INTRODUCTION
Congenital mesoblastic nephroma (CMN) is the most com- mon renal solid tumor of the newborn period (1). CMN occurs in two forms: a typical or leiomyomatous benign type seen almost exclusively in infants under the age of three months and an atypical or cellular type usually seen in older children, but also occurring in infants. The latter type is potentially malignant and capable of recurrence and metastasis (2). Mixed forms with a combination of the two patterns have also been reported (3). CMN is associated with polyhydramnios in most cases, and surgical excision is almost always curative (4-8).
Although CMN has a good prognosis, rare cases of CMN that show oligohydramnios resulting from fetal renal failure may be difficult to diagnose accurately and such patients have a poor prognosis due to the destruction of homeostasis. We report a case of a congenital mesoblastic nephroma that pre- sented with oligohydramnios, which was detected by ultra- sonography in the prenatal period. Early and accurate prena- tal diagnosis of a renal tumor may improve the outcome of affected pregnancies by allowing for prompt implementa- tion of the best strategy for prenatal management and deliv- ery (9). The differential diagnosis of mesoblastic nephroma includes hydronephrosis, focal renal dysplasia, multicystic dysplastic kidney, malignant nephroblastoma, Wilms’ tumor, diffuse nephroblastomatosis, and infantile polycystic kidney disease (4, 5, 10-12). Accurate prenatal ultrasonography can
give diagnostic information useful for the detection of CMN.
CASE REPORT
A 28-yr old woman, gravida 2, para 1, was referred to our hospital at 34 weeks of gestation for oligohydramnios and a fetal abdominal mass detected by ultrasonography. An earli- er delivery had been performed by cesarean section, due to breech presentation. The results of routine pregnancy tests (CBC, U/A, viral marker, Toxoplasma, and others) were non- specific and the triple test indicated that the patient was not at high risk. At 24 weeks of gestation, ultrasonographic find- ings showed a fetal weight (650 g) appropriate for the men- strual dates, no fetal abnormality, and adequate amniotic fluid.
After the checkup, the patient did not receive antenatal care for two months. At 33 weeks of gestation, the patient returned to the local clinic where a fetal abdominal mass and a low level of amniotic fluid were noted. The fetus was suspected the intrauterine growth restriction (1,440 g, below 10% of 33 weeks of gestation), and the patient was referred to our hospital. On admission, her vital signs were as follows; tem- perature 36.0℃, pulse rate 84/min, respiration rate 20/min, and blood pressure 120/80 mmHg. Laboratory findings were not remarkable. An indicated sonography (using Aloka SSD- 5000) was performed. The amniotic fluid index was almost zero. A huge (8.1×5.0×7.7 cm), well-encapsulated, abdo-
Cheol Hong Kim, Yoon Ha Kim, Moon Kyoung Cho, Ki Min Kim, Jin A Ha, Eun Hyun Joo*, Seok Mo Kim, Tae-Bok Song
Department of Obstetrics and Gynecology, Chonnam National University Medical School, Gwangju;
Department of Obstetrics and Gynecology*, Chonnam Hospital, Yeosu, Korea
Address for correspondence Yoon Ha Kim, M.D.
Department of Obstetrics and Gynecology, Chonnam National University, College of Medicine, 8 Hak-dong, Dong-gu, Gwangju 501-190, Korea
Tel : +82.62-220-6375, Fax : +82.62-227-1637 E-mail : [email protected]
357 J Korean Med Sci 2007; 22: 357-61
ISSN 1011-8934
Copyright � The Korean Academy of Medical Sciences
A Case of Fetal Congenital Mesoblastic Nephroma with Oligohydramnios
Although congenital renal tumors are rare, congenital mesoblastic nephroma (CMN) is the most common renal tumor in early infancy. It is non-metastatic, well differen- tiated, amenable to surgical removal, and carries a good prognosis. Polyhydram- nios has been detected in most of the published cases of CMN. However, we experienced a rare case of fetal CMN associated with oligohydramnios. A 28-yr old woman at 34 weeks of gestation was referred to our hospital for oligohydramnios and a fetal abdominal mass. An ultrasonography revealed a huge, well-encapsu- lated mass arising from the right kidney. An emergency cesarean section was per- formed due to fetal distress. After birth, despite intensive neonatal care, the baby died because of renal failure, disseminated intravascular coagulopathy, pulmonary edema, together with other problems
Key Words : Oligohydramnios; Congenital Mesoblastic Nephroma; Renal Failure
Received : 9 September 2005 Accepted : 14 December 2005
minal mass was detected, which was composed of both solid and multiple cystic components (Fig. 1). The tumor arose from the right fetal kidney, while the left kidney and other fetal organs were normal. Upon fetal heart rate monitoring, repeated severe variable deceleration was noted, and an emer- gency cesarean section was performed. A female neonate
weighing 1,750 g, with Apgar scores of 5 at 1 min and 9 at 5 min, was delivered. The pH value of umbilical arterial blood was 7.319.
On admission to the neonatal intensive care unit, the vital signs of the neonate were as follows; temperature 36.5℃, pulse rate 138/min, respiration rate 62/min, and blood pressure 69/43 mmHg. On physical examination, the infant showed a remarkable abdominal mass 8 cm in diameter in the right side of the abdomen. The mass was almost occupying the ab- dominal cavity. The infant also had clubbed feet. Ultrasono- graphic examination (using GE Logiq 9) and computed tomo- graphy scan of the abdomen revealed a well circumscribed, heterogeneous, non-enhanced mass 7 cm in diameter, origi- nating from the right kidney, which showed both necrotic and cystic components. The left kidney was normal (Fig. 2, 3). Within 24 hr of birth, the infant developed anuria, severe anemia, hypoglycemia, and hypoalbuminemia. Prothrombin time and activated prothrombin time were both prolonged.
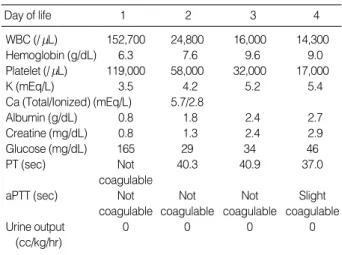
Despite intensive treatment, no urine was ever excreted and both generalized and pulmonary edema developed. On the second day, gastrointestinal hemorrhage and hypotension developed. The infant was resuscitated and intubated. Due to the simultaneous presence of several severe systemic con- ditions, radical nephrectomy could not be performed. The laboratory findings showed general deterioration. Renal fail- ure developed and hyperkalemia, hypoglycemia, thrombocy- topenia, anemia, and poor coagulation profiles (aPTT unde- tectably prolonged) could not be corrected despite major ther- apeutic interventions. (Table 1). The infant died at four days of age, owing to respiratory failure and disseminated intravas- cular coagulopathy.
Fig. 3.Contrast-enhanced CT of right renal tumor. The CT scan shows a well circumscribed, heterogeneous, non-enhanced mass with dimensions 7.5×5.0×7.4 cm, developed from the right kid- ney, with both necrotic and cystic components (white arrow). The left kidney was normal (black arrow).
Fig. 1.Prenatal ultrasound reveals a well-encapsulated abdomi- nal mass with dimensions 8.1×5.0×7.7 cm.
Fig. 2.Postnatal ultrasound reveals a huge, well circumscribed, echocomplex mass, possibly arising from the right kidney.
Fetal Congenital Mesoblastic Nephroma 359
Autopsy was performed and revealed an encapsulated mass, with dimensions 8.5×8.0×5.0 cm arising from the right renal pelvis. Cystic hemorrhage was observed (Fig. 4). On the side of the mass, a remnant of the kidney, with dimen- sions 2.0×0.8×2.0 cm, was seen. On cross section, the mass was yellow to pink in color, and lobulated. The left kidney and both lungs were normal. Microscopically, the tumor was classified as a cellular mesoblastic nephroma (Fig. 5). The neonate’s karyotype was normal (46, XX).
DISCUSSION
CMN is the most common renal tumor in infancy, account- ing for 3-6% of all childhood renal masses and 50% of all solid tumors in the neonatal period (13). Current opinion favors the classification of mesoblastic nephroma as a distinct, and usually benign neoplasm, arising from the renal paren- chyma (14). There appears to be a higher incidence of preterm labor and premature rupture of membranes in pregnancies complicated by CMN, as a result of associated polyhydram- nios (4, 15). However, the mechanism of polyhydramnios is unclear (16). Postulated mechanisms include a decreased gas- trointestinal uptake due to compression by the lesion and increased renal perfusion resulting in increased urine produc- tion. Another mechanism, hypercalcemia induced polyuria of the fetus, has been reported secondary to the tumor secretion of prostaglandin. Hypercalcemias have been reported to be caused by the tumor secretion of prostaglandin. Hyperten- sion may also occur and may be caused by entrapment of renal parenchyma by invading fibrous strands at the edge of the tumor with resultant renin hypersecretion (2).
Pathologically, the tumor has two patterns. The classical pattern of CMN is a moderate cellular proliferation of thick interlacing bundles of spindle cells, with elongated nuclei, which usually infiltrate into the renal and perirenal tissues.
Mitotic figures are present usually in the range of 0 to 1 per 10 high power fields (17). The other pattern, termed cellular
mesoblastic nephroma, is more common, and consists of den- sely cellular proliferation of polygonal cells with mitotic fig- ures in the range of 8 to 30 per 10 high power fields (17).
Cysts are common in this pattern.
Sonographically, mesoblastic nephroma may present as a large (4 to 8 cm), unilateral renal mass with nodular densi- ties, or as diffuse renal enlargement. These tumors are pre- dominantly solid, but cystic areas are occasionally seen (18).
Unlike Wilms’ tumor, there is no well-defined capsule, most likely due to hemorrhage with subsequent cystic degenera- tion (19). Patients suffering from CMN may show abnormali- ties in systems not closely associated with the tumor. Such abnormalities may include neuroblastoma (20), central ner- vous system defects (5, 20), genitourinary problems, gastroin- testinal difficulties, and limb abnormalities (5). Radical resec- tion of the tumor is the treatment of choice, which is usually curative (15). However, a small percentage of patients with these tumors experience local recurrence or distant metastasis due to inadequate resection (21) or cellular or atypical CMN, which is potentially a malignant tumor (3, 22). No familial or exogenous factors have been correlated to CMN occurrence, in contrast to the development of Wilms’ tumor, for exam- ple, where a familial link has been noted. There is no known predisposition to its occurrence in siblings born to the same mother after the birth of an affected infant. The condition is not associated with other karyotypic abnormalities (15). Cyto- genetic abnormalities such as trisomy 11 occur sporadically (23, 24). However, Fuchs et al. reported a case of CMN occur- ring in two siblings within one family and suggested that a second-trimester anomaly scan with targeted examination of the kidneys is warranted in families with a child affected by CMN (25).
In our case, the pregnant patient presented with oligohy- dramnios, and the neonate showed anuria, hypotension, hy- perkalemia, abnormal coagulation profiles, disseminated intravascular coagulopathy, and other pathologic findings.
An associated anomaly noted was clubbed feet. On autopsy,
Day of life 1 2 3 4
WBC (/ L) 152,700 24,800 16,000 14,300
Hemoglobin (g/dL) 6.3 7.6 9.6 9.0
Platelet (/ L) 119,000 58,000 32,000 17,000
K (mEq/L) 3.5 4.2 5.2 5.4
Ca (Total/Ionized) (mEq/L) 5.7/2.8
Albumin (g/dL) 0.8 1.8 2.4 2.7
Creatine (mg/dL) 0.8 1.3 2.4 2.9
Glucose (mg/dL) 165 29 34 46
PT (sec) Not 40.3 40.9 37.0
coagulable
aPTT (sec) Not Not Not Slight
coagulable coagulable coagulable coagulable
Urine output 0 0 0 0
(cc/kg/hr)
Table 1.The serial laboratory findings of the neonate
Fig. 4.Gross photograph shows the encapsulated mass with di- mensions 8.5×8.0×5.0 cm arising from the right renal pelvis.
the tumor was shown to be a cellular mesoblastic nephroma with mitotic figures more than 8 per 10 high power fields.
Areas of coagulative necrosis and hemorrhage were also ob- served.
According to the literature, polyhydramnios was observed in almost 40% of the CMN cases (20), and acute fetal distress occurred in 25% of fetuses with CMN (26). Even though it is important to note the high incidence of polyhydramnios (24), CMN can also be accompanied by oligohydramnios, which heralds a poor prognosis. Careful, continuous obser- vation of the fetus should be considered when a renal tumor is diagnosed on routine prenatal ultrasound, and close ultra- sound follow-up and maternal-fetal monitoring should be performed to detect any fetal complications.
REFERENCES
1. Bolande RP. Congenital and infantile neoplasia of the kidney. Lancet 1974; 2: 1497-9.
2. Broecker B. Non-Wilms’ renal tumors in children. Urol Clin North Am 2000; 27: 463-9.
3. Bisceglia M, Carosi I, Vario M, Zaffarano L, Creti G. Congenital mesoblastic nephroma: report of a case with review of the most sig- nificant literature. Pathol Res Pract 2000; 196: 199-204.
4. Giulian BB. Prenatal ultrasonographic diagnosis of fetal renal tu- mors. Radiology 1984; 152: 69-70.
5. Walter JP, McGahan JP. Mesoblastic nephroma: prenatal sonogra- phic detection. J Clin Ultrasound 1985; 13: 686-9.
6. Howey DD, Farrell EE, Sholl J, Goldschmidt R, Sherman J, Hage- Fig. 5.(A) The section revealed a well-defined cellular mass (He- matoxylin-eosin stain,×40). (B) The tumor showed proliferation of spindle cells with short-elongated nuclei with necrosis and numer- ous mitotic figures (inset) (Hematoxylin-eosin stain, ×200). (C) In some areas, the tumor cells were haphazardly arranged. Entrapped immature glomeruli were often present in the tumor (Hematoxylin- eosin stain, ×200).
A B
C
man JR. Congenital mesoblastic nephroma: prenatal ultrasonic find- ings and surgical excision in a very-low-birth-weight infant. J Clin Ultrasound 1985; 13: 506-8.
7. Geirsson RT, Ricketts NE, Taylor DJ, Coghill S. Prenatal appear- ance of a mesoblastic nephroma associated with polyhydramnios. J Clin Ultrasound 1985; 13: 488-90.
8. Ohmichi M, Tasaka K, Sugita N, Kamata S, Hasegawa T, Tanizawa O. Hydramnios associated with congenital mesoblastic nephroma:
a case report. Obstet Gynecol 1989; 74: 469-71.
9. Goldstein I, Shoshani G, Ben-Harus E, Sujov P. Prenatal diagnosis of congenital mesoblastic nephroma. Ultrasound Obstet Gynecol 2002; 19: 209-11.
10. Gordillo R, Vilaro M, Sherman NH, Phillips M, Hoyer JR, Rosen- berg HK. Circumscribe- d renal mass in dysplastic kidney. J Ultra- sound Med 1987; 6: 613-7.
11. Ambrosino MM, Hernanz-Schulman M, Horii SC, Raghavendra BN, Genieser NB. Prenatal diagnosis of nephroblastomatosis in two sib- lings. J Ultrasound Med 1990; 9: 49-51.
12. Rempen A, Kirchner T, Frauendienst-Egger G, Hocht B. Congeni- tal mesoblastic nephroma. Fetus 1992; 2: 1-5.
13. Campagnola S, Fasoli L, Flessati P, Sulpasso M, Balter R, Pea M, Caudana R. Congenital cystic mesoblastic nephroma. Urol Int 1998;
61: 254-6.
14. Diana W, Timothy M, Mary E. Fetology: diagnosis and management of the fetal patient 2000; 849-52.
15. Haddad B, Haziza J, Touboul C, Abdellilah M, Uzan S, Paniel BJ.
The congenital mesoblastic nephroma: a case report of prenatal diag- nosis. Fetal Diagn Ther 1996; 11: 61-6.
16. Shibahara H, Mitsuo M, Fujimoto K. Prenatal sonographic diagno- sis of a fetal renal mesoblastic nephroma occuring after transfer of a cryopreserved embryo. Hum Reprod 1999; 14: 1324-7.
17. Pettinato G, Manivel JC, Wick MR, Dehner LP. Classical and cel- lular (atypical) congenital mesoblastic nephroma:a clinicopatholog- ic, ultrastructual, immunohisto-chemical, and flow cytometric study, Hum Pathol 1989; 20: 682-90.
18. Ehman RL, Nicholson SF, Machin GA. Prenatal sonographic detec- tion of congenital mesoblastic nephroma in a monozygotic twin preg- nancy. J Ultrasound Med 1983; 2: 555-7.
19. Slasky BS, Penkrot RJ, Bron KM. Cystic mesoblastic nephroma. Urol- ogy 1982; 19: 220-3.
20. Blank E, Neerhout RC, Burry KA. Congenital mesoblastic nephro- ma and polyhydramni- os. JAMA 1978; 240: 1504-5.
21. Bechwith JB, Weeks DA. Congenital mesoblastic nephroma: when should we worry? Arch Pathol Lab Med 1986; 110: 98-9.
22. Joshi VV, Kasznicka J, Walters TR. Atypical mesoblastic nephroma.
Arch Pathol Lab Med 1986; 110: 100-6.
23. Speleman F, van den Berg E, Dhooge C. Cytogenetic and molecu- lar analysis of cellular atypical mesoblastic nephroma. Genes Chro- mosomes Cancer 1998; 21: 265-9.
24. Cin DP, Lipcsei G, Hermand G, Boniver J, van den Berghe H. Con- genital mesoblastic nephroma and trisomy 11. Cancer Genet Cyto- genet 1998; 103: 68-70.
25. Fuchs IB, Henrich W, Brauer M, Stover B, Guschmann M, Degen- hardt P, Dudenhausen JW. Prenatal diagnosis of congenital meso- blastic nephroma in 2 siglings. J Ultrasound Med 2003; 22: 823-7.
26. Leclair MD, El-Ghoneimi A, Audry G, Ravasse P, Moscovici J, He- loury Y. The outcome of prenatally diagnosed renal tumors. J Urol 2005; 173: 186-9.
27. Matsumura M, Nishi T, Sasaki Y, Yamada R, Yamamoto H, Ohhama Y, Tanaka Y, Kurosu F, Amano K. Prenatal diagnosis and treatment strategy for congenital mesoblastic nephroma. J Pediatr Surg 1993;
28: 1607-9.
Fetal Congenital Mesoblastic Nephroma 361