-92-
알레르기 질환의 건강증진과 예방
부산성모병원 이비인후과
구 수 권
Health Promotion and Prevention of Allergic Disease
Soo-Kweon Koo, MD, PhD
Department of Otolaryngology-Head and Neck Surgery, Saint Mary’s Hospital, Busan, Korea
ABSTRACT
The prevalence of allergic diseases have been increasing over the last few decades. These diseases have become a global pu- blic health problem and a burden to health care resources. Allergen exposure in the high risk group is one of the numerous factors contributing to the developing and worsening allergic diseases. Thus, prevention is a very important strategy in treating allergic diseases. This review focuses on environmental risk factors and possible preventive methods in combating allergic diseases.
KEY WORDS:Allergy·Prevention·Environmental factors·Allergen exposure.
서 론
최근 식생활의 변화와 대기오염 등으로 알레르기 질환은 증가하고 있으며 특히 이비인후과 영역의 알레르기 비염은 전 인구의 20~30%를 차지할 정도로 유병률이 높다. 알레르 기 질환의 예방은 질환의 치료와 공공위생에 대단히 중요하 다. 최근 알레르기 질환의 예방과 관련하여 다양한 연구가 진 행되고 있으며 임상적 유용성을 찾는데 많은 노력을 기울이 고 있다. 이에 저자는 이를 정리하고, 소개하여 알레르기 질 환의 예방과 치료에 도움을 주고자 한다.
알레르기 질환의 건강증진과 예방의 단계
건강증진의 정의(Health promotion)
건강증진의 정의는“최적정의 건강유지에 필요한 생활방 식(life style)을 가지도록 하기 위해 개인에 적용할 수 있는 행위들을 말한다. ”로 실제적인 측면에서 요약하면 신체적, 감 정적인 안녕을 추구하고, 수명을 연장하고, 삶의 질을 높이 는 기술적인 행위라고 말할 수 있다. 즉 많은 질병들은 원인
을 모르거나 예측 불가능 한 것이 아니고 개인적인 생활방식 때문에 생기는 것이므로 생활방식을 바꿈으로써 질병을 감 소시킬 수 있다는 개념이다. 따라서 알레르기 질환도 개인의 생활양식(예를 들어 모유수유, 금연 등)과 알레르기 질환과 의 연관성을 규명하고, 교육하여 알레르기 질환의 예방과 치 료에 도움을 줄 수 있으며, 이와 관련된 연구, 교육, 정책, 입 법 등이 건강증진(Health promotion)이다.1)2)
예방(Prevention)의 단계
예방의 3가지 단계는 다음과 같다(Fig.1).3)
1차 예방(Primary prevention)
질환이 발병하기 이전에 원인에 노출되는 것을 방지하여 질환의 발병자체를 예방하는 것으로 금연, 모유수유, 규칙 적인 운동, 영양상담, 예방접종 등이 있다. 알레르기 질환의 1차 예방은 앞으로 알레르기 질환에 감작될 고위험군이지만 아직 감작되지 않은 대상을 예방하는 것을 말한다.4)
2차 예방(Secondary prevention)
예방에 실패하여 질병이 발생된 후 가능한 조기에 진단, 치 료, 관리하여 심각한 합병증으로 진행되는 것을 예방하는 것 이다. 알레르기 질환은 항원에 감작되었지만 질환의 증거가 없는 상태를 대상으로 한다.
논문접수일:2008년 10월 29일
교신저자:구수권, 608-838 부산광역시 남구 용호동 538-41 부산성모병원 이비인후과
전화:(051) 933-7220·전송:(051) 932-8600 E-mail:[email protected]
3차 예방(Tertiary prevention)
만성 질환으로 진행되었을 때 재활치료를 통하여 정상생 활 및 사회활동으로 복귀를 촉진시키는 것을 말한다. 알레르 기 질환은 이미 알레르기 비염이나 천식 등 알레르기 질환을 가진 환자들을 대상으로 한다. 대부분의 연구는 3차 예방과 관련이 있다.
알레르기 질환의 일차예방
(Primary Prevention of Allergic Disease)
알레르기 질환의 일차예방은 임상적 효능에 논란이 많다.5) 최근 고위험군에서 알레르기 비염, 천식 등으로 이행되는 것 을 막기 위해, 조기에 감작의 빈도를 줄이는 연구와 방법이 시도되고 있다.6)7)
Maternal and infant feeding
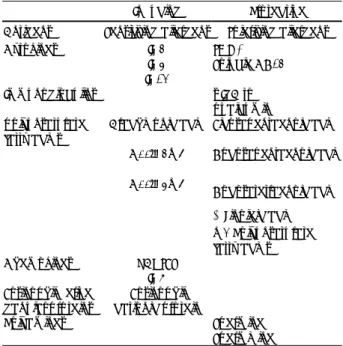
알레르기 질환의 예방에서 모유와 영유아의 섭식은 중요 하다. 2001년 한 연구는 모유수유를 한 영아에서 아토피 피 부염이나 천명이 감소하였으며 이 효과는 4세 이전까지 지 속되다가 그 이후에는 효과가 줄어든다하였다.8) 개발도상국 가에서 실시한 또 다른 연구에서 알레르기 질환이 없는 부모 에게 태어난 영유아에서 지속적으로 모유수유를 하면 알레르 기 질환의 발병률이 낮아진다고 하였지만 부모가 알레르기 질환을 가진 영유아에서는 알레르기 질환의 예방효과가 없 다하였다.9)10) 현재까지의 연구를 통해보면 논란은 있지만 부 모의 알레르기 성향과 상관없이, 모유수유는 면역학적 측면 이나 영유아기의 정서적인 측면에서 모든 영아들에게 권장 되어야 할 것으로 판단된다.11) 모유수유와 알레르기 질환의 예방효과에 대한 논란은 이와 관련된 연구의 방법적 차이, 모유를 구성하고 있는 성분들이 각각 알레르기 질환의 발병 에 서로 다른 효과를 보이는 점, 영유아 개개인의 유전적 차 이 등에 기인한다.12-14) 실제로 모유에는 알레르기를 유발하 는 IL-4, IL-5 등의 cytokine이 있고 이와 반대로 알레르 기 질환을 예방하는 soluble CD-14, s-IgA 등이 포함되어
이론적으로 알레르기 질환의 발병에 서로 다른 효과를 보이 는 물질이 함유되어 있다(Table 1).12)15)
분유를 포함한 영유아기의 섭식은 알레르기 질환의 예방 에 대단히 중요하다. 분유에는 알레르기 질환 발생에 밀접한 관련이 있는 유단백이 함유되어 있으며 최근 이 유단백을 가 수분해하여 제거함으로써 알레르기의 항원성을 현저히 낮춘 가수분해 우유가 사용되고 있다. 실제로 고위험군 영유아에 서 가수분해 우유는 알레르기 질환의 발병율과 우유 알레르 기의 위험을 감소시킨다.16) 아토피의 위험이 높은 영유아에 서 고형식은 6개월부터 시작하며 이때 고형식은 여러 가지 상황을 고려하여 잘 선택해야 한다.17) 유제품은 12개월부터, 계란은 24개월, 땅콩, 생선 등은 적어도 36개월은 지나야 가 능한데 계란, 땅콩, 생선, 해산물과 견과류는 주의를 요한다.
알레르기 질환의 고위험군 산모에서 임신 중 항원을 배제한 음식을 섭식하는 것은 출생할 영유아의 알레르기 질환의 발 병율을 감소시키지 않고 오히려 산모와 태아의 영양 불균형 을 초래 할 수 있어 권장되지 않는다.18) 항원을 배제한 음식 은 수유 중 atopic eczema의 출현을 예방할 수 있지만 좀 더 많은 연구가 필요하다.18)
House dust mites
실내항원을 줄이는 것은 알레르기 질환의 치료에 중요하
다.19)20) 실험실에서 진드기 항원을 줄이는 방법은 실생활 환
경에서 임상적 효과를 얻기가 힘들다. 최근 몇몇 연구자들이
Table 1. Factors in breast milk that are currently being evaluated as either inducing or protecting against food allergies
Inducing Protective
Antigens Sensitizing allergens Tolerizing allergens
Cytokines IL-4
IL-5 IL-13
TGF-β Soluble CD14
Immunoglobulins s-IgA to
ovalbumin polyunsaturated
fatty acids
Arachidonic acid Eicosapentaenoic acid C22:4n-6 Docosapentaenoic acid C22:5n-6
Docosatetraenoic acid α-Linoleic acid n-3 Polyunsaturated fatty acids
Chemokines RANTES
IL-8 Eosinophil-derived
ganular proteins
Eosinophil cationic protein
Polyamines Spermine
Spermidine
Adopted from Friedman NJ, Zeiger RS. The role of breast-feeding in the development of allergies and asthma. J Allergy Clin Immu- nol 2005;115:1238-48
No evidence of allergic Evidence of sensitization Established disease sensitization Not disease Allergic rhinitis Risk group Asthma
Primary prevention
Secondary prevention
Tertiary prevention Fig.1. Three types of prevention of allergic disease.
주목할 만한 결과를 발표하였지만 임신 중이나, 출생 직후에 진드기 항원의 노출을 예방하는 것은 여전히 만족할 만한 결 과를 얻지 못하고 있다.21-26)
Early exposure of pets
출생 초기에 실내 항원에 노출되는 것이 성장 후 알레르기 질환에 대한 감작과 임상증상을 일으키는데 영향을 주는지 는 논란이 많다.27-29) 독일과30)31) 덴마크의32) 최근 연구에서 출생초기에 고양이 항원에 노출되는 것이 알레르기 질환의 감작과 임상증상을 일으키는데 밀접한 연관이 있다하였지만 또 다른 연구는 알레르기 비염의 발현에 영향을 주지 않는 다 하였다.33) 어떤 연구는 출생 초기에 강아지나 고양이 항 원에 노출되는 것이 오히려 알레르기 증상의 발현을 예방한 다고 하여 서로 다른 견해를 주장하기도 하였다.34-37) 이런 차이점은 연구 방법에 따른 많은 변수에 기인한다. 어떤 연 구에서는 면역학적으로 실내 먼지 속에 있는 고양이 항원인 Fel d1에 노출된 소아에서 IgE항체 생성 없이 IgG, IgG4를 형성하며 이런 변형된 Th2 반응으로 알레르기 증상 없이 면역학적 내성을 형성한다 하였다.38)39)
Occupational agents
공장 근로자들에 있어 천식의 일차적 예방에 대한 많은 연 구가 진행되고 있으며 다양한 방법이 제시되고 있다.40-42) 의 료관련 종사자들에게 latex 알레르기의 일차적 예방은 아직 도 논란이 있지만 근로환경에서 latex항원의 농도를 줄이는 것은 중요하다.43)44)
Environmental tobacco smoke
임신 중 흡연에 노출된 태아는 폐기능 저하와 기도 단면 적의 감소로 폐의 성장과 기도에 나쁜 영향을 미치게 되며 특히 천식의 가족력이 있거나 임신고혈압 산모에서 더 심각
하다.45)46) 실제로 부모의 흡연에 의해 담배 연기에 노출된
영유아는 생후 1세 때 알레르기 발병이 2배 이상 높게 나타 나고 소아 알레르기비염의 증상 유발에 부모의 흡연여부가 많은 영향을 끼치는 것으로 보고된다.47) 간접흡연은 담배연 기가 필터를 통하지 않고 대기 중으로 직접 연소되는데 직접 흡연보다 독성이 강해서 호흡기 점막을 더 자극하며, 알레르 기비염, 소아기 천식이나 천명에 밀접한 관련이 있다. 간접 흡연이 출생 전과 출생 후 어떤 시기에 더 중요한지는 논란 이 있다. 최근 연구는 출생 전 간접흡연도 출생 후 간접흡연 만큼 호흡기능에 치명적인 영향을 준다하였고48) 어떤 연구 는 출생 전 간접흡연이 더 중요하다 주장하여49) 산모의 직, 간 접 흡연의 중요성을 강조하였다. 부모의 흡연과 atopy, ecze-
ma, rhinitis 등은 연관이 없다는 보고도 있지만50) 알레르기 질환의 일차적 예방에 부모와 보호자, 환자는 금연해야 하 며, 출생 전부터 어린이는 간접흡연의 환경으로부터 보호되 어야 한다.
Prevention of the development of asthma in rhinitis patients
항원의 예방접종은 알레르기 질환의 임상증상을 개선시키 는데 주로 사용하지만 알레르기 질환의 예방에도 효과가 있 다. 실제적으로 몇몇 연구에서 알레르기 비염 등으로 면역치 료를 받은 환아의 경우 천식의 발현을 현저히 낮춘다고 하 였다.51) 설하 면역요법(Sublingual immunotherapy)은 아직 은 더 많은 연구가 진행되어야 하지만 일반적으로 면역치료 와 동일한 효과가 있고 현재의 면역치료보다 좀 더 일찍 시 작할 수 있음으로 알레르기 질환의 이차적 예방에 중요한 역 할을 할 것으로 생각된다.52) Ketotifen,53) Cetrizine 등54)55) 과 같은 약물을 천식발현이 예상되는 고위험군에서 예방적 목적으로 사용하기도 하는데 일부 천명을 감소시키는 효능 은 있지만 좀 더 많은 연구가 필요하다.55)
현재까지의 연구결과를 보면 알레르기 질환의 일차예방은 모유수유, 임신 중 산모와 영유아에서 간접흡연에 대한 예방, 작업장에서의 알레르기 항원에 대한 노출 제한 등이 권장되 고 있고 식이제한이나, 실내항원의 조절은 예방적 효능에 대 해 아직까지 논란의 여지가 많다.
알레르기 질환의 이차예방(Secondary Prevention of Allergic Disease)
항원에 감작은 되었으나 질환의 증거가 없는 경우를 대상 으로 한다. 임상적으로 감작의 유무를 알 수 없는 경우가 많 아 이차예방은 더 많은 연구가 필요하다.
알레르기 질환의 삼차예방(Tertiary Prevention of Allergic Disease)
Inhalation-allergen avoidance
알레르기 비염의 가장 중요한 흡입항원은 집먼지 진드기
이다.20)56) 흡입항원의 예방과 관련된 대부분의 연구는 천식
과 관련되어 있고 알레르기 비염에 관한 연구는 흔하지 않다.
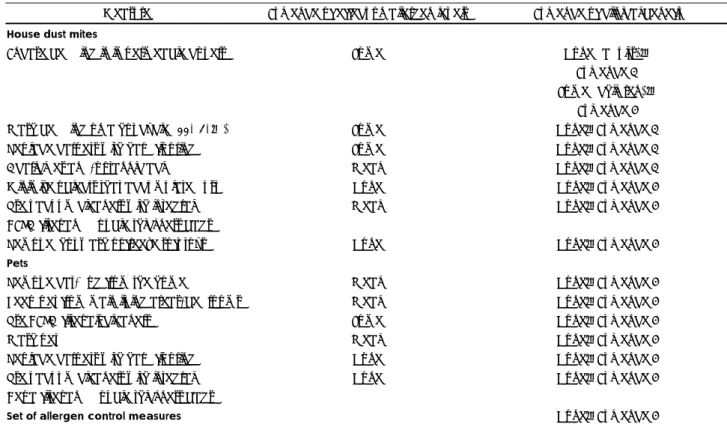
불행하게도 흡입항원의 예방은 임상양상을 개선하는데 한계 점을 가지고 있다.57) 특히 흡입항원의 예방에 있어 물리적, 화학적 방법의 효능은 만족스럽지 못하며 단일 방법만 사용 해서는 알레르기 질환의 개선을 가져 올 수 없다(Table 2).58)59)
집먼지 진드기가 통과할 수 없는 베개나 침구의 덮개에 대한 연구에서 대략 30% 정도 항원(Der p l)의 감소를 보이지만 알 레르기 질환의 예방효과는 큰 차이가 없다하였고60)61) 강력하 게 먼지를 걸러낼 수 있는 HEPA filter(High Efficiency Par- ticulate filter)도 큰 차이가 없다하였다.62) 하지만 다양한 방 법(청소, 카펫 치우기, 덮개 사용 등)을 통해 항원이 제거된 주거 환경을 만들었을 때 Fel d 1이 6.8% 감소하였으며 비 염증상이 현저하게 개선되었다고 보고한 연구도 있다.63) 결 론적으로 흡입항원의 회피는 임상적인 증상의 개선을 가져 오지만 단일한 물리적, 화학적 방법(덮개, HEPA filter 등) 만을 사용해서는 임상양상의 개선을 가져올 수 없다. 동물 털에 알레르기 반응을 보이는 환자에서 집안에 동물을 기르 지 않는 방법은 권장할 만한 방법이지만 공공시설이나 학교 등에서 노출될 수 있음으로 그 예방적 효능은 좀 더 많은 연구가 필요하다.
Occupational agents
작업장에서 천식, 알레르기 비염과 관련 있는 원인항원의 완전한 제거가 중요하며, 직업과 관련한 알레르기 질환(occu- pational allergic disease)은 조기 진단이 3차 예방에 대단 히 중요하다. 이는 알레르기 질환을 유발하는 작업장에서 조
기에 격리시킬수록 질환의 치료가 용이하기 때문이다.64) 3차 예방에 있어 원인 물질로부터 완전한 격리가 가장 중요하지 만 latex알레르기의 경우 powder를 묻히지 않은 수술용 장 갑 등은 항원의 정도가 미약하여 대부분 계속 사용하는 것이 허용되어 있다.65) 원인 물질의 완전한 격리가 불가능할 경우 다양한 방법을 통하여 조절하는 것이 권장된다.
Indoor and outdoor air pollutants
대기 오염물질은 대개 비알레르기성 비염과 관련이 있으 며 알레르기 비염환자를 악화시킨다. 대기오염은 특히 빈곤 층에 많은 문제를 일으키며 환기. 습도조절, 담배연기나 매 연의 실내 유입 차단 등이 권장되고 있지만, 효능에 관련된 연구는 거의 없는 실정이다.66-69)
결 론
알레르기 질환은 치료보다 예방이 중요하다. 최근 알레르 기 질환의 예방과 관련하여 많은 연구들이 진행되고 있으며, 금연이나 모유수유 등 공공위생과 관련된 예방적 개념이 강 조되고 있다. 알레르기 질환에서 가장 대표적인 질환인 알레 르기 비염을 담당하는 이비인후과 의사들은 예방의 개념과
Table 2. Effectiveness of avoidance measures in rhinitis and asthma for certain indoor allergens
Measure Evidence of effect on allergen levels Evidence of clinical benefit House dust mites
Encase bedding in impermeable covers Some None (adults):
Evidence A
Some (children):
Evidence B
Wash bedding on a hot cycle (55-60℃) Some None:Evidence A
Replace carpets with hard flooring Some None:Evidence A
Acaricides and/or tannic acid Weak None:Evidence A
Minimize objects that accumulate dust None None:Evidence B
Use vacuum cleaners with integral Weak None:Evidence B
HEPA filter and double-thickness bags
Remove, hot wash or freeze soft toys None None:Evidence B
Pets
Remove cat/dog from the home Weak None:Evidence B
Keep pet from main living areas/bedrooms Weak None:Evidence B
Use HEPA-filter air cleaners Some None:Evidence B
Wash pet Weak None:Evidence B
Replace carpets with hard flooring None None:Evidence B
Use vacuum cleaners with integral None None:Evidence B
Hepa filter and double-thickness bags
Set of allergen control measures None:Evidence B
Adopted from Custovic A, Wijk RG. The effectiveness of measures to change the indoor environment in the treatment of allergic rhinitis and asthma. Allergy 2005;60:1112-5
예방과 관련된 다양한 연구결과의 이해가 필요하다 하겠다.
중심 단어:알레르기 질환·예방·환경요인·알레르겐노출.
REFERENCES
1) Tang K, Beaglehole R, O’Byrne D. Policy and partnership for health promotion-addressing th determinants of health. World Health Organ Bull 2005;83:884-5.
2) Asher I, Baena-Cagnani C, Boner A, Canonica GW, Chuchalin A, Custovic A, et al. World Allergy Organization guidelines for pre- vention of allergy and allergic asthma. Int Arch Allergy Immunol 2004;135:83-92.
3) Last J. A dictionary of epidemiology New York: Oxford University Press;1995. p.135.
4) Warner JA. Primary sensitization in infants. Ann Allergy Asthma Immunol 1999;83:426-30.
5) Becker A. Prevention strategies for asthma-primary prevention.
CMAJ 2005;173(Suppl 6):S20-S4.
6) Chan-Yeung M, Becker A. Primary prevention of childhood asthma and allergic disorders. Curr Opin Allergy Clin Immunol 2006;6:146-51.
7) Prescott SL, Tang ML. The Australasian Society of Clinical Immu- nology and Allergy position statement: summary of allergy preven- tion in child. Med J Aust 2005;182:464-7.
8) Gdalevich M, Mimouni D, Mimouni M. Breast-feeding and the risk of bronchial asthma in childhood: a systematic review with meta- analysis of prospective studies. J Pediatr 2001;139:261-6.
9) Oddy WH, Holt PG, Sly PD, Read AW, Landau LI, Stanley FJ, et al. Association between breast feeding and asthma in 6 year old chil- dren: findings of a prospective birth control study. BMJ 1999;319:
815-9.
10) Burgess SW, Dakin CJ, O’Callaghan MJ. Breastfeeding does not increase the risk of asthma at 14 years. Pediatrics 2006;117:e787-e92.
11) Kramer MS, Kakuma R. The optimal duration of exclusive breast- feeding: a systematic review. Adv Exp Med Biol 2004;554:63-77.
12) Friedman NJ, Zeiger RS. The role of breast-feeding in the development of allergies and asthma. J Allergy Clin Immunol 2005;115:1238-48.
13) Hoekstra MO, Niers LE, Steenhuis TJ, Rovers M, Knol EF, Uitter- waal CS. Is randomization of breast-feeding feasible? J Allergy Clin Immunol 2005;115:1324.
14) Lowe AJ, Carlin JB, Bennett CM, Abramson MJ, Hosking CS, Hill DJ, et al. Atopic disease and breast-feeding-cause or consequence? J Allergy Clin Immunol 2006;117:682-7.
15) Friedman NJ, Zeiger RZ. Prevention and natural history of food allergy. In: Leung DYM, Sampson HA, Geha RS, Szefler SJ, edi- tors. Pediatric allergy, principles and practice. St Louis: Mosby, Inc;
2003. p.496.
16) Osborn DA, Sinn J. Formulas containing hydrolyzed protein for pre- vention of allergy and food intolerance in infants. Cochrane Data- base Syst Rev 2004;3:CD003741.
17) Fiocchi A, Assa’ad A, Bahna S. Food allergy and the introduction of solid foods to infants: a consensus document. Adverse Reaction to Food Committee, Americam College of Allergy, Asthma and Immu- nology. Ann Allergy Asthma Immunol 2006;97:10-20;quiz 1,77.
18) Kramer M, Kakuma R. Maternal dietary antigen avoidance during pre- gnancy or lactation, or both, for preventing or teaching atopic dis- ease in the child. Cohrane Database Syst Rev 2006;3:CD000133.
19) Sporik R, Holgate ST, Platis-Mills TA, Cogswell JJ. Exposure to house dust mite allergen (Der P 1) and the development asthma in childhood. A prospective study. N Engl J Med 1990;323:502-7.
20) Wahn U, Lau S, Bergmann R, Kulig M, Forster J, Bergmann K, et al.
Indoor allergen exposure is a risk factor for sensitization during the first three years of life. J Allergy Clin Immunol 1997;99:763-9.
21) van Strien RT, Koopman LP, Kerkhof M, Spithoven J, de Jongste JC, Gerritsen J, et al. Mite and pet allergen levels in homes of children born to allergic and nonallergic parents: the PIAMA study. Environ Health Perspect 2002;110:A693-A8.
22) Corver K, Kerkhof M, Brussee JE, Brunekreef B, van Strien RT, Vos AP, et al. House dust mite allergen reduction and allergy at 4 yr:
follow up of the PIAMA-study. Pediatr allergy Immunol 2006;17:
329-36.
23) Simpson A, Custovic A. Allergen avoidance in the primary preven- tion of asthma. Cur Opin Allrgy Clin Immunol 2004;4:45-51.
24) Simpson A, Simpson B, Custovic A, Craven M, Woodcock A. Stringent environmental control in pregnancy and early life: the long-term ef- fects on mite, cat and dog allergen. Clin Exp Allergy 2003;33:1183-9.
25) Horak F Jr, Matthews S, Ihorst G, Arshad SH, Frischer T, Kuehr J, et al. Effect of mite-impermeable mattress encasings and an educa- tional package on the development of allergies in a multinational ran- domized, controlled birth-cohort study-24 months results of the Study of Prevention of Allergy in Children in Europe. Clin Exp Allergy 2004;
34:1220-5.
26) Mihrshahi S, Peat JK, Marks GB, Mellis CM, Tovey ER, Webb K, et al. Eighteen-month outcomes of house dust mite avoidance and dietary fatty acid modification in the Child-hood Asthma Prevention Study (CAPS). J Allergy Clin Immunol 2003;111:162-8.
27) Strachan DP. Is allergic disease programmed in early life? [editorial;
comment].Clin Exp Allergy 1994;24:603-5.
28) Wahn U, Bergmann R, Kulig M, Forster J, Bauer CP. The natural course of sensitization and atopic disease in infancy and childhood.
Pediatr Allergy Immunol 1997;8(Suppl10):16-20.
29) Illi S, von Mutius E, Lau S, Niggemann B, Gruber C, Wahn U. Peren- nial allergen sensitization early in life and chronic asthma in child- ren: a birth cohort study. Lancet 2006;368:763-70.
30) Lau S, Illi S, Sommerfeld C, Niggemann B, Bergmann R, von Mutius E, et al. Early exposure to house-dust mite and cat allergens and de- velopment of childhood asthma: a cohort study. Multicentre Allergy Study Group. Lancet 2000;356:1392-7.
31) Lau S, Illi S, Platts-Mills TA, Riposo D, Nickel R, Gruber C, et al.
Longitudinal study on the relationship between cat allergen and en- dotoxin exposure, sensitization, cat-specific IgG and development of asthma in childhood-report of the German Multicentre Allergy Study (MAS 90). Allergy 2005;60:766-73.
32) Brussee JE, Smit HA, van Strien RT, Corver K, Kerkhof M, Wijga AH, et al. Allergen exposure in infancy and the development of sen- sitization, wheeze, and asthma at 4 years. J Allergy Clin Immunol 2005;
105:946-52.
33) Frosh AC, Sandhu G, Joyce R, Strachan DP. Prevalence of rhinitis, pillow type and past and present ownership of furred pets [see com- ments]. Clin Exp Allergy 1999;29:457-60.
34) Hesselmar B, Aberg N, Aberg B, Eriksson B, Bjoksten B. Does early exposure to cat or dog protect against later allergy development? [In Process Citation]. Clin Exp Allergy 1999;29:611-7.
35) Ownby DR, Johnson CC, Peterson EL. Exposure to dogs and cats in the first year of life and risk of allergic sensitization at 6 to 7 years of age. JAMA 2002;288:963-72.
36) Nafstad P, Magnus P, Gaarder PI, Jaakkola JJ, Exposure to pets and atopy-related diseases in the first 4 years of life. Allergy 2001;56:
307-12.
37) Svanes C, Heinrich J, Jarvis D, Chinn S, Omenaas E, Gulsvik A, et al.
Pet-keeping in childhood and adult asthma and hay fever: Euro-pean community respiratory health survey. J Allergy Clin Immunol 2003;
112:289-300.
38) Platts-Mills T, Vaughan J, Squillace S, Woodfolk J, Sporik R. Sen- sitization, asthma, and a modified Th2 response in children exposed
to cat allergen: a population-based cross sectional study. Lancet 2001;
357:752-6.
39) Woodfolk JA, Platts-Mills TA. The immune response to intrinsic and extrinsic allergens: determinants of allergic disease. Int Arch Allergy Immunol 2002;129:277-85.
40) Cullinan P, Harris JM, Newman Taylor AJ, Hole AM, Jones M, Bar- nes F, et al. An outbreak of asthma in a modern detergent factory.
Lancet 2000;356:1899-900.
41) Cathcart M, Nicholson P, Roberts D, Bazley M, Juniper C, Murray P, et al. Enzyme exposure, smoking and lung function in employees in the detergent industry over 20 years. Medical Subcommittee of the UK Soap and Detergent Industry Association. Occup Med Oxf 1997;
47:473-8.
42) Sarlo K. Control of occupational asthma and allergy in the detergent industry. Ann Allergy Asthma Immunol 2003;(5 Suppl. 2):32-4.
43) Filon FL, Radman G. Latex allergy; a follow up study of 1040 heal- thcare workers. Occup Environ Med 2006;63:121-5.
44) Tarlo SM, Liss GM. Prevention of occupational asthma-practical impli- cations for occupational physicians. Occup Med (Lond) 2005;55:588-94.
45) Stick SM, Burton PR, Gurrin L, Sly PD, LeSouef PN. Effects of maternal smoking during pregnancy and a family history of asthma on respiratory function in newborn infants. Lancet 1996;348:1060-4.
46) Lodrup Carlsen KC, Jaakkola JJ, Nafstad P, Carlsen KH. In utero exposure to cigarette smoking influences lung function at birth. Eur Respir J 1997;10(8):1774-9.
47) Zuraimi MS, Tham KW, Chew FT, Ooi PL, David K. Home exposure to environmental tobacco smoke and allergic symptoms among young children in Singapore. Int Arch Allergy Immunol 2008;146(1):57-65.
48) Lux AL, Henderson AJ, Pocock SJ. Wheeze associated with prenatal tobacco smoke exposure: a prospective, longitudinal study. ALSPAC Study Team. Arch Dis Child 2000;83:307-12.
49) Lannero E, Wickman M, Pershagen G, Nordvall L. Maternal smoking during pregnancy increases the risk of recurrent wheezing during the first years of life (BAMSE). Respir Res 2006;7:3.
50) Raherison C, Penard-Morand C, Moreau D, Caillaud D, Charpin D, Kopfersmitt C, et al. In utero and childhood exposure to parental to- bacco smoke, and allergies in schoolchildren. Respir Med 2007;101:
107-17.
51) Johnstone D, Dutton A. The value of. hyposensitization therapy for bronchial asthma in children: a fourteen-years study. Pediatrics 1968;
42:793-802.
52) Pajno GB, Morabito L, Barberio G, Parmiani S. Clinical and immu- nologic effects of long-term sublingual immunotherapy in asthmatic children sensitized to mite: a double blind, placebo-controlled study.
Allergy 2000;55:842-9.
53) Iikura Y, Naspitz CK, Mikawa H, Talaricoficho S, Baba M, Sole D, et al. Prevention of asthma by ketotifen in infants with atopic der- matitis. Ann Allergy 1992;68:233-6.
54) Warner JO. A double-blinded, randomized. placebo-controlled trial of cetrizine in preventing the onset of asthma in chidren, with atopic der-
matitis: 18 months’ treatment and 18 months’ posttreatment follow- up. J Allergy Clin Immunol 2001;108:929-37.
55) Warner JO. Early treatment of atopic child. Pediatr Allergy Immunol 1997;8(suppl 10):46-8.
56) Platts-Mills TA. The role of immunoglobulin E in allergy and asthma.
AM J Respir Crit Care Med 2001;164:S1-S5.
57) Global Strategy for asthma Management and Prevention. GINA. Up- date from NHLBI/WHO Workshop Report 1995, Available at: www.
ginasthma.com, revised 2006;2006.
58) Sheikh A, Hurwitz B, Shehata Y. House dust mite avoidance mea- sures for perennial allergic rhinitis. Cochrane Database Syst Rev 2007;
24:CD001563.
59) Custovic A, Wijk RG. The effectiveness of measures to change the in- door environment in the treatment of allergic rhinitis and asthma. Aller- gy 2005;60:1112-5.
60) Terreehorst I, Hak E, Oosting AJ, Tempels-Pavlica Z, De Monchy JG, Bruijnzeel-Koomen CA, et al. Evaluation of impermeable covers for bedding in patients with allergic rhinitis. N Engl J Med 2003;3:237-46.
61) Terreehorst I, Duivenvoorden HJ, Tempels Pavlica Z, Oosting AJ, De- monchy JG, Bruijnzeel-Koomen CA, et al. The effect of encasings on quality of life in adult house dust mite allergic patients with rhinitis, asthma and/or atopic dermatitis. Allergy 2005;60:888-93.
62) Wood RA, Johnson EF, Van Natta ML, Chen PH, Eggleston PA. A placebo- controlled trial of a HEPA air cleaner in the treatment of cat allergy. Am J Respir Crit Care Med 1998;158:115-20.
63) Bjornsdottir US, Jakobinudottir S, Runarsdottir V, Juliusson S. The effect of reducing levels of cat allergen (Fel d 1) on clinical symptoms in patients with cat allergy. Ann Allergy Asthma Immunol 2003;91:
189-94.
64) Cullinan P, Tarlo S, Nemery B. The prevention of occupational asthma.
Eur Respir J 2003;22:853-60.
65) Vandenplas O, Jamart J, Delwiche JP, Evrard G, Larbanois A. Occup- ational asthma caused by natural rubber latex: outcome according to cessation or reduction of exposure. J Allergy Clin Immunol 2002;109:
125-30.
66) Eggleston PA, Butz A, Rand C, Curtin-Brosnan J, Kanchanaraksa S, Swartz L, et al. Home environmental intervention in inner-city asthma:
a randomized controlled clinical trial. Ann Allergy Asthma Immunol 2005;95:518-24.
67) Kattan M, Stearns SC, Crain EF, Stout JW, Gergen PJ, Evans R III, et al. Cost-effectiveness of a home-based environmental intervention for inner-city children with asthma. J Allergy Clin Immunol 2005:
116:1058-63.
68) Morgan WJ, Crain EF, Gruchalla RS, O’Connor GT, Kattan M, Evans R III, et al. Results of a Home-Based Environmental Intervention Among Urban Children with Asthma. N Engl J Med 2004;351: 1068-80.
69) Williams SG, Brown CM, Falter KH, Alverson CJ, Gotway- Crawford C, Homa D, et al. Does a multifaceted environmental intervention alter the impact of asthma on inner-city children? J Natl Med Assoc 2006;98:249-60.