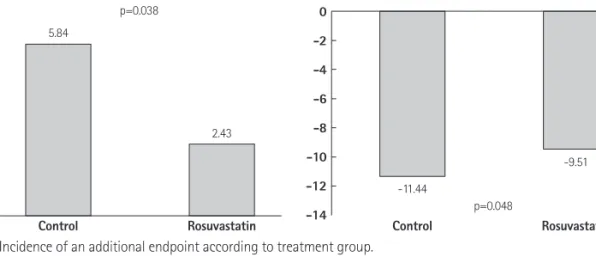
Effect of High Dose Rosuvastatin Loading before Percutaneous Coronary Intervention on Contrast-Induced Nephropathy
6
0
0
전체 글
(2)
(3)
(4)
(5)
(6)
수치

관련 문서
Contrast-induced nephropathy (CIN) is a common complication of primary percutaneous coronary intervention (pPCI) and is associated with high mortality and morbidity, long
Purpose: The optimum loading dose of clopidogrel has not been established in Asian patients with ST-segment elevation myocardial infarction (STEMI) under- going primary
This study aimed to evaluate the effects of percutaneous coronary intervention (PCI) on short- and long-term major adverse cardiac events (MACE) in elderly ( > 75 yr old) acute
It is uncertain that atorvastatin pretreatment can reduce myocardial damage in patients undergoing primary percutaneous coronary intervention (PCI) for ST-segment elevation
