- 11 -
KISEP Original Articles J Rhinol 5((((1)))), 1998
A Comparison of the Therapeutic Effects of Powder and Aerosolized Budesonide in the Treatment of Perennial Allergic Rhinitis
Yang-Gi Min, M.D., Hong-Ju Park, M.D., Ji-Hun Mo, M.D., Ja Bock Yun, M.D., In-Ho Jung, M.D. and Tae-Young Kwon, M.D.
ABSTRACT
The aims of this study are to compare the efficacy and side effects of intranasal budesonide as a dry powder and as a freon- propelled pressurized aerosol in the treatment of perennial allergic rhinitis and to assess the difference in compliance with the powder and aerosol. The study design was a randomized, double-blind crossover between two treatment groups over a six-week period. Twelve patients with symptomatic perennial allergic rhinitis received 400 μg of intranasal budesonide administered daily as two puffs/nostril/day of the drug delivered by a freon-propelled aerosol for the first three weeks and as one inhalation/
nostril/day of the pure drug powder for the next three weeks. Fourteen adults with allergic rhinitis received the drug in the reverse sequence. Patients recorded daily symptoms on diaries, and, at each clinic visit, adverse effects were recorded. Compliance with the powder and with the aerosol was also evaluated. During the six weeks, there were significant improvements in symptoms in both treatment groups, and the differences in efficacy and compliance with the medication between the two groups were not si- gnificant. Adverse effects included headaches, epistaxis, and nasal dryness;however, they were not serious and equally dist- ributed in the two groups. We conclude that powder and aerosolized budesonide improve the symptoms of perennial allergic rhinitis significantly with little difference in efficacy, side effects, and preference.
KEY WORDS:Budesonide·Turbuhaler·Propellant inhaler·Allergic rhinitis.
INTRODUCTION
Rhinitis is defined as inflammation of the nasal mucosa, and is characterized by expression of more than one of these sy- mptoms:nasal obstruction, rhinorrhea, sneezing, and nasal it- ching. The inflammation in allergic rhinitis is associated with the infiltration of inflammatory cells such as eosinophils and mast cells. The release of inflammatory mediators by these cells results in vasodilatation of nasal mucosa, tissue edema, nasal edema and nasal obstruction. It also induces hypersecretion of nasal mucosal glands, nasal itching, and nasal sneezing.
The treatment of allergic rhinitis has been focused on the blockage or release of inflammatory mediators by such medi- cations as antihistamines or disodium cromoglycate. However, their anti-inflammatory effect has not been proven clinically.
Though these medications can help to relieve nasal symptoms,
they cannot resolve the inflammation of the nasal mucosa ef- fectively. Since the underlying pathology in perennial allergic rhinitis is usually an inflammatory reaction, nasally applied corticosteroids may produce greater clinical benefits than other medication. Recently, topical steroids have been used widely for the treatment of allergic rhinitis. Budesonide, one of the topical steroids, has been reported to have a significant effect on allergic rhinitis. There are two types of delivery systems for budesonide:the freon-propelled aerosol delivery system and the turbine inhaler system (Turbuhaler). The Turbuhaler system was recently developed as an alternative to the freon-propelled aerosol delivery system due to environmental awareness and side effects such as drying and caking of the nasal mucosa. Tu- rbuhaler allows the drug to be released and insufflated at very low inspiratory flow rates, thus making it adaptable for nasal use.
In this study, we compared the efficacy and side effects of intranasal budesonide delivered by Turbuhaler with the conv- entional freon-propelled nasal spray for the treatment of per- ennial allergic rhinitis. We have also evaluated the preferences for the two types of delivery system.
MATERIALS AND METHODS
Twenty-six patients were enrolled in the study-14 men and
Department of Otorhinolaryngology-Head and Neck Surgery,Seoul National University College of Medicine, Seoul, Korea Address correspondences and reprint requests to Yang-Gi Min, M.D., Department of Otorhinolaryngology-Head and Neck Su- rgery, College of Medicine, Seoul National University, 28 Yon- gon-Dong, Chongno-Gu, Seoul, 110-714, Korea
Tel:82-2-760-2446, Fax:82-2-744-9935 Accepted for publication on April 5, 1998
12 / J Rhinol 5(1), 1998
12 women with a mean age of 28.5 years (range:16-58 ye- ars). They had a history of perennial allergic rhinitis with a mean duration of 2.57 years (range:1-11 years).
Of the 12 patients given aerosolized budesonide during the first three weeks (Group A:six male, six female, mean age 27.7 years), all of the patients completed the study. All of the 14 patients given budesonide powder during the first three we- eks (Group B:eight male, six female, mean age 29.2 years) also completed the study (Table 1). Patients were enrolled in this study successively from September 1996 through Sept- ember 1997. They had more than two of the following symp- toms for more than an hour daily:nasal itching, watery rhi- norrhea, sneezing, nasal obstruction. They had strongly positive skin prick tests to Dermatophagoides pteronyssinus and De-
rmatophagoides farinae, and showed RAST scores of morethan three to the two common allergens. Patients with infectious or atrophic rhinitis, severe nasal septal deformities, nasal pol- yposis, systemic diseases such as diabetes mellitus, tuberculosis, or hepatic disease were excluded from this study. Patients who had used a nasal steroid within two months of enrollment, antihistamines or vasoconstrictor within three days of enrollment, or immunotherapy within the last two years were also excluded.
All patients signed an informed consent form.
After satisfaction of the initial entry criteria, all patients were given a symptom diary for one week. Those patients who re- corded more than two of the nasal symptoms were included in the study.
After a one week run-in period, two active three-week trea- tment periods with a crossover at the end of the first three-week period ensued. Patients were assigned randomly by computerized method to receive either aerosolized budesonide during the first three weeks followed by budesonide powder during the second three-week period (Group A:n=12), or budesonide powder for three weeks followed by aerosolized budesonide for three weeks (Group B:n=14). Blindness was maintained using the double dummy technique.
Treatment was composed of nominal 400 μg daily doses of budesonide powder or aerosol. Aerosolized budesonide was administered as two puffs of 50 μg dosage in each nasal cavity in the morning and evening; budesonide powder, as two puffs of 100 μg dosage in each nasal cavity in the mo- rning.
To assess efficacy, the severity of nasal symptoms, such as sneezing, watery rhinorrhea, nasal itching, and nasal obstruc- tion, was recorded on a diary using a four-point scale (0=none,
1=mild-present but not troublesome, 2=moderate-frequently troublesome but not sufficient to interfere with normal daily activity or night time sleep, 3=severe-sufficiently troublesome to interfere with normal daily activity or night-time sleep).
Patients were assessed on four separate occasions:at trial entry, at the end of the run-in period, at crossover, and at the end of the trial. At trial entry, demographic details such as name, identification number, sex, and age were recorded. The severity of rhinitis was assessed on a four-point scale (0=none;1=
mild;2=moderate;3=severe) at all visits. At each visit, symptom diaries were checked for accuracy.
For assessment of safety, all patients were asked whether they had suffered any adverse reactions to the medication. If there were any adverse effects, the severity, frequency, and du- ration were evaluated and the causal relationship with the drug was estimated. At the end of the trial, patients were asked to specify which of the two treatments they thought had been more effective and to state compliance. Compliance was ass- essed on a three-point scale (0=not good, 1=good, 2=very good) and patients who noted not good were asked to give reasons for the non-compliance.
Statistical analysis
To assess efficacy, daily symptom scores from the diaries were averaged into mean scores for each patient at each clinic visit. Wilcoxon’s signed rank tests were used to analyze the difference of efficacy at each clinic visit. Differences between the two treatment groups and changes over time for these sc- ores were examined using a repeated measures analysis of variance (ANOVA). If the p-value was less than 0.05, the di- fferences were considered significant. All adverse reactions were evaluated to estimate the safety of budesonide. Compliance with the two treatment modalities was analyzed using Wilco- xon’s signed rank test.
RESULTS Efficacy
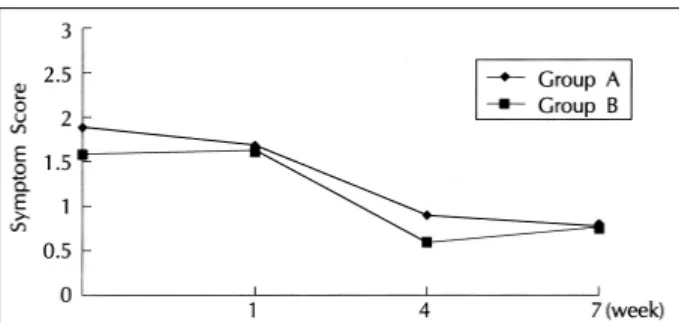
Figures 1 to 4 show the patterns of mean daily score varia- tion throughout the trial for sneezing, watery rhinorrhea, itchy nose, and blocked nose, respectively.
After three weeks of initial treatment, symptom scores for sneezing, watery rhinorrhea, and nasal obstruction showed ma- rked reductions in Group A (sneezing p=0.016, watery rhin- orrhea p=0.016, nasal obstruction p=0.004) and all symptom scores in group B showed significant decrease (sneezing p=
0.002, watery rhinorrhea p=0.016, nasal itching p=0.016, nasal obstruction p=0.039). Symptom scores for nasal itching in group A did not showed significant decrease. The total sum
Table 1. Patients characteristics
Group A Group B
Number 12 14 Sex(M/F) 6/6 8/6 Age(year) 27.7 29.2
Min et al:Budesonide in Allergic Rhinitis / 13
of symptom scores showed marked reductions in both groups (Group A:4.92→2.00, Group B:6.36→2.79).
After crossover, symptom scores in both groups did not ch- ange significantly as compared to those after three weeks of initial treatment. However, when compared to those after the run-in period, all nasal symptom scores except for nasal itching in group A changed significantly in both groups (Group A:
sneezing p=0.008, watery rhinorrhea p=0.078, nasal itching
p=0.85, nasal obstruction p=0.002;Group B:sneezing p=0.001, watery rhinorrhea p=0.002, nasal itching p=0.016, nasal obstruction p=0.014).
There were no significant differences between therapeutic effects in the two treatment groups (sneezing p=0.2872, wa- tery rhinorrhea p=0.2154, nasal itching p=0.2094, nasal ob- struction p=0.3054).
Adverse effects
A total of three adverse effects were reported by three pat-
ients (8%) when using aerosolized budesonide as compared with two events reported by two patients (5.6%) using bude- sonide powder. These are summarized in Table 2. None of the adverse effects were serious or lasted longer than three days.
Compliance
At the end of the trial, three patients showed better comp- liance with aerosolized budesonide, two patients showed better compliance with budesonide powder, and the remaining 21 patients showed equal compliance to the two types of delivery systems. The mean values of compliance scores for aerosolized budesonide and budesonide powder were 1.73 and 1.65, and there was no significant difference in compliance between ae- rosolized form and powder (p=0.9614).
DISCUSSION
This study shows that the daily administration of 400 μg budesonide either as a pure powder or carried by a freon-pro- pelled aerosol improves nasal symptoms of perennial allergic rhinitis patients. All symptom scores showed statistically sig- nificant improvements in both group A and B, but the symptom score for nasal itching in group A did not reach statistical si- gnificance. This may be due to the fact that the mean symptom score of nasal itching of group A was too low (0.33) as com- pared to that of group B (1.07). Only three of 12 patients in group A complained of nasal itching. Two patients with mild nasal itching showed no improvement, but it was not troubl- esome. The one patient with moderate nasal itching showed improvement after the treatment into no nasal itching sensation.
The fact that the mean symptom score for nasal itching in
Table 2. Adverse effects
Adverse Effects Group A (n=12) Group B (n=14)
Nausea 1 0 Headache 1 0 Epistaxis 1 1 Nasal dryness 0 1
Total 3 2
Fig. 1. Changes of symptom scores for sneezing.
Fig. 2. Changes of symptom scores for rhinorrhea.
Fig. 3. Changes of symptom scores for nasal itching.
Fig. 4. Changes of symptom scores for nasal obstruction.
14 / J Rhinol 5(1), 1998
group B reduced significantly after the use of budesonide su- pports good control of nasal itching. Other studies also have shown good control of nasal itching with budesonide.
1)2)Viner and Jackman observed in a retrospective study that the most common symptom of perennial rhinitis is nasal obstruction;
they reported an incidence of 53% in 961 patients surveyed.
3)Several studies have shown budesonide to be effective in co- ntrolling nasal obstruction.
4-8)In a placebo-controlled study, administration of budesonide reduced the degree of hypertrophy of the conchae, as well as in edema, secretion and obstruction of nasal mucosa significantly.
9)In this study, budesonide also provided significantly good control of nasal obstruction in both treatment groups (Group A:p=0.004;Group B:p=0.039).
In cases of severe nasal obstruction, aerosolized budesonide can be used without limitation;however, there are some li- mitations in using budesonide powder. An inspiratory flow rate of more than 20 L/min is needed for effective distribution of budesonide powder. Though this is a low flow rate, total nasal obstruction sometimes occurs when symptoms aggravate se- verely. It would be required for the patient to use a topical decongestant prior to administration of budesonide powder.
The effectiveness of intranasal budesonide in treating per- ennial allergic rhinitis have been reported in several placebo controlled studies.
2)3)Long term studies of one-to-five-year duration have confirmed both the efficacy and safety of intra- nasal budesonide as a treatment for perennial rhinitis and re- vealed no influence on the hypothalamic-pituitary adrenal axis when administered in intranasal doses of 400 μg.
9)10)Juniper et al. reported that headaches, epistaxis, nasal dry- ness, nasal soreness, and dry mouth were common adverse re- actions. More than half of the patients reported headaches, or nosebleeds.
4)In this study, five of 26 patients complained of adverse reactions. The distribution of side effects in this study was similar to those of other studies.
4)9)Two patients with he- adaches and nausea after using aerosolized budesonide showed better compliance with budesonide powder. The presence of adverse reactions might be one of the important determining factors in choosing between the two delivery systems.
In terms of efficacy and side effects, there are no significant differences between the two types of delivery systems. Given
the awareness of environmental hazards and restrictions on the use of freon-propelled aerosols, budesonide powder can be a therapeutic alternative to aerosolized budesonide. Budesonide powder can be used with prior use of a topical decongestant, and freon-propelled aerosol can induce an environmental ha- zard.
In conclusion, this study demonstrates that both aerosolized budesonide and budesonide powder are effective in reducing the symptoms of perennial allergic rhinitis and that there are no significant differences of efficacy, side effects and prefer- ence between the two delivery systems.
REFERENCES
1) Balle VH. The effect of budesonide in perennial rhinitis. Eur J Respir Dis 1982;63:197-204.
2) Malm L, Whil JA, Lamm CJ, et al. Reduction of methacholine- induced nasal secretion by treatment with a new topical steroid in perennial non-allergic rhinitis. Allergy 1981;36:209-14.
3) Viner AS, Jackman N. Retrospective survey of 1271 patients dia- gnosed as perennial rhinitis. Clin Allergy 1976;6:251-9.
4) Juniper EF, Guyatt GH, Andersson B, Ferrie PJ. Comparison of powder and aerosolized budesonide in perennial rhinitis: validation of rhinitis quality of life questionaire. Ann Allergy 1993;70:225-30.
5) Adamopoulos G, Manolopoulos L, Giotakis I. A comparison of the efficacy and patient acceptability of budesonide and beclometha- sone dipropionate aqueous nasal sprays in patients with perennial rhinitis. Clin Otolaryngol 1995;20:340-4.
6) Basran GS, McGivern DV, Hanley S, Davies D. The efficacy of budesonide and beclomethasone dipropionate, delivered via a pre- ssurized metered dose inhaler, in the treatment of perennial rhin- itis: a randomized, double-blind, crossover study. Am J Rhinol 1995;9:285-90.
7) McArthur JG. A comparison of budesonide and beclomethasone dipropionate sprays in the treatment of seasonal allergic rhinitis.
Clin Otolaryngol 1994;19:537-42.
8) Fisher WG. Comparison of budesonide and disodium cromogly- cate in the treatment of seasonal allergic rhinitis in children. Ann Allergy 1994;73(12):515-20.
9) Day JH, Andersson B, Briscoe MP. Efficacy and safety of intrana- sal budesonide in the treatment of perennial rhinitis in adults and children. Ann Allergy 1981;36:209-14.
10) Pipkorn U., Pukander J., Suonpaa J, et al. Long-term safety of bu- desonide nasal aerosol: a 5.5 year follow-up study. Clin Allergy 1988;18:253-9.