서 론
대사증후군은 나이, 흡연, 신체활동, 비만, 이상지혈증, 고혈압, 고 혈당 등과 같은 이미 밝혀져 있는 심혈관 질환 및 당뇨병의 위험요인 들이 서로 군집을 이루는 현상을 한 가지 질환군으로 개념화시킨 것 으로, 이후 여러 기관에서 독립적인 진단기준들이 만들어져 향후 심
혈관 질환 및 당뇨병 발생이 높은 위험군을 예측하는 데 유용한 지 표로 사용되어 오고 있다.1,2) 또한 심혈관계 질환 이환율과 심혈관계 질환으로 인한 사망률 및 모든 원인에 의한 사망률을 증가시키며, 인 슐린 저항성을 대표하기 때문에 당뇨병의 발병 위험을 증가시킨 다.3,4) 최근 대사증후군은 전 세계적으로 증가 추세를 보이고 있으 며,5,6) 우리나라 역시 Lim 등7)의 연구 결과에 따르면 1998년부터 2007
Original Article
대사증후군 구성 요인별 당뇨병 발생 예측도 비교:
전국적인 인구 기반 후향적 코호트 연구
상정은
1, 이종은
1, 최준석
1, 허 연
1, 남효윤
1, 남가은
1, 김도훈
1,*, 한경도
21고려대학교안산병원 가정의학과, 2가톨릭대학교 의과대학 의생명과학교실
A Comparison of Predictability of Physician-Diagnosed Diabetes according to Metabolic Syndrome Components: A Nationwide Population-Based Retrospective Cohort Study
Jung-Eun Sang
1, Jong-Eun Lee
1, Jun-Seok Choi
1, Youn Huh
1, Hyo-Yun Nam
1, Ga-Eun Nam
1, Do-Hoon Kim
1,*, Kyung-Do Han
21Department of Family Medicine, Korea University Ansan Hospital, Ansan; 2Department of Medical Lifescience, School of Medicine, The Catholic University of Korea, Seoul, Korea
Background: Metabolic syndrome is associated with an increased risk of cardiovascular disease and diabetes. However, in Korea, the association between metabolic syndrome components and diabetes has been examined only by cross-sectional survey. This study aimed to identify the association between metabolic syndrome components and risk of developing diabetes of diabetes in the National Health Insurance Service- National Sample Cohort (NHIS-NSC).
Methods: Data were obtained from the NHIS-NSC between 2010 and 2013. Out of a total of 211,541 eligible individuals, the following were excluded:
25,133 under the age of 30 years; 180 with incomplete information; and 19 with diabetes at baseline. Finally, 166,257 subjects were included in the study. Statistical analysis was performed using the independent t-test and chi-square test. The association between metabolic syndrome and the risk of developing diabetes was estimated by using Cox multivariable regression analysis.
Results: During the follow-up, 4,405 were diagnosed with diabetes among total 166,257 participants.
Conclusion: Metabolic syndrome as well as the individual components is associated with an increased risk of diabetes after adjusting for age and sex, body mass index, smoking status, alcohol intake, and physical activity. During the 4-year follow up, the risk for incident rate of diabetes increased with the number of metabolic syndrome components. It has been also suggested that the metabolic syndrome component most strongly associated with incident diabetes was high fasting blood glucose.
Keywords: Metabolic Syndrome X; Diabetes Mellitus; Impaired Fasting Glucose; National Health Insurance Service-National Sample Cohort
https://doi.org/10.21215/kjfp.2017.7.1.110eISSN 2233-9116
Korean J Fam Pract. 2017;7(1):110-115
KJFP
Korean Journal of Family PracticeReceived March 15, 2016 Revised June 25, 2016 Accepted July 22, 2016 Corresponding author Do-Hoon Kim
Tel: +82-31-412-5360, Fax: +82-31-412-7657 E-mail: [email protected]
Copyright © 2017 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons At- tribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
상정은 외. 대사증후군 구성 요인별 당뇨병 발생 예측도 비교 Korean Journal of Family Practice
KJFP
Original Article
Korean Journal of Family Practice 년까지 우리나라 국민건강영양조사 자료를 이용한 대사증후군의
유병률을 살펴본 결과 24.9%에서 31.3%로 증가하였다. 이러한 대사 증후군 유병률의 증가는 대사증후군 각각의 구성요인의 증가로 인 한 것으로 생각되며, 최근 서구화된 식습관 및 생활습관에 의한 변 화로 다섯 가지 구성요인 중 저고밀도지단백 콜레스테롤혈증, 복부 비만, 고중성지방혈증 순으로 증가하는 경향을 보였다.7)
대사증후군은 당뇨병과 심혈관 질환의 예측인자로 알려져 있으 며, 서구의 경우 대규모의 다양한 인종이 포함된 인구집단을 이용한 여러 코호트 연구에서 대사증후군과 당뇨병의 연관성을 입증하였
다.8-11) Ballantyne 등11)의 미국인을 대상으로 한 대규모 연구에 따르면
대사증후군 각각의 항목뿐만 아니라 대사증후군은 당뇨병 발생의 예측인자임을 확인할 수 있었고, Lorenzo 등9)의 연구에서는 National Cholesterol Education Program Adult Treatment Panel III (NCEP-ATP III) 가 World Health Organization (WHO) 정의보다 더 높은 민감도를 보였으나 이 두 진단기준 모두 당뇨병의 독립적인 예측인자로 나타 났다. 우리나라에서도 Hwang 등12)의 연구에서 2,435명의 당뇨병을 진단 받지 않은 사람을 8.7년간 추적 관찰한 결과 대사증후군은 당 뇨병과 중요한 연관성을 갖고 있는 것을 확인할 수 있었다. 현재까지 우리나라에서는 대사증후군 구성요인과 당뇨병에 대한 연구들 대 부분이 유병률과 관련된 단면연구를 통한 분석이었고, 코호트 연구 가 없었다.
따라서 본 연구에서는 전 국민을 대표하는 국민건강보험공단 표 본자료를 이용한 대사증후군 및 각각의 구성요인과 당뇨병 발생과 의 연관성에 대하여 다루고자 한다.
방 법
1. 자료원 및 연구대상자
국민건강보험공단은 1963년 의료보험법 제정에 의해 시작된 이래 로 1977년 500인 이상 사업자 근로자 의료보험 실시를 시작으로 1989년에는 전국민 의료보험 실현과 함께 2000년에 국민건강보험공 단 출범으로 의료보험의 완전 통합이 이루어지게 되었다. 현재 국민 건강보험 공단은 전 국민의 자격 및 보험료, 건강검진결과, 진료내역, 암 및 희귀난치성질환자 등록정보 등의 방대한 빅데이터인 국민건 강정보를 유지 및 관리하고 있다. 또한 건강보험가입자의 건강을 유 지 및 증진하고, 나아가 보험급여비를 줄이고 일반건강검진, 암검진, 생애전환기 건강진단 및 영유아 건강검진을 통하여 평생 건강관리 체계를 구축하고 있다.
건강보험공단자료는 방대한 자료규모와 개인정보보호 문제 등을 개선하고자 전 국민의 2%인 약 100만 명을 표본 추출하여 2002년을
기준으로 2013년까지 동일 대상자의 자료를 12년간 관찰한 자료이다.
이는 건강보험가입자 및 의료급여수급권자(외국인 제외)를 대상으 로 연령, 성, 지역, 가입자 구분, 소득분위 등 대상자의 사회경제적 변 수 및 장애, 사망관련 총 14개의 변수 및 사회∙경제적 자격변수(장애 및 사망포함), 의료이용(명세서, 진료내역, 상병내역, 처방전 교부상 세내역 및 건강검진) 현황, 요양기관 현황 등의 내용으로 구성되어 있다.13) 본 연구에서는 국민건강보험공단의 표본 코호트 자료를 사 용하였고 2010년 1월부터 2013년 12월까지 4년간 1차 일반건강검진 및 생애전환기건강진단을 받은 2009년 수진자 211,541명을 대상으로 하였다. 이 중 30대 미만 25,133명, 결측 180명, 검진 전 당뇨병을 진단 받은 19,971명은 제외되어 총 166,257명이 분석 대상자로 선정되었다.
본 연구는 고려대학교 안산병원 연구윤리심의위원회가 심의 및 승 인하였다(AS15213).
2. 대사증후군과 당뇨병의 정의
대사증후군은 NCEP-ATP III 진단기준 및 복부둘레의 경우 WHO 의 서태평양지역 기준을 적용하였으며, 구성인자로는 1) 복부비만:
허리둘레 남자 >90 cm, 여자> 80 cm, 2) 고중성지방혈증: 중성지방
≥150 mg/dL, 3) 저고밀도지단백 콜레스테롤혈증: 고밀도지단백 콜레 스테롤 남자 <40 mg/dL, 여자 <50mg/dL, 4) 고혈압: 혈압 ≥130/85 mmHg, 5) 공복고혈당: 공복혈당 ≥100 mg/dL이며, 상위 5개 항목 중 3 개 항목 이상 만족할 경우 대사증후군으로 진단하였다.14)
당뇨병은 2010년 1월 1일부터 2013년 12월 31일까지 4년간의 관찰 기간 동안 International Classification of Diseases (ICD) 10; E11-14인 제 2형 당뇨병만을 포함하였으며, 당뇨병 진단과 함께 인슐린을 포함한 약물처방을 받은 사람을 기준으로 당뇨병의 발생을 확인하였다.
3. 관련 변수 정의
인구사회학 변수인 흡연상태는 평생 총 5갑(100개비) 이상의 담배 를 피운 적이 없는 비흡연자, 평생 총 5갑(100개비) 이상의 담배를 피 운 적이 있으나 현재는 흡연하지 않는 과거 흡연자, 평생 총 5갑(100 개비) 이상의 담배를 피운 적이 있으며 현재도 흡연 중인 현재 흡연 자인 세 군으로 나누었다. 음주습관은 음주 관련 문진 문항에서 음 주일수와 잔 수를 모두 응답한 자로 음주의 여부에 따라 구분하였 으며, 신체활동은 신체활동실천율로 1주일 동안 걷기, 중등도 활동, 격렬한 활동을 실천한 일수에 대한 비율로 가벼운 운동, 출퇴근이나 여가 시간에 걷기를 포함한 하루 30분 이상 걷기, 빠르게 걷기, 복식 테니스 하기, 보통 속도로 자전거 타기, 엎드려 걸레질하기 등 하루 30분 이상 중등도 활동 및 달리기, 에어로빅, 빠른 속도로 자전거 타 기, 등산 등 하루 20분 이상 격렬한 활동으로 정의하였다.
Jung-Eun Sang, et al. Comparison of Predictability of Diabetes according to Metabolic Syndrome Components
Korean Journal of Family Practice
KJFP
신체계측은 체질량지수의 경우 전신의 비만 정도를 체중(kg)을 신장(m)의 제곱으로 나누어 산출하였고, 복부비만은 허리둘레에 따라 남성 90 cm 미만, 여성 80 cm 미만 또는 이상인 경우로 양호 또 는 경계로 구분하였고 이외 체중, 수축기 혈압/이완기 혈압을 측정하 였으며, 검사는 혈청 검사를 통해 공복혈당, 혈청 총콜레스테롤, 고 밀도지단백 콜레스테롤, 저밀도지단백 콜레스테롤, 중성지방을 측 정하였다.
4. 통계분석
통계분석은 SAS Institute ver. 9.4 for Windows (SAS Institute, Cary, NC, USA)를 이용하였다. 당뇨병 발생을 추적 관찰하여 당뇨병이 발 생한 군과 발생하지 않은 군의 기초특성을 비교하였으며, 범주형의 경우 카이제곱 검정을 사용하였고, 연속형 범주의 경우 독립 t-검정 을 사용하였다. 대사증후군의 구성인자와 당뇨병 발생 위험과의 연 관성은 다중 콕스 회귀분석으로 인과관계를 확인하였다. 누적위험 함수비율(hazard ratio, HR)과 95% 신뢰구간(confidence interval, CI) 을 산출하였으며, 나이, 성별, 비만도, 음주, 흡연, 운동을 보정하였다.
통계적으로 유의한 수준은 P값이 0.05 미만인 경우로 하였다.
결 과
연구 대상자 총 166,257명 중 4년간 추적 관찰기간 동안 새롭게 당
뇨병 진단을 받은 사람은 4,405명(남자 2,459명, 여자 1,946명)이었다.
평균 연령은 57.9±11.7세, 체중 66.6±11.8 kg, 체질량지수 25.4±3.3 kg/
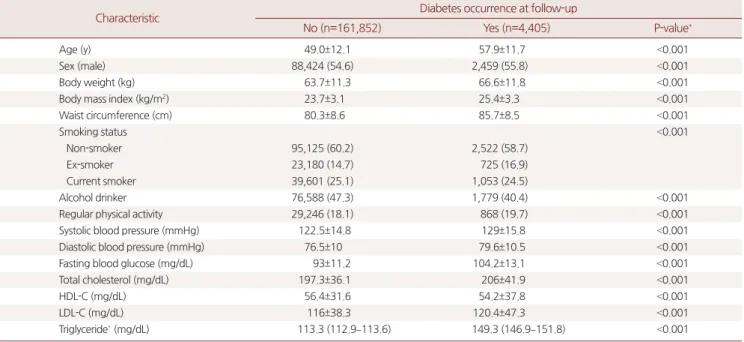
m2, 복부둘레 85.7±8.5 cm, 수축기 혈압 129±15.8 mmHg, 이완기 혈압 79.6±10.5 mmHg, 공복혈당 104.2±13.1 mg/dL, 혈청 총콜레스테롤 206±41.9 mg/dL, 혈청 고밀도지단백 콜레스테롤 54.2±37.8 mg/dL, 혈 청 저밀도지단백 콜레스테롤 120.4±47.3 mg/dL, 혈청 중성지방농도 149.3 mg/dL (146.9–151.8 mg/dL)로 나타났다. 또한 추적 관찰기간 동 안 당뇨병 진단을 받지 않은 사람은 161,852명(남자 88,424명, 여자 73,428명)이었으며, 평균연령은 49.0±12.1세, 체중 63.7±11.3 kg, 체질량 지수 23.7±3.1 kg/m2, 복부둘레 80.3±8.6 cm, 수축기 혈압 122.5±14.8 mmHg, 이완기 혈압 76.5±10 mmHg, 공복혈당 93±11.2 mg/dL, 혈청 총콜레스테롤 197.3±36.1 mg/dL, 혈청 고밀도지단백 콜레스테롤 56.4±31.6 mg/dL, 혈청 저밀도지단백 콜레스테롤 116±38.3 mg/dL, 혈 청 중성지방농도 113.3 mg/dL (112.9–113.6 mg/dL)로 나타났다. 당뇨병 을 진단 받지 않은 군과 진단 받은 군 모두 모든 항목에서 P값 0.001 미만으로 유의한 결과를 보였다(Table 1).
대사증후군의 구성인자들에서 당뇨병 발생을 비교하였을 때, 비 당뇨군 발생군과 당뇨병 발생군 각각에서 복부둘레에서는 42,979명 (26.6%), 2,292명(52%), 고저밀도지단백 콜레스테롤혈증에서는 43,347 명(26.8%), 2,066명(46.9%), 고혈압에서는 70,253명(43.4%), 3,012명 (68.4%), 공복고혈당에서는 41,704명(25.8%), 2,825명(64.1%), 고중성지 방혈증 55,456명(34.3%), 2,639명(59.9%)으로 나타났으며, 대사증후군
Table 1. Baseline characteristic of subjects according to the occurrence of diabetes at follow up
Characteristic Diabetes occurrence at follow-up
No (n=161,852) Yes (n=4,405) P-value*
Age (y) 49.0±12.1 57.9±11.7 <0.001
Sex (male) 88,424 (54.6) 2,459 (55.8) <0.001
Body weight (kg) 63.7±11.3 66.6±11.8 <0.001
Body mass index (kg/m2) 23.7±3.1 25.4±3.3 <0.001
Waist circumference (cm) 80.3±8.6 85.7±8.5 <0.001
Smoking status <0.001
Non-smoker 95,125 (60.2) 2,522 (58.7)
Ex-smoker 23,180 (14.7) 725 (16.9)
Current smoker 39,601 (25.1) 1,053 (24.5)
Alcohol drinker 76,588 (47.3) 1,779 (40.4) <0.001
Regular physical activity 29,246 (18.1) 868 (19.7) <0.001
Systolic blood pressure (mmHg) 122.5±14.8 129±15.8 <0.001
Diastolic blood pressure (mmHg) 76.5±10 79.6±10.5 <0.001
Fasting blood glucose (mg/dL) 93±11.2 104.2±13.1 <0.001
Total cholesterol (mg/dL) 197.3±36.1 206±41.9 <0.001
HDL-C (mg/dL) 56.4±31.6 54.2±37.8 <0.001
LDL-C (mg/dL) 116±38.3 120.4±47.3 <0.001
Triglyceride† (mg/dL) 113.3 (112.9–113.6) 149.3 (146.9–151.8) <0.001
Values are presented as mean±standard deviation for continuous variables, number (%) for categorical variables, or median (range).
HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol.
*P-values were obtained by using independent t-test for continuous variables or chi-square test for categorical variables. †Log transformation was performed for analyses.
상정은 외. 대사증후군 구성 요인별 당뇨병 발생 예측도 비교 Korean Journal of Family Practice
KJFP
을 진단 받은 사람에서는 38,452명(23.8%), 2,744명(62.3%)으로 나타났 다(Table 2).
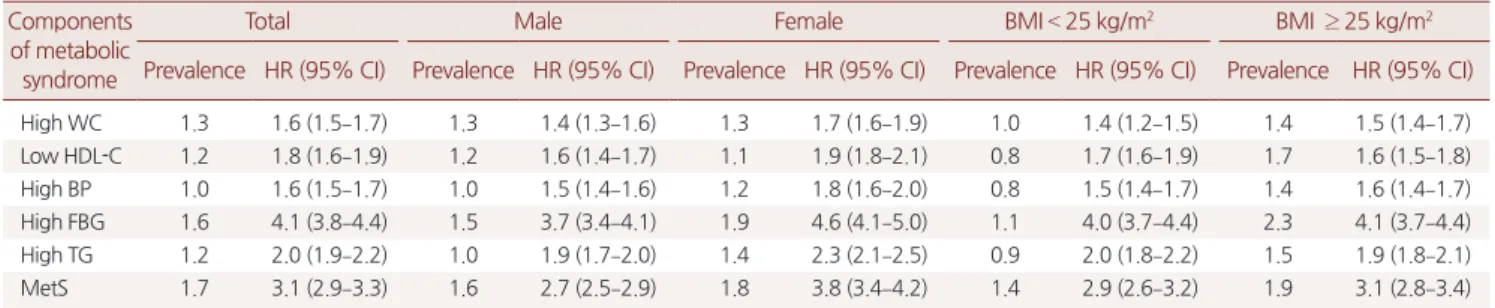
대사증후군의 구성요인들에 따른 1년간 100명 중 당뇨병 발생수 와 당뇨병 발생 위험도는 나이, 성별, 체질량지수, 음주 및 흡연, 신체 활동을 보정한 후에도 대사증후군의 구성요인들 모두 당뇨병 발생 수와 당뇨병 발생 위험을 증가시켰다(복부비만: prevalence 1.3, HR 1.6, 95% CI 1.5–1.7; 고저밀도지단백 콜레스테롤혈증: prevalence 1.2, HR 1.8, 95% CI 1.6–1.9; 고혈압: prevalence 1.0, HR 1.6, 95% CI 1.5–1.7;
공복고혈당: prevalence 1.6, HR 4.1, 95% CI 3.8–4.4; 고중성지방혈증:
prevalence 1.2, HR 2.0, 95% CI 1.9–2.2; 대사증후군: prevalence 1.7, HR 3.1, 95% CI 2.9–3.3). 또한 공복고혈당에 해당하는 군과 대사증후군 진단받은 군의 당뇨병 발생수와 당뇨병 발생 위험도를 비교하였을 때, 대사증후군을 진단받은 군에 비하여 공복고혈당에 해당하는 군이 성별이나 비만도와 관계없이 모두 당뇨병 발생의 위험이 더 높 은 것을 확인할 수 있었다. 성별 및 비만도에 따른 하위 그룹에서도
각각의 대사증후군 구성요인들은 당뇨병 발생 수와 발생의 위험을 높이는 것으로 나타났다(Table 3).
4년간 추적 관찰기간 동안 대사증후군의 구성요인들을 만족하는 항목수가 증가할수록 당뇨병 발생률이 증가하였다(Figure 1).
체질량지수와 대사증후군을 진단 받았는지에 따른 4개의 군으로 나누어 4년간의 추적 관찰기간 동안의 당뇨병 발생률을 비교하였을 때, 대사증후군을 진단받은 비만인 군, 대사증후군을 진단받지 않 은 비만인 군, 대사증후군을 진단받은 정상체중인 군, 대사증후군 을 진단받지 않은 정상체중인 군 순으로 당뇨병 발생률이 증가하였 다(Figure 2).
고 찰
대사증후군은 전 세계적으로 증가하고 있으며, 당뇨병 및 심혈관
Table 2. Comparison of occurrence rate of diabetes according to com- ponents of metabolic syndrome at baseline
Components of metabolic syndrome
Diabetes
No Yes P-value*
High WC 42,979 (26.6) 2,292 (52.0) <0.001
Low HDL-C 43,347 (26.8) 2,066 (46.9) <0.001
High BP 70,253 (43.4) 3,012 (68.4) <0.001
High FBG 41,704 (25.8) 2,825 (64.1) <0.001
High TG 55,456 (34.3) 2,639 (59.9) <0.001
MetS 38,452 (23.8) 2,744 (62.3) <0.001
Values are presented as number (%).
High WC: WC ≥90 cm in men or ≥80 cm in women; low HDL-C: HDL-C <40 mg/dL in men or <50 mg/dL in women; high FBG: FBG ≥100 mg/dL: high BP:
BP >130/85 mmHg; high TG: TG ≥150 mg/dL.
WC, waist circumference; HDL-C, high density lipoprotein cholesterol; BP, blood pressure; FBG, fasting blood glucose; TG, triglyceride; MetS, metabolic syndrome.
*P-values were obtained by using chi-square test.
Table 3. Prevalence and HR (95% CI) of diabetes according to components of metabolic syndrome at baseline Components
of metabolic syndrome
Total Male Female BMI < 25 kg/m2 BMI ≥ 25 kg/m2
Prevalence HR (95% CI) Prevalence HR (95% CI) Prevalence HR (95% CI) Prevalence HR (95% CI) Prevalence HR (95% CI)
High WC 1.3 1.6 (1.5–1.7) 1.3 1.4 (1.3–1.6) 1.3 1.7 (1.6–1.9) 1.0 1.4 (1.2–1.5) 1.4 1.5 (1.4–1.7)
Low HDL-C 1.2 1.8 (1.6–1.9) 1.2 1.6 (1.4–1.7) 1.1 1.9 (1.8–2.1) 0.8 1.7 (1.6–1.9) 1.7 1.6 (1.5–1.8)
High BP 1.0 1.6 (1.5–1.7) 1.0 1.5 (1.4–1.6) 1.2 1.8 (1.6–2.0) 0.8 1.5 (1.4–1.7) 1.4 1.6 (1.4–1.7)
High FBG 1.6 4.1 (3.8–4.4) 1.5 3.7 (3.4–4.1) 1.9 4.6 (4.1–5.0) 1.1 4.0 (3.7–4.4) 2.3 4.1 (3.7–4.4)
High TG 1.2 2.0 (1.9–2.2) 1.0 1.9 (1.7–2.0) 1.4 2.3 (2.1–2.5) 0.9 2.0 (1.8–2.2) 1.5 1.9 (1.8–2.1)
MetS 1.7 3.1 (2.9–3.3) 1.6 2.7 (2.5–2.9) 1.8 3.8 (3.4–4.2) 1.4 2.9 (2.6–3.2) 1.9 3.1 (2.8–3.4)
Values were calculated by using Cox multivariable regression analysis with adjustment for age, sex, body mass index, smoking status, alcohol intake, physical activity.
High WC: WC ≥90 cm in men or ≥80 cm in women; low HDL-C: HDL-C <40 mg/dL in men or <50 mg/dL in women; high FBG: FBG ≥100 mg/dL: high BP: BP >130/85 mmHg; high TG: TG ≥150 mg/dL; prevalence: the number of new cases of diabetes per 100 people during one year.
HR, hazard ratio; CI, confidence interval; BMI, body mass index; WC, waist circumference; HDL-C, high density lipoprotein cholesterol; BP, blood pressure; FBG, fasting blood glucose; TG, triglyceride; MetS, metabolic syndrome.
Theproportionofpeople withoutthediagnosisofdiabetes
0 1.0
0.9
4 Follow-up (y)
0.8
01 2 3
4
5
3 2
1
Figure 1. Comparison of occurrence rate of diabetes according to the number of metabolic syndrome components. Values were calculated by using Kaplan–Meier disease-free survival curves (P<0.001, log-rank test).
Jung-Eun Sang, et al. Comparison of Predictability of Diabetes according to Metabolic Syndrome Components
Korean Journal of Family Practice
KJFP
질환을 미리 예측할 수 있어 중요성이 대두되고 있다. 이번 연구는 전 국민의 대표성을 가진 국민건강보험자료를 이용한 대사증후군 의 구성요인과 당뇨병 발생위험의 연관성에 대한 첫 번째 연구로서 의미가 있다. 이전 외국의 연구들과 비교하여 우리나라의 특성을 알 아보고자 연구를 진행하였으나 결과는 대체적으로 외국의 연구들 과 비슷한 결과를 보였다.
첫 번째로 대사증후군이 당뇨병 발생위험을 증가시켰으며 만족 하는 대사증후군 구성요인의 개수가 증가할수록 당뇨병 발생위험 이 증가하였다. 이는 Klein 등15)의 연구에서도 대사증후군의 구성요 인을 만족하는 항목들이 증가할수록 당뇨병 발생률을 증가시켰으 며(odds ratio [OR] 33.67, 95% CI 7.93–142.96), 이 중 당뇨병과 가장 관 련이 높은 것은 공복고혈당이었다(age and sex adjusted OR 18.33, 95%
CI 12.15–27.67). 또한 각각의 구성요인 중 공복고혈당이 당뇨병의 발 생위험과 가장 연관성이 높았으며, 더구나 대사증후군을 만족하는 군보다도 당뇨병 발생 위험도가 더 높아 단일인자로 매우 중요하다 는 점이다. Wilson 등8)의 연구에서도 같은 결과를 보였고, 이것은 공 복고혈당이 인슐린 저항성과 관련이 있어 당뇨병 발생에 가장 큰 위 험인자임을 반영하며 당뇨병으로의 진행 10년 동안 50%의 위험성이 있는 당뇨 전 단계이기도 하다.
본 연구에서 특징적이었던 점은 대사증후군을 진단받은 정상체 중인 군보다 대사증후군을 진단받지 않은 비만인 군이 당뇨병 발생 률이 더 높았다. 이는 Katzmarzyk 등16)과 Hinnouho 등17)의 연구에서 모든 원인의 사망률과 심혈관 질환으로 인한 사망률이 대사증후군 을 진단받은 정상체중인 군보다 비만인 건강한 사람에서 더 높았던
것과 같은 결과를 보였다.
본 연구의 한계점으로는 4년이라는 추적관찰 기간이 짧다는 것이 며, 여러 기관에서 제시하는 대사증후군의 진단기준 중 NECP-ATP III 진단기준 하나만으로 연구를 진행하였기 때문에 다른 진단기준 에 따른 결과의 차이가 있을 것으로 생각된다. 그러나 Kim 등18)의 연 구에서는 2001년 국민건강영양조사 자료를 이용하여 20세 이상의 성인을 대상으로 한 연구에서 나이를 보정한 후 대사증후군과 고혈 압/당뇨병/심혈관 질환 또는 뇌졸중과의 연관성 차이에서 남녀 모두 에서 NCEP-ATP III 진단기준이 International Diabetes Federation (IDF) 진단기준보다 고혈압, 당뇨병과 더 연관성이 있다는 결과를 보 였다. 또한 이러한 한계점을 보안하고자 연령, 성별, 비만도, 음주/흡 연 및 신체활동 보정을 하였다.
본 연구의 의미로는 건강보험공단자료라는 대규모 자료를 이용한 대사증후군의 구성요인과 당뇨병 발생 위험의 연관성을 연구한 첫 연구로 성별이나 체질량지수로 나누어 하위그룹 분석을 실시하였으 며 연령, 성별, 체질량지수, 음주 및 흡연, 신체활동을 보정한 후에도 의미 있는 결과를 관찰하였다는 점이다.
결론적으로 대사증후군의 구성요인들을 만족하는 항목수가 증 가할수록 당뇨병 발생률이 증가하였으며, 대사증후군의 구성요인 중 공복혈당이 당뇨병 발생의 가장 큰 중요 인자임을 확인하였다.
요 약
연구배경:
대사증후군은 심혈관 질환 및 당뇨병 발생이 높은 위험 군을 예측하는 데 유용한 지표로 사용되고 있다. 현재까지 우리나 라에서는 대사증후군 구성인자와 당뇨병에 대한 연구들 대부분이 단면연구를 통한 분석이었고, 코호트 연구가 없었다. 본 연구에서는 국민건강보험공단 표본자료를 이용한 대사증후군 및 각각의 구성 인자와 당뇨병 발생과의 연관성에 대하여 다루었다.방법:
국민건강보험공단의 표본 코호트 자료를 사용하여 2010년부 터 2013년까지 1차 일반건강검진 및 생애전환기건강진단을 받은 수 진자 211,541명을 대상으로 이 중 30대 미만 25,133명, 결측 180명, 검 진 전 당뇨병을 진단 받은 19,971명은 제외되어 총 166,257명이 분석 대상자로 선정되었다. 변수 분석에는 카이제곱 검정과 독립 t-검정을 사용하였다. 대사증후군의 구성인자와 당뇨병 발생 위험과의 연관 성은 다중 콕스 회귀분석으로 인과관계를 확인하였다.결과:
연구 대상자 총 166,257명 중 추적 관찰기간 동안 새롭게 당뇨 병 진단을 받은 사람은 4,405명이었다.결론:
대사증후군뿐만 아니라 대사증후군의 구성인자들은 나이, 성별, 체질량지수, 음주 및 흡연, 신체활동을 보정한 후에도 당뇨병Theproportionofpeople withoutthediagnosisofdiabetes
0 1.0
0.9
4 Follow-up (y)
0.8
A B
C D
3 2
1
Figure 2. Comparison of occurrence rate of diabetes according to body weight and metabolic syndrome. (A) Normal weight people without the diagnosis of metabolic syndrome, (B) normal weight with the diagnosis of metabolic syndrome, (C) obese people without the diagnosis of metabolic syndrome, (D) obese people with the diagnosis of metabolic syndrome.
상정은 외. 대사증후군 구성 요인별 당뇨병 발생 예측도 비교 Korean Journal of Family Practice
KJFP
발생 위험을 증가시켰다. 4년간 추적 관찰기간 동안 대사증후군의 구성인자들을 만족하는 항목수가 증가할수록 당뇨병 발생률이 증 가하였다. 또한 대사 증후군의 구성인자 중 공복혈당이 당뇨병 발생 의 가장 큰 중요인자임을 확인하였다.
중심단어:
대사증후군; 당뇨병; 공복고혈당; 건강보험공단자료REFERENCES
1. Bae SJ, Lee MK. Definition and diagnosis of the metabolic syndrome. J Ko- rean Med Assoc 2005; 48: 1157-64.
2. Kwon HS. Update on the metabolic syndrome. Biowave 2007; 9.
3. Isomaa B, Almgren P, Tuomi T, Forsén B, Lahti K, Nissén M, et al. Cardiovas- cular morbidity and mortality associated with the metabolic syndrome. Di- abetes Care 2001; 24: 683-9.
4. Haffner SM, Valdez RA, Hazuda HP, Mitchell BD, Morales PA, Stern MP.
Prospective analysis of the insulin-resistance syndrome (syndrome X). Dia- betes 1992; 41: 715-22.
5. Nestel P, Lyu R, Low LP, Sheu WH, Nitiyanant W, Saito I, et al. Metabolic syndrome: recent prevalence in East and Southeast Asian populations. Asia Pac J Clin Nutr 2007; 16: 362-7.
6. Aguilar M, Bhuket T, Torres S, Liu B, Wong RJ. Prevalence of the metabolic syndrome in the United States, 2003-2012. JAMA 2015; 313: 1973-4.
7. Lim S, Shin H, Song JH, Kwak SH, Kang SM, Won Yoon J, et al. Increasing prevalence of metabolic syndrome in Korea: the Korean National Health and Nutrition Examination Survey for 1998-2007. Diabetes Care 2011; 34:
1323-8.
8. Wilson PW, D’Agostino RB, Parise H, Sullivan L, Meigs JB. Metabolic syn- drome as a precursor of cardiovascular disease and type 2 diabetes mellitus.
Circulation 2005; 112: 3066-72.
9. Lorenzo C, Okoloise M, Williams K, Stern MP, Haffner SM. The metabolic
syndrome as predictor of type 2 diabetes: the San Antonio heart study. Dia- betes Care 2003; 26: 3153-9.
10. Laaksonen DE, Lakka HM, Niskanen LK, Kaplan GA, Salonen JT, Lakka TA. Metabolic syndrome and development of diabetes mellitus: application and validation of recently suggested definitions of the metabolic syndrome in a prospective cohort study. Am J Epidemiol 2002; 156: 1070-7.
11. Ballantyne CM, Hoogeveen RC, McNeill AM, Heiss G, Schmidt MI, Dun- can BB, et al. Metabolic syndrome risk for cardiovascular disease and diabe- tes in the ARIC study. Int J Obes (Lond) 2008; 32 Suppl 2: S21-4.
12. Hwang YC, Jee JH, Oh EY, Choi YH, Lee MS, Kim KW, et al. Metabolic syn- drome as a predictor of cardiovascular diseases and type 2 diabetes in Kore- ans. Int J Cardiol 2009; 134: 313-21.
13. Lee J, Lee JS, Park SH, Shin SA, Kim K. Cohort profile: the National Health Insurance Service-National Sample Cohort (NHIS-NSC), South Korea. Int J Epidemiol 2016 January 28 [Epub]. doi: 10.1093/ije/dyv319.
14. Heng D, Ma S, Lee JJ, Tai BC, Mak KH, Hughes K, et al. Modification of the NCEP ATP III definitions of the metabolic syndrome for use in Asians identifies individuals at risk of ischemic heart disease. Atherosclerosis 2006;
186: 367-73.
15. Klein BE, Klein R, Lee KE. Components of the metabolic syndrome and risk of cardiovascular disease and diabetes in Beaver Dam. Diabetes Care 2002; 25: 1790-4.
16. Katzmarzyk PT, Church TS, Janssen I, Ross R, Blair SN. Metabolic syn- drome, obesity, and mortality: impact of cardiorespiratory fitness. Diabetes Care 2005; 28: 391-7.
17. Hinnouho GM, Czernichow S, Dugravot A, Batty GD, Kivimaki M, Singh- Manoux A. Metabolically healthy obesity and risk of mortality: does the definition of metabolic health matter? Diabetes Care 2013; 36: 2294-300.
18. Kim HM, Kim DJ, Jung IH, Park C, Park J. Prevalence of the metabolic syn- drome among Korean adults using the new International Diabetes Federa- tion definition and the new abdominal obesity criteria for the Korean peo- ple. Diabetes Res Clin Pract 2007; 77: 99-106.