Introduction
The introduction of osseointegrated dental implants in dentistry brought out a new era in dental clinical practice.
During the past 50 years, prosthetic rehabilitation of the edentulous patient with implant-supported prosthesis has developed into a viable and predictable treatment option [1,2].
As the practice of dental implant has been developed, the immediate and early loading of implants appears to be a viable treatment option in the fully edentulous ridges. Some reports
have shown successful clinical results [3-5]. Various designs of implant and prosthetic components were suggested by different manufacturers for immediate and early loading of implants.
Though histomorphometric studies in humans as well as in animals have assured the possibility by showing remarkable results, it could be hasty generalization to extrapolate these examples to other implant designs.
Materials and Methods
The subject was a 59-year-old patient with advanced periodontitis and partial edentulism who came in for restorative treatment. He was healthy and had no medical history with surgical contra-indications. Implant-fixed restorations were planned for both maxilla and mandible. The patient wanted to restore maxilla and mandible one after the other. First, 10
Determination of implant loading timing:
A pilot histomorphometric human study
Se Hoon Kahm*
Department of Dentistry, Jeju National University Hospital, Jeju, Korea
ABSTRACT
Purpose: The purpose of this study are to perform a histomorphometric analysis of the peri implant tissue reaction and the bone implant interface in early loaded implants and an unloaded implant in the edentulous maxilla, and to compare these results for determining proper timing of supra structure placement.
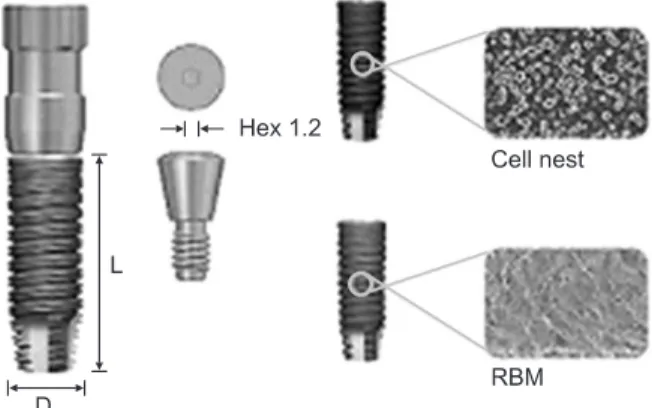
Materials and Methods: In this study, GS- II implant (Osstem Co., Korea) was used. GS II implant fixture is a dual threaded internal connection type with upper microthreads and Cell Nest surfaces (anodic oxidation treatment). Three early loaded implants groups (5 days, 20 days, 50 days after surgical treatments) and an unloaded implant control group in the edentulous maxilla were retrieved with a 5.0 mm trephine bur. Histomorphometric analysis – percentage of bone-to-implant surface contact (BIC) and bone volume – was perfomed through digital imaging analysis.
Results: The histologic data showed that the osseointegration was achieved in both loaded and unloaded conditions. Five days group showed slightly higher BIC and bone volume than other early loaded groups. Unloaded group was failed to compare.
Conclusion: Within the limitations of the study, the clinical and radiological results showed that the osseointegration was achieved. Immediate functional loading of implants could lead to favorable bone responses. More studies are needed so that proper and faster way of loading implants can be developed.
Key Words: Bone remodeling, Dental implants, Immediate dental implant loading, Oseeointegration
Received Feb 17, 2014; Revised version received Mar 5, 2014 Accepted Mar 6, 2014
Corresponding author: Se Hoon Kahm
Department of Dentistry, Jeju National University Hospital, 15 Aran 13-gil, Jeju 690-767, Korea
Tel: 82-64-717-1843, Fax: 82-64-717-1846 E-mail: [email protected]
implants were installed with 4 mini implants for study and the other 6 implants for further restorations in maxilla. #15, 16, 25, 26 implants were test implants-GS-II implant, D3.5×L8.5 mm (Osstem Co., Seoul, Korea) (Fig. 1). After installation, immediate impression was taken with custom tray and pick-up impression copings. #16 (5 days-immediate load group), #26 (20 days-early load 1 group), #25 (50 days-early load 2 group),
#15 (180 days-delayed load group) implant were connected for the interim restorations. Each implant was connected
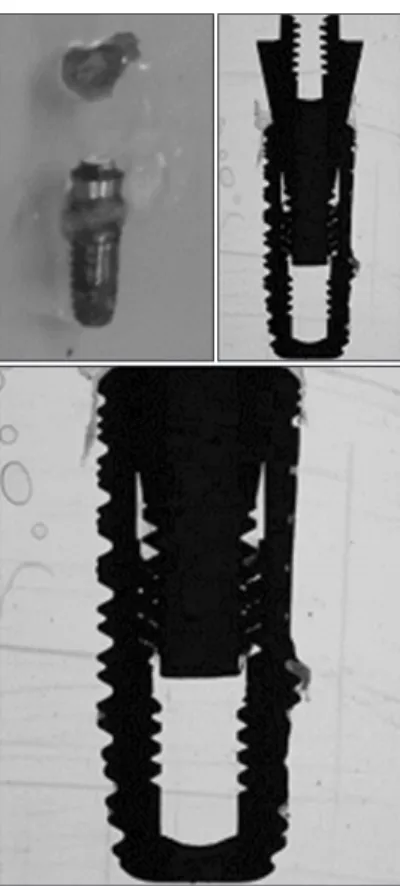
and loaded functionally. Eight months later, 4 implants with surrounding bone were retrieved with a 5.0 mm trephine bur. Histologic samples were prepared and examined by light microscope. Measured data were converted to digital images with Axiocam MRc5 (Carl Zeiss, Jena, Germany). The BIC (percentage of bone-to-implant surface contact, %), bone volume (proportion of mineralized bone within the limits of the three consecutive implant threads, %) of specimens were calculated with an image analysis software (Axiovision 4.1; Carl Zeiss). 4 additional implants (GS-II ultrawide, D6×L13 mm) were placed replacing test implants for definitive prosthesis (Figs. 2-5).
Results
All implants were successfully osseointegrated in clinical and radiological evaluation. There was a problem with retrieving procedure, #15 implant (180 days-delayed group) sample could not be measured in histomorphometrical study. Except for #15 implant (180 days-delayed group), at low magnification, it was possible to observe that bone trabecule was present around the implants. Areas of bone remodeling and haversian systems
Fig. 5. Panoramic view after retrieving test implants and installing wide implants.
Fig. 4. Panoramic view in loading status, at 50 days.
Fig. 3. Panoramic view with surgical stent.
Fig. 2. Initial panoramic view.
Fig. 1. GS-II implant fixture (Osstem Co., Seoul, Korea).
RBM: resorbable blasted media.
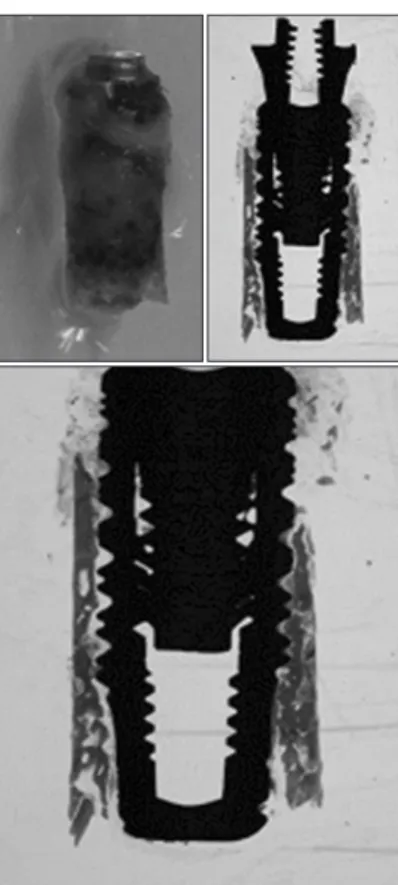
were present near the implant surface. In the area of implant’s top, the infiltration of inflammatory cells and retarded healing process were observed (Figs. 6-9). However, compact, cortical and mature bone with well-formed osteons was present at the interface of the measured implants. BICs of measured implants were 74.92%±18.05% in #16 implant (5 days-immediate load group), 55.90%±24.41% in #26 implant (20 days-early load 1 group), and 51.40%±32.71% in #25 implant (50 days-early load 2 group). Bone volumes of measured implants were 74.64±
23.08% in #16 implant (5 days-immediate load group), 43.49%
±37.54% in #26 implant (20 days-early load 1 group), and 60.91%±21.59% in #25 implant (50 days-early load 2 group) (Fig. 10, Table 1).
Discussion
Development of implant industry-enhancement of implant surface treatment, modification of implant design and surgical techniques-could lead to early or immediate implant loading for edentulous patients. Immediate loading protocol has
advantages and disadvantages. It can decrease total treatment time, dental visits, surgical interventions. Besides patients’
compliance and comfortable function, esthetics can be improved. On the other hand, it has some problems, such as higher failure rates, unpredictable soft tissue changes (Table 2).
There are several methods for implant stability and success, such as success rate, marginal loss measurement, presence or absence of peri-implantitis, periotest, and resonance frequency analysis (implant stability quotient values).
Also, histomorphometric analysis is a certain method for bone maturity and bone-implant contact. There are some histomorphometric reports about animals, human cadavers, patient’s request about immediate implant loading [6-10].
In animal studies, immediate loading does not affect the bone mineral apposition rate when compared with unloaded implants [6,7]. In human biopsy of immediate loaded implants, even in a poor bone site and after a healing period of only 2 months, there was a high bone-to-implant contact percentage [9]. This indicate that early and immediate loading of single- unit SLA surfaced implants was possible.
Fig. 6. Histomorphometric view of #15 implant (180 days-delayed load control group).
Fig. 7. Histomorphometric view of #16 implant (5 days-immediate load test group).
Comparison of immediate and delayed implants appeared radiographically osseointegrated and clinically stable at retrieval. Mineralized tissue was found at the implant interface.
The percentage of bone-to-implant contact in the delayed and immediate implants was 58%±4.0% and 52%±3.2%, respectively. In the loaded implant, a more compact, mature,
well-organized peri-implant bone was found with many areas of remodeling and some osteons, whereas the bone tissue surrounding the unloaded implant was constituted of only thin bone trabeculae. Immediate loading did not seem to impair osseointegration of an immediate postextraction implant compared to an unloaded post extraction one [10].
In this study, the histologic data showed that the osseointeg- Fig. 9. Histomorphometric view of #25 implant (50 days-early load 2 test group).
Fig. 8. Histomorphometric view of #26 implant (20 days-early load 1 test group).
Fig. 10. Bone-to-implant surface contact (BIC), bone area in diagram.
Table 1. BIC and Bone Area in Each Group
Group BIC (%) Bone area
(volume; %)
#16 (5 days)
Immediate load group
#26 (20 days) Early load 1 group
#25 (50 days) Early load 2 group
#15 (180 days) Delayed load group
74.92±18.05
55.90±24.41
51.40±32.71
Not measured
74.64±23.08
43.49±37.54
60.91±21.59
Not measured
Values are presented as mean±standard deviation.
BIC: bone-to-implant surface contact.
ration was achieved well in all conditions. The time of loading implants affected the oseeointegration in histomorphometrical analysis. Osseointegration is newly defined as, ‘stability of an implant in bones that represents a dynamic equilibrium between existing native bone (primary contact) and remodeling and new bone formation (secondary contact) and it’s maintenance at the bone-implant interface’. However, its relation is not linear, as a diagram. After 2-4 weeks implant was installed, BIC was very low, called ‘stability dip’ [11,12]. It was dangerous for functional loading in those periods. This study showed the similarity of loading timing of the implant. After that, the BIC of the implant was stabilized and trabecular bone maturation was more progressing. Then stability and loading capacity of implants were increased. In this study, GS-II implant (Osstem Co.) was used. GS-II implant fixture is a dual-threaded internal connection type with upper microthreads and Cell-Nest surfaces (anodic oxidation treatment). Tapered and dual threaded design of implant and surface modification-anodizing treatment-could be helpful in early implant to bone contact and newly bone formation.
Determining the loading timing of the implants was not a simple matter. However, the dangerous period of functional loading certainly exists. The restoration of implants should be avoided in these periods. Histomorphometric analysis of implant is invasive and dangerous method, but it could provide exact information about bone remodeling condition, bone to implant contact, newly formed bone information. Limited in this study, there are possibility of immediate loading could have positive effects in bone formation and remodeling. More prospective studies might show the proper timing of implant loading.
In this study, the clinical and radiological results showed that the osseointegration was achieved. The time of loading implants might affect the osseointegration in histological aspects.
Likely, immediate functional loading of implants could lead to favorable bone responses. However, in order to have a more proper and faster way of loading implants, more prospective studies and randomized controlled trials are needed.
Acknowledgments
Histomorphological analysis of this paper helped to appre- ciate Osstem Implant Research Center.
References
1. Brånemark PI, Adell R, Breine U, Hansson BO, Lindström J, Ohlsson A: Intra-osseous anchorage of dental prostheses. I.
Experimental studies. Scand J Plast Reconstr Surg 3:81-100, 1969.
2. Albrektsson T, Dahl E, Enbom L, Engevall S, Engquist B, Eriksson AR, Feldmann G, Freiberg N, Glantz PO, Kjellman O: Osseointegrated oral implants. A Swedish multicenter study of 8139 consecutively inserted Nobelpharma implants. J Periodontol 59:287-296, 1988.
3. Szmukler-Moncler S, Piattelli A, Favero GA, Dubruille JH:
Considerations preliminary to the application of early and immediate loading protocols in dental implantology. Clin Oral Implants Res 11:12-25, 2000.
4. Buser D, Mericske-Stern R, Bernard JP, Behneke A, Behneke N, Hirt HP, Belser UC, Lang NP: Long-term evaluation of non- submerged ITI implants. Part 1: 8-year life table analysis of a prospective multi-center study with 2359 implants. Clin Oral Implants Res 8:161-172, 1997.
5. Cochran DL, Buser D, ten Bruggenkate CM, Weingart D, Taylor TM, Bernard JP, Peters F, Simpson JP: The use of reduced healing times on ITI implants with a sandblasted and acid-etched (SLA) surface: early results from clinical trials on ITI SLA implants. Clin Oral Implants Res 13:144-153, 2002.
6. Nkenke E, Lehner B, Weinzierl K, Thams U, Neugebauer J, Steveling H, Radespiel-Tröger M, Neukam FW: Bone contact, growth, and density around immediately loaded implants in the mandible of mini pigs. Clin Oral Implants Res 14:312-321, 2003.
7. Huré G, Aguado E, Grizon F, Baslé MF, Chappard D: Some biomechanical and histologic characteristics of early-loaded locking pin and expandable implants: a pilot histologic canine study. Clin Implant Dent Relat Res 6:33-39, 2004.
8. Nkenke E, Hahn M, Weinzierl K, Radespiel-Tröger M, Neukam FW, Engelke K: Implant stability and histomorphometry: a Table 2. Advantage and Disadvantages of Immediate Implant Load-
ing Technique
Advantage of immediate loading
Disadvantage of immediate loading No second stage surgery
(decreased morbidity) Less waiting time
(better soft tissue healing) Less patient visits Monitoring of the implant during healing phase Higher patient acceptance
Increased micro-movement (higher failure rate) Unable to predict final soft and hard tissue outcomes
correlation study in human cadavers using stepped cylinder implants. Clin Oral Implants Res 14:601-609, 2003.
9. Degidi M, Scarano A, Iezzi G, Piattelli A: Histologic analysis of an immediately loaded implant retrieved after 2 months. J Oral Implantol 31:247-254, 2005.
10. Guida L, Iezzi G, Annunziata M, Salierno A, Iuorio G, Costigliola G, Piattelli A: Immediate placement and loading of dental implants: a human histologic case report. J Periodontol
79:575-581, 2008.
11. Cochran DL: The evidence for immediate loading of implants.
J Evid Based Dent Pract 6:155-163, 2006.
12. Cochran DL, Schenk RK, Lussi A, Higginbottom FL, Buser D:
Bone response to unloaded and loaded titanium implants with a sandblasted and acid-etched surface: a histometric study in the canine mandible. J Biomed Mater Res 40:1-11, 1998.