는 것이 중요 하다.
췌관내 유두상 점액종양은 비교적 예후가 좋은 종양으로 알려져 왔으나 침윤성 및 재발성 병변에 대한 보고가 많아 짐에 따라 적극적으로 절제하는 추세이다.(14) 경계성 악성 또는 악성병변이 의심되는 경우에는 보다 적극적인 절제가 필요하며 침윤성 병변의 경우 절단면의 암 침윤 가능성을 생각하여 광범위한 췌장 절제를 시행하여야 한다.
수술 후 5년 생존율은 82.6%로 일반적인 췌관에 생긴 암 의 17.3%에 비해 예후가 좋으나, 주변조직으로 침범이 있는 경우와 없는 경우 5년 생존율이 각각 28%, 86%로 주위 조 직 침범 및 전이 여부가 예후에 매우 중요하다.(15) 본 연구 에서도 분지췌관 병변의 경우 5년 생존율은 90.8%, 주췌관 및 혼합형 병변의 경우 79.5%로 일반적인 췌장암에 비해 예후가 좋은 것으로 나타났다.
향후 추적 검사로는 간, 폐로의 전이와 절단면 주변부의 재발보고가 있으므로 암태아성 항원, 흉부방사선검사, 초음 파검사 또는 전산화 단층 촬영을 포함하는 정기적인 외래 추적검사가 필요할 것으로 생각된다.
결 론
1994년 10월부터 2004년 12월까지 삼성서울병원에서 IPMT로 수술을 시행받은 59명의 환자 중 분지췌관형 병변 30예를 대상으로 adenoma와 borderline malignancy를 양성군 으로, carcinoma in situ와 invasive carcinoma를 악성군으로 묶어 비교한 결과, mural nodule을 동반하는 경우(P=0.030), 주췌관의 확장이 있는 경우(P=0.036), 종양이 췌두부에 위 치하는 경우(P=0.031)에 악성인 경우가 많았다. 일부 보고 에 의하면 3 cm 이하의 분지췌관형 병변의 경우 외과적 절 제 없이 지속적인 관찰 또는 축소수술을 제안하기도 하지 만 본 연구에서는 악성 분지췌관형 병변 10예 중 8예에서 3cm 이하의 병변이었고, 또한 재발 및 예후에 있어 주췌관 형 및 혼합형 병변과의 차이를 발견할 수 없었다. 따라서 본 저자들은 수술 전 IPMT의 아형에 따른 악성화 여부를 속단하는 것은 위험하며, 분지췌관형 IPMT의 치료에 있어 외과적 절제술이 필요하다고 생각된다. 특히 3 cm 이하의 분지췌관형 병변인 경우라도 적극적인 수술적 치료와 더불 어 수술 후 정기적인 경과관찰이 필요할 것으로 생각한다.
REFERENCES
1) Ohhashi K, Murakami Y, Maruyama M, Takekoshi T, OhtaH, Ohhashi H, et al. Four cases of “mucin-producing” cancer of the pancreatic on specific findings of the papillar Vater. Prog Dia Endosc 1982;20:348-51.
2) Chang WY, Heo JS, Noh JH, Sohn TS, Choi SH, Kim YI.
Surgical treatment for intraductal papillary mucinous tumor of the pancreas. J Korean Surg Soc 2002;62:491-5.
3) Terris B, Ponsot P, Paye F, Hammel P, Sauvanet A, Molas G, et al. Intraductal papillary mucinous tumors of the pancreas confined to secondary ducts show less aggressive pathologic features as compared with those involving the main pancreatic duct. Am J Surg Pathol 2000;24:1372-7.
4) Sugiyama M, Atomi Y. Intraductal papillary mucinous tumors of the pancreas: imaging studies and treatment strategies. Ann Surg 1998;228:685-91.
5) Tanaka M. Intraductal papillary mucinous neoplasm of the pancreas: diagnosis and treatment. Pancreas 2004;28:282-8.
6) Kobori M, Egawa SI, Shibuya K, Shimamura H. Intraductal papillary mucinous tumor of the pancreas comprise 2 clinical subtypes. Arch Surg 1999;134:1131-6.
7) Kuroda A. Recent progress in clinicopathology of pancreatic tumors. Tan To Sui 1988;9:1459-72 (in Japan).
8) McDonald JM, Williard W, Mais D, Beitler A. The incidence of intraductal papillary mucinous tumors of the pancreas. Curr Surg 2000;57:610-4.
9) Yamada M, Kozuka S, Yamao K, Nakazawa S, Naitoh Y, Tsukamoto Y. Mucin-producing tumor of the pancreas. Cancer 1991;68:159-68.
10) Yanagisawa A, Ohhashi K, Hori M, Takagi K, Kitagawa T, Sugano H, et al. Ductectatic-type mucinous cystadenoma and cystadenocarcinoma of the human pancreas: a novel clinico- pathological entity. Jpn J Cancer Res 1993;84:474-9.
11) Furukawa T, Takahashi T, Kobari M, Matsuno S. The mucus- hypersecreting tumor of the pancreas. Developmental and ex- tension visualized by three-dimensional computerized mapping.
Cancer 1992;70:1505-13.
12) Shimamura H, Furukawa T, Kodama T, Matsumoto G, Kimura M, Yusa T, et al. Mucin-producing tumor of the pancreas- surgical treatment. J Hep Bil Pancr Surg 1997;4:168-76.
13) Nagai E, Ueki T, Chijiiwa K, Tanaka M, Tsuneyashi M. In- traductal papillary mucinous neoplasm of the pancreas associated with so-called “Mucinous ductal ectasia Histoche- mical” and immunohistochemical analysis of 29 cases. Am J Surg Pathol 1995;19:576-89.
14) Sho M, Nakajima Y, Kanehiro M, Hisanaga M, Nishio K, Nagao M, et al. Pattern of recurrence after resection for intraductal papillary mucinous tumors of the pancreas. World J Surg 1998;22:874-8.
15) Kimura W, Mahuuchi M, Kuroda A. Charateristics and trea-
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ tment of mucin-producing tumor of the pancreas. Hepato-
gastroenterology 1998;45:2001-8.
16) Jang JY, Kim SH, Ahn YJ, Yoon YS, Lee KU, Lee YJ, et al. Analysis of clinical features and factors predictive of malignancy in intraductal papillary mucinous tumor of the pancreas: multi-center analysis in korea Korean. J HBP Sur- gery 2003;7:1-11.
17) Kippel G. Clinicopathologic view of intraductal papillary mucinous tumor of the pancreas. Hepatogastroenterology 1998;45:1981-5.
18) Yun JS, Cho SI, Lee HS, Chung JP, Park YN, Kim KS, et al. Clinical & pathological characteristics of intraductal pa-
pillary mucinous tumor of the pancreas. J Korean Surg Soc 2003;64:165-9.
19) Sugiyama M, Atomi Y, Kuroda A. Two types of mucin- producing cystic tumors of the pancreas: diagnosis and treatment. Surgery 1997;122:617-25.
20) Roh HR, Kin SH, Suh KS, Park YH, Lee KU. Surgical management of intraductal papillary mucinous tumor of the pancreas. J Korean Surg Soc 1999;57:260-71.
21) Takagi K, Ohta H, Ohhashi K. Diagnostic ability and limitation of ERCP for pancreatic cancer. Stomach and Intestine 1982;17:1065-80 (in Japan).