https://doi.org/10.14734/PN.2020.31.1.7 pISSN 2508-4887•eISSN 2508-4895
Yun Jeong Park, Bachelor1, Young Hwa Kwak, Bachelor1, Hee Yon Kim, Bachelor1, Sang Won Han, PhD2, Eui Hyeok Kim, Master2
1Department of Obstetrics and Gynecology, Yonsei University College of Medicine, Seoul;
2Department of Obstetrics and Gynecology, National Health Insurance Service Ilsan Hospital, Goyang, Korea
Objective: This study aimed to determine neonatal outcomes and morbidities according to gesta
tional weeks in term births.
Methods: This was a retrospective observational study of 626 singleton deliveries from 37 0/7 to 41 6/7 gestational weeks in National Health Insurance Service Ilsan Hospital using electronic medical record data from January 1, 2011 to December 31, 2017 Neonatal outcomes and morbidity in women who attempted vaginal delivery were compared at each gestational week.
Results: Early term births (37 0/7 to 38 6/7) accounted for 38.7% of fullterm births (242/626). The rate of neonatal intensive care unit (NICU) admission was the lowest at 39 gestational weeks (25.0%) and highest at 41 weeks (30.8%). Compared to 39 gestational weeks, the rate of NICU admission days for more than 5 days and 5minute Apgar score less than 7 were higher at 37 gestational weeks (26.6%
vs. 11.3%, P=0.028 and 7.6% vs. 2.0%, P=0.011, respectively). The intubation rate was lower in 39 weeks than in 37 weeks without statistical significance. The incidence of meconiumstained amniotic fluid increased with gestational weeks from 37 weeks (1.3% at 37 weeks, 30.8% at 41 weeks, P<0.001).
Severe neonatal morbidities were very low and not different according to gestational weeks.
Conclusion: Among term births, our study showed that the prevalence of neonatal morbidities was highest at 37 gestational weeks and lowest at 39 gestational weeks. However, there was no significant difference in severe morbidities. Further studies are urgently required to determine the appropriate timing of delivery to avoid common neonatal complications.
Key Words: Term birth, Intensive care, Neonatal, Morbidity, Gestational age
Introduction
Neonates born before 37/0 gestational weeks since the first day of their mother’s last menstrual period are classified as preterm, whereas those delivered after 41/0 gestational weeks are classified as postterm.1,2 The morbidities and mortalities of preterm and postterm infants are well known and established.3-5 Compared with preterm or postterm birth, term birth, which has traditionally been defined as birth between 37 0/7 and 41 6/7 gestational weeks, used to be regarded as uniform and good, compared with preterm or postterm birth.
“Term gestation” is used to let clinicians and the public consider the optimal time for delivery of healthy neonates during the whole term period. Recent studies, however, have shown that the fetus matures continuously even during the 5-week term period;6 hence, neonatal out- comes vary according to the timing of delivery even within the term period.7-9 Infants born before 39 gestational weeks are at an increased risk for neonatal adverse respiratory out- comes, and the risk increases with decreased gestational age at birth.10 Early term birth should be considered only when the conditions of the mother, baby, or both can result in worse outcomes if pregnancy is allowed to continue.
In 2010, Fleischman et al.11 first suggested the subcategory called early term from 37 0/7 to Received: 28 February 2019
Revised: 17 July 2019 Accepted: 14 October 2019 Correspondence to Eui Hyeok Kim, Master Department of Obstetrics and Gynecology, National Health Insurance Service Ilsan Hospital, 100 Ilsanro, Ilsandonggu, Goyang 10444, Korea
Tel: +82319000211 Fax: +82319000138 E-mail: [email protected] Copyright© 2020 by The Korean Society of Perinatology
This is an Open Access article distributed under the terms of the Creative Com
mons Attribution NonCommercial License (http://creativecommons.org/
license/bync/4.0/), which permits unrestricted noncommercial use, distribution, and reproduction in any
Neonatal Outcomes in Term Births accor
ding to Gestational Weeks
fol lows: early term, 37 0/7 to 38 6/7 gestational weeks; full term, 39 0/7 to 40 6/7 gestational weeks; late term, 41 0/7 to 41 6/7 gestational weeks; and postterm, 42 0/7 gestational weeks and beyond.6
There are several important and complicated principles to consider in the timing of delivery. Although it is most important to minimize maternal and neonatal risks and to ensure the safety of the mother and fetus, obstetricians should also consider the practice environment in hospitals and patient preference.
In recent studies, neonates born at 37 to 38 gestational weeks had more respiratory complications, such as respiratory di- stress syndrome, transient tachypnea of newborns, pneumonia, and feeding difficulties, than neonates born after 38 gestational weeks.12-14 In some cases, early term delivery and even preterm delivery may be warranted for either maternal or newborn be- nefit or both, and healthcare providers may need to weigh com- peting risks and benefits for the mother and newborn; therefore, decisions regarding the timing of delivery must be individualized depending on the situation. Obstetricians should determine the optimal delivery time based on proven data and expert consensus in consideration of risks and benefits according to gestational weeks.7 Considering that labor induction or augmen tation in term pregnancy represents the most frequently conducted inter- ventional procedure in the field of obstetrics15,16 and the rapid increase in the rate of cesarean section,17 which includes planned cesarean delivery without labor such as ma ternal request for cesarean delivery and breech presentation, the timing of deli- very has become more important recently.
Thus, it seems important and useful to provide information about neonatal outcomes according to gestational week even in term birth. Such studies have been relatively well documented in United States and European literature, but there are no data in the Republic of Korea to prove that full-term infants have better outcomes than early term infants. Hence, this study aimed to determine neonatal outcomes and morbidities in term births according to gestational weeks.
Methods
1. Study design and cohort
We conducted an observational retrospective study of 626
singleton deliveries at the National Health Insurance Service Ilsan Hospital in the Republic of Korea using electronic medical record (EMR) data between January 1, 2011, and December 31, 2017 (Fig. 1). The study was approved by the institutional re- view board of National Health Insurance Service Ilsan Hospital (number NHIMC-2017-04-031). The need for informed consent was waived because of the retrospective design of the study.
All women with fetuses aged from 37 0/7 to 41 6/7 gestational weeks who were planning vaginal delivery were considered for study participation. Exclusion criteria were major fetal anomalies requiring postpartum urgent care (such as hydrocephalus or major cardiac disease), still birth, twin pregnancy, breech pre- sentation, neonates before 37/0 or after 41/6 gestational weeks, severe preeclampsia with uncontrollable hypertension, uncon- trollable diabetes or severe intrauterine growth restriction (birth weight <5%) and scheduled cesarean section without labor;
minor abnormalities, such as hydronephrosis or small cardiac ventricular septal defect, were included.
2. Study end points and data collection
The primary end points of this study were neonatal outcomes and morbidities at each gestational week. Gestational weeks were determined by obstetricians using the earliest ultrasono- graphy examination from any obstetric clinic, including National Health Insurance Service Ilsan Hospital, or maternal clinical history, such as the first date of the mother’s last menstrual period.2 If the gestational weeks obtained from ultrasonography ex amination were different from those obtained using the first date of the mother’s last menstrual period (by more than 7 days), we determined the final gestational age by ultrasonography examination.
From the institution’s EMRs, we obtained the following infor- mation concerning the women’s delivery mode (vaginal or ce sa-
Study population (626)
Early term birth (242, 38.7%)
37 0/7 to 37 6/7 GW (79, 13%)
38 0/7 to 38 6/7 GW (163, 26%)
Full term birth (371, 59.3%)
39 0/7 to 39 6/7 GW (247, 39%)
40 0/7 to 40 6/7 GW (124, 20%)
Late term birth (13, 2.1%)
41 0/7 ~ GW (13, 2%)
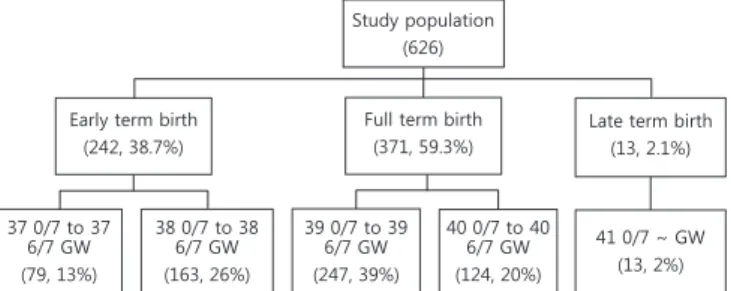
Fig. 1. Flow diagram of patient population. GW, gestational weeks.
after adjustment. All P-values were 2-tailed, and P<0.05 was considered statistically significant. All analyses were performed using the Statistical Package for Social Sciences, version 23.0 (IBM Corp., Armonk, NY, USA).
Results
Six hundred twenty-six women were recruited for this study;
there were 242 (38.7%) early term births, 371 (59.3%) full-term births, and 13 (2.1%) late-term births (more than 42 0/7 gesta- tional weeks). Table 1 summarizes the characteristics of the study population.
Among early term births, 79 (13%) deliveries were from 37 0/7 to 37 6/7 gestational weeks and 163 (26%) were from 38 0/7 to 38 6/7 gestational weeks. Among full-term births, 247 (39%) deliveries were from 39 0/7 to 39 6/7 gestational weeks and 124 (20%) were from 40 0/7 to 40 6/7 gestational weeks. Among late- term births, 13 (2%) deliveries were at more than 41 gestational weeks (Table 1). The average age of pregnant women was 32.0 years, with an average BMI of 21.8 kg/m2, and these variables were not statistically significantly different between the groups.
Overall, 201 (32.1%) women had spontaneous labor, and 425 (67.9%) attempted induced labor. Forty-five (7.2%) women de- livered after premature rupture of membranes (Table 1).
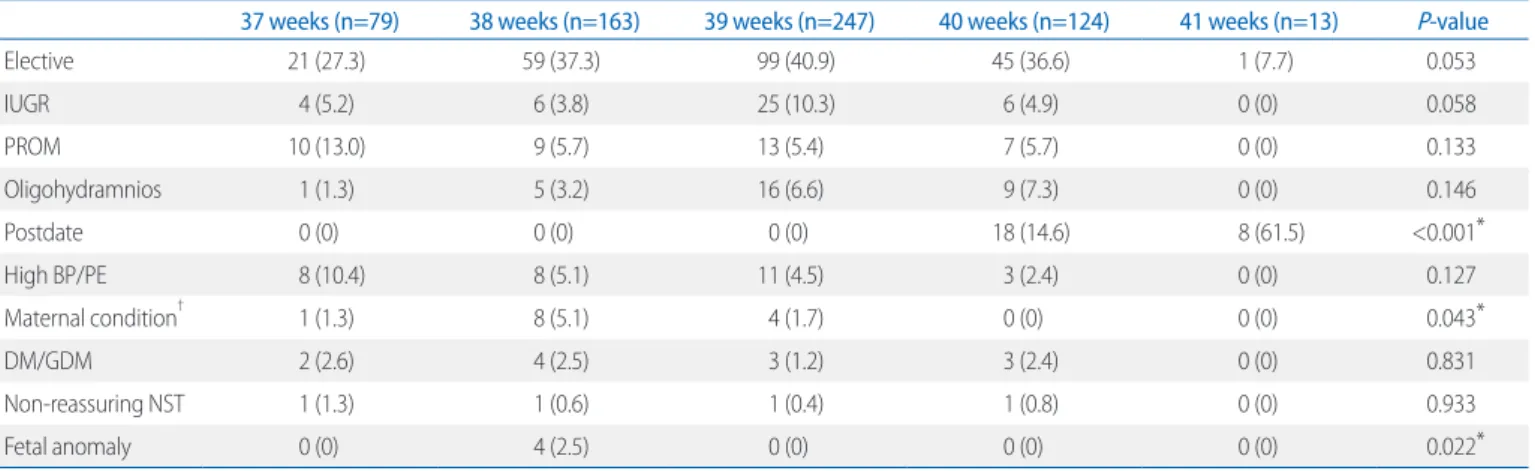
The most common reasons for labor induction were elective induction (36.7%), followed by intrauterine growth restriction (6.7%) and oligohydramnios (5.1%) (Table 2). Table 3 showed the indications for cesarean section and except maternal request for cesarean during labor, there was no difference among the gestational weeks.
Neonatal birth weight was different according to gestational rean delivery): age; gestational weeks; decrease in the hemo-
globin level after delivery, which indicates the amount of blood loss during delivery; length of hospital stay; body weight before pregnancy; body mass index (BMI) before pregnancy; body weight at full term; BMI at full term; weight gain during preg- nancy; and parity. To evaluate neonatal complications, we col- lected all neonatal data for infants delivered vaginally from 37 0/7 gestational weeks to 41 6/7 gestational weeks from the EMRs. We also assessed the neonatal weight, 1-minute and 5-minute Apgar scores, neonatal intensive care unit (NICU) admission rate, meconium status, and neonatal intubation status.
3. Procedure for labor induction
Women in the induction group were admitted to the delivery room via the outpatient department. Because Braxton-Hicks contractions, which are not painful and are discovered incident- ally on a non-stress test at near term, are not accompanied by changes in cervical length, we did not consider them as sponta- neous labor. Labor induction was attempted with intravenous injection of oxytocin (Pitocin, 10 IU/mL; Jeil Pharmaceutical Co., Ltd., Daegu, Korea) or intravaginal administration of prostag- landin E2 (Propess, 10 mg; Bukwang Pharm Co., Ltd., Seoul, Korea), and when women developed spontaneous labor pain, augmentation with oxytocin was attempted if labor progression was inadequate.
4. Statistical analyses
Demographic and clinical characteristics were compared ac- cording to gestational weeks using the Student t-test or analysis of variance for continuous values and the χ2 test or Fisher’s exact test for categorical values. Differences among the sub- groups were tested by multiple logistic regression methods
Table 1. Characteristics of the Study Population
37 weeks (n=79) 38 weeks (n=163) 39 weeks (n=247) 40 weeks (n=124) 41 weeks (n=13) P-value
Age (years) 32.2±4.7 32.0±5.2 32.1±4.7 31.6±4.6 33.0±3.7 0.524
BMI 21.8±4.4 22.0±3.8 21.9±3.6 21.5±3.6 22.7±2.3 0.407
Spontaneous labor 31 (39.2) 59 (36.2) 75 (30.4) 32 (25.8) 4 (30.8) 0.222
Induction of labor 48 (60.8) 104 (63.8) 172 (69.6) 92 (74.2) 9 (69.2) 0.222
PROM 9 (11.4) 10 (6.1) 14 (5.7) 12 (9.7) 0 (0) 0.251
C/sec rate 10 (12.7) 11 (6.7) 30 (12.1) 12 (9.7) 2 (15.4) 0.407
Values are presented as mean±standard deviation or number (%).
Abbreviations: BMI, body mass index; PROM, premature rupture of membranes; C/sec, Cesarean section.
birth and a 5-minute Apgar score less than 7 were the lowest at 41 gestational weeks (Table 4). The incidence of meconium- stained amniotic fluid increased with gestational weeks with statistically significance (P<0.001) (Table 4). Severe neonatal morbidities such as hyaline membrane disease, respiratory dis- weeks (P<0.001) and the overall percentile of neonates weighing
less than 2.5 kg was 5.9 % and was mainly distributed at 37 weeks (Table 4). The rate of NICU admissions was the lowest at 39 gestational weeks (17.8%) without statistically significance.
The rates of NICU admission days for more than 5 days after Table 2. Reasons for Induction of Labor
37 weeks (n=79) 38 weeks (n=163) 39 weeks (n=247) 40 weeks (n=124) 41 weeks (n=13) P-value
Elective 21 (27.3) 59 (37.3) 99 (40.9) 45 (36.6) 1 (7.7) 0.053
IUGR 4 (5.2) 6 (3.8) 25 (10.3) 6 (4.9) 0 (0) 0.058
PROM 10 (13.0) 9 (5.7) 13 (5.4) 7 (5.7) 0 (0) 0.133
Oligohydramnios 1 (1.3) 5 (3.2) 16 (6.6) 9 (7.3) 0 (0) 0.146
Postdate 0 (0) 0 (0) 0 (0) 18 (14.6) 8 (61.5) <0.001*
High BP/PE 8 (10.4) 8 (5.1) 11 (4.5) 3 (2.4) 0 (0) 0.127
Maternal condition† 1 (1.3) 8 (5.1) 4 (1.7) 0 (0) 0 (0) 0.043*
DM/GDM 2 (2.6) 4 (2.5) 3 (1.2) 3 (2.4) 0 (0) 0.831
Nonreassuring NST 1 (1.3) 1 (0.6) 1 (0.4) 1 (0.8) 0 (0) 0.933
Fetal anomaly 0 (0) 4 (2.5) 0 (0) 0 (0) 0 (0) 0.022*
Values are presented as number (%).
Abbreviations: IUGR, intrauterine growth restriction; PROM, premature rupture of membranes; BP, blood pressure; PE, preeclampsia; DM, diabetes mellitus; GDM, gestational diabetes mellitus; NST, nonstress test.
*Statistically significant.
†Maternal condition included an increased maternal liver enzyme level and thrombocytopenia. Fetal anomaly included fetal hydronephrosis and fetal ovarian cyst.
Table 3. Indications for Cesarean Delivery
37 weeks (n=10) 38 weeks (n=11) 39 weeks (n=30) 40 weeks (n=12) 41 weeks (n=2) P-value
Fetal distress 3 (30.0) 2 (18.2) 10 (33.3) 4 (33.3) 0 (0) 0.517
Chorioamnionitis 0 (0) 0 (0) 1 (3.3) 0 (0) 0 (0) 0.820
Failure to progress 7 (70.0) 10 (71.8) 16 (53.4) 7 (58.4) 0 (0) 0.534
Unstable lie 0 (0) 0 (0) 1 (3.3) 0 (0) 0 (0) 0.820
Maternal request 0 (0) 0 (0) 2 (6.7) 1 (8.3) 2 (100) <0.001*
Values are presented as number (%).
*Statistically significant.
Table 4. Neonatal Outcomes according to Gestational Weeks
37 weeks (n=79) 38 weeks (n=163) 39 weeks (n=247) 40 weeks (n=124) 41 weeks (n=13) P-value
Fetal weight (gm) 2,904±462 3,023±448 3,186±408 3,385±364 3,540±529 <0.001*
Less than 2,500 gm 12 (15.2) 14 (8.60) 10 (4.0) 0 (0) 0 (0) <0.001*
NICU admission rate 23 (29.1) 40 (24.5) 44 (17.8) 31 (25.0) 4 (30.8) 0.172
NICU AD >5 21 (26.6) 25 (15.3) 28 (11.3) 16 (12.9) 1 (7.7) 0.017*
Meconium stained AF 1 (1.3) 15 (9.2) 29 (11.7) 29 (23.4) 4 (30.8) <0.001*
1 minute Apgar <7 29 (37.0) 45 (27.6) 76 (30.8) 52 (41.9) 5 (38.5) 0.098
5 minute Apgar <7 6 (7.6) 9 (5.5) 5 (2.0) 14 (11.3) 0 (0) 0.004*
Intubation 6 (7.6) 7 (4.3) 8 (3.2) 4 (3.2) 0 (0) 0.432
Values are presented as mean±standard deviation or number (%).
Abbreviations: NICU, neonatal intensive care unit; AD, admission days; AF, amniotic fluid.
*Statistically significant.
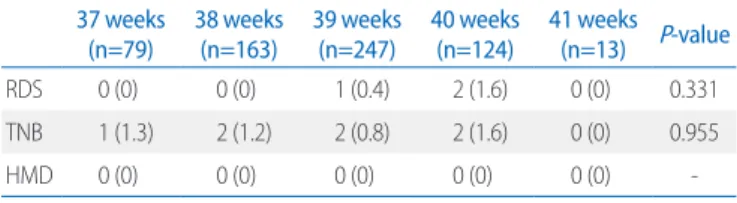
tress syndrome, and tachypnea of newborns were very rare and did not differ according to gestational weeks (Table 5).
Compared to 39 gestational weeks, the rate of NICU admission days for more than 5 days and 5-minute Apgar score less than 7 were higher at 37 gestational weeks (26.6% vs. 11.3%, P=0.028 and 7.6% vs. 2.0%, P=0.011, respectively) (Table 6). Meconium stained amniotic fluid was, however, higher at 39 gestational weeks. The intubation rate was lower in 39 weeks than in 37 weeks without statistical significance.
Discussion
Births at 39 gestational weeks were reported to have the lowest neonatal morbidity and mortality.18 Our results also showed that early term delivery at 37 or 38 gestational weeks should be avoided and that elective induced labor should be delayed until 39 gestational weeks or more in cases of uncomplicated maternal
or fetal conditions.
Among neonatal morbidities, respiratory disease mainly affects preterm infants.19,20 Therefore, neonatal morbidity in term in- fants has received less attention, and risks in this group have been less well characterized, as term birth was regarded as a homogeneous low-risk group.
A recent study showed that the overall frequency of induced labor more than doubled in the United States, increasing from 9.5% in 1990 to up to 23.8% in 2010.16 Additionally, elective in- duction for the mother and provider’s convenience accounted for approximately 40% of cases.21 The specific timing of term birth and its outcome on neonatal prognosis have become important public health issues.7 Our results were consistent with the recent recommendation of The American College of Obstetrics and Gynecology Committee Opinion to wait until 39 gestational weeks for delivery.22 However, in many situations, including in our study, elective (not medically indicated) induced labor oc- curred before 39 gestational weeks.23 In a recent study from Korea, delivery between 39 and 41 weeks minimized fetal/infant mortality, in non-small for gestational age24 and the other study from Korea also reported that neonatal morbidities including respiratory morbidities, intracranial hemorrhage, and admission to NICU were significantly higher in neonates who were delivered at 37 weeks’ gestation, compared to those in neonates who were delivered at 39 weeks’ gestation.25 Compared to delivery at 39 gestational weeks, early term delivery at 37 gestational weeks was associated with a significant increase in neonatal morbidity, and adverse outcomes were lowest with delivery from 38 0/7 to 39 6/7 gestational weeks. Our study also showed that the preva- lence of severe neonatal morbidity or mortality, such as hyaline membrane disease or respiratory distress syndrome requiring the use of surfactant, was rare throughout the entire term birth.
Information on neonatal outcomes based on conditions leading to delivery is useful for consultations with women when discussing benefits according to the delivery time even in term births with an uncomplicated pregnancy.
The main strengths of the present study lie in the analysis of conditions leading to delivery in a single institution with the same protocol and use of EMRs with detailed information about conditions associated with delivery. EMRs provided data of in- duced labor, the indication for induction, reason for cesarean delivery, and various maternal conditions about deliveries. Addi- Table 5. Incidence of Severe Neonatal Morbidities
37 weeks
(n=79) 38 weeks
(n=163) 39 weeks
(n=247) 40 weeks
(n=124) 41 weeks (n=13) P-value
RDS 0 (0) 0 (0) 1 (0.4) 2 (1.6) 0 (0) 0.331
TNB 1 (1.3) 2 (1.2) 2 (0.8) 2 (1.6) 0 (0) 0.955
HMD 0 (0) 0 (0) 0 (0) 0 (0) 0 (0)
Values are presented as number (%).
Abbreviations: RDS, respiratory distress syndrome; TNB, transient neonatal brady
cardia; HMD, hyaline membrane disease.
Table 6. Comparison of Outcomes between 37 and 39 Gestational Weeks
37 weeks
(n=79) 39 weeks
(n=247) P-value Adjusted P-value*
Primigravida 24 (30.4) 73 (29.6) 0.889 0.354
Engagement 68 (86.1) 21 (86.6) 0.898 0.761
ROM 18 (22.8) 31 (12.6) 0.027† 0.050†
5 minute Apgar score <7 6 (7.6) 5 (2.0) 0.028† 0.011† NICU admission rate 23 (29.1) 44 (17.8) 0.045† 0.099
NICU AD >5 21 (26.6) 28 (11.3) 0.002† 0.029†
Meconium stained AF 1 (1.3) 29 (11.7) 0.003† 0.002†
Intubation 6 (7.6) 8 (3.2) 0.113 0.092
Values are presented as number (%).
Abbreviations: ROM, rupture of membranes; NICU, neonatal intensive care unit;
AD, admission days; AF, amniotic fluid.
*Adjusted for maternal age, fetal weight, postdate delivery, maternal condition, fetal anomaly, maternal request.
†Statistically significant.
tionally, neonatal morbidities were evaluated by the Apgar score measured by the same institution; hence, we could determine neonatal outcome more accurately, with decreased inter-insti- tutional variation. To the best of our knowledge, this study is the first to evaluate neonatal outcomes, only in women who were planning vaginal delivery and had labor pain, according to ges tational age in term pregnancy in the Republic of Korea.
Deli veries with labor can be different from those without labor, and neonatal respiratory problems are more common in cases of scheduled cesarean delivery before labor than in cases of vaginal birth or cesarean delivery during labor.10,26
Several limitations should be considered when interpreting the present study findings. First, the number of participants was too small for us to generalize our study outcomes to other cohorts. Second, and most importantly, we could not access the results according to delivery precursors or maternal conditions such as induction indications, which could affect neonatal mor- bidities, although there were no significant differences in delivery precursors or maternal conditions between gestational weeks.
Even subcategorizing more participants according to the ma- ternal or neonatal situation could be difficult because of the numerous maternal and neonatal conditions. Lastly, as women with more severe conditions, such as uncontrollable diabetes or hypertension, were more likely to have induced labor earlier or delivery that could have contributed to increased neonatal mor- bidities, our results should be interpreted with caution. Herein, neonatal conditions were better for late-term deliveries than for early term deliveries. Because we did not know the effect of neo- natal outcomes on expectant management in spontaneous term deliveries,27 we should have categorized deliveries according to reasons for induced labor in addition to gestational age
In conclusion, among term births, our study has shown that the prevalence of neonatal morbidity was highest at 37 gestational weeks and lowest at 39 weeks, but there was no significant difference in severe morbidities and mortalities in term birth, and the differences between 38 and 39 gestational weeks were unremarkable. Early term delivery should be attempted only when an accepted maternal or fetal indication for delivery exists.
Further large-scale prospective studies are urgently needed to determine the appropriate timing of delivery and to avoid com- mon neonatal complications in term births.
Acknowledgements
This research was supported by grants from National Health Insurance Service Ilsan Hospital.
Conflict of interest
No potential conflict of interest relevant to this article was reported.
References
1) World Health Organization. ICD-10: international statistical classification of diseases and related health problems. 10th ed. Geneva: World Health Organization, 2004.
2) American Academy of Pediatrics, The American College of Obstetrician and Gynecologists. Guidelines for perinatal care. 7th ed. Washington, DC: American Academy of Pediatrics Committee on Fetus and Newborn, 2013.
3) Nakling J, Backe B. Pregnancy risk increases from 41 weeks of gestation.
Acta Obstet Gynecol Scand 2006;85:663-8.
4) Engle WA, Tomashek KM, Wallman C; Committee on Fetus and Newborn, American Academy of Pediatrics. "Late-preterm" infants: a population at risk. Pediatrics 2007;120:1390-401.
5) Divon MY, Haglund B, Nisell H, Otterblad PO, Westgren M. Fetal and neo natal mortality in the postterm pregnancy: the impact of gestational age and fetal growth restriction. Am J Obstet Gynecol 1998;178:726-31.
6) Spong CY. Defining "term" pregnancy: recommendations from the de- fining "term" pregnancy workgroup. JAMA 2013;309:2445-6.
7) Spong CY, Mercer BM, D'alton M, Kilpatrick S, Blackwell S, Saade G. Ti- ming of indicated late-preterm and early-term birth. Obstet Gynecol 2011;118:323-33.
8) Reddy UM, Bettegowda VR, Dias T, Yamada-Kushnir T, Ko CW, Willinger M. Term pregnancy: a period of heterogeneous risk for infant mortality.
Obstet Gynecol 2011;117:1279-87.
9) Engle WA. Morbidity and mortality in late preterm and early term new- borns: a continuum. Clin Perinatol 2011;38:493-516.
10) Morrison JJ, Rennie JM, Milton PJ. Neonatal respiratory morbidity and mode of delivery at term: influence of timing of elective caesarean sec- tion. Br J Obstet Gynaecol 1995;102:101-6.
11) Fleischman AR, Oinuma M, Clark SL. Rethinking the definition of “term pregnancy”. Obstet Gynecol 2010;116:136-9.
12) De Luca R, Boulvain M, Irion O, Berner M, Pfister RE. Incidence of early neonatal mortality and morbidity after late-preterm and term cesarean delivery. Pediatrics 2009;123:e1064-71.
13) Hourani M, Ziade F, Rajab M. Timing of planned caesarean section and
the morbidities of the newborn. N Am J Med Sci 2011;3:465-8.
14) Consortium on Safe Labor, Hibbard JU, Wilkins I, Sun L, Gregory K, Ha- berman S, et al. Respiratory morbidity in late preterm births. JAMA 2010;
304:419-25.
15) Murthy K, Grobman WA, Lee TA, Holl JL. Trends in induction of labor at early-term gestation. Am J Obstet Gynecol 2011;204:435.e1-6.
16) Osterman MJ, Martin JA. Recent declines in induction of labor by gesta- tional age. NCHS Data Brief 2014;155:1-8.
17) American College of Obstetricians and Gynecologists (College), Society for Maternal-Fetal Medicine, Caughey AB, Cahill AG, Guise JM, Rouse DJ.
Safe prevention of the primary cesarean delivery. Am J Obstet Gynecol 2014;210:179-93.
18) McIntire DD, Leveno KJ. Neonatal mortality and morbidity rates in late preterm births compared with births at term. Obstet Gynecol 2008;111:
35-41.
19) Usher RH, Allen AC, McLean FH. Risk of respiratory distress syndrome related to gestational age, route of delivery, and maternal diabetes. Am J Obstet Gynecol 1971;111:826-32.
20) Dani C, Reali MF, Bertini G, Wiechmann L, Spagnolo A, Tangucci M, et al.
Risk factors for the development of respiratory distress syndrome and transient tachypnoea in newborn infants. Italian Group of Neonatal Pneumology. Eur Respir J 1999;14:155-9.
21) Dublin S, Johnson KE, Walker RL, Avalos LA, Andrade SE, Beaton SJ, et al.
Trends in elective labor induction for six United States health plans, 2001-2007. J Womens Health (Larchmt) 2014;23:904-11.
22) American College of Obstetricians and Gynecologists. ACOG committee opinion no. 561: nonmedically indicated early-term deliveries. Obstet Gynecol 2013;121:911-5.
23) Tita AT, Landon MB, Spong CY, Lai Y, Leveno KJ, Varner MW, et al. Timing of elective repeat cesarean delivery at term and neonatal outcomes. N Engl J Med 2009;360:111-20.
24) Ko HS, Wie JH, Choi SK, Park IY, Park YG, Shin JC. Optimal time of delivery to reduce the risk of infant mortality in small and normally grown fe- tuses: a national cohort study in Korea. PLoS One 2018;13:e0209308.
25) Ko HS, Jang YR, Yun H, Wie J, Choi SK, Park IY, et al. Late-preterm infants, early-term infants, and timing of elective deliveries; current status in a Korean medical center. J Matern Fetal Neonatal Med 2019;32:1267-74.
26) Hansen AK, Wisborg K, Uldbjerg N, Henriksen TB. Risk of respiratory mor- bidity in term infants delivered by elective caesarean section: cohort study. BMJ 2008;336:85-7.
27) Salemi JL, Pathak EB, Salihu HM. Infant outcomes after elective early- term delivery compared with expectant management. Obstet Gynecol 2016;127:657-66.