Korean J Gastroenterol Vol. 67 No. 3, 142-145 http://dx.doi.org/10.4166/kjg.2016.67.3.142 pISSN 1598-9992 eISSN 2233-6869
CASE REPORT
Korean J Gastroenterol, Vol. 67 No. 3, March 2016 www.kjg.or.kr
조기위암의 점막하박리술 후 발생한 위주변 농양
정지윤, 김준성, 김병욱, 박성민, 김기준, 류승지, 김영욱, 지정선, 최 황
가톨릭대학교 의과대학 내과학교실, 인천성모병원 소화기내과
Perigastric Abscess as a Complication of Endoscopic Submucosal Dissection for Early Gastric Cancer: First Case Report
Ji Yun Jung, Joon Sung Kim, Byung-Wook Kim, Sung Min Park, Gi Jun Kim, Seung Ji Ryu, Young Wook Kim, Jeong Seon Ji, and Hwang Choi Division of Gastroenterology, Department of Internal Medicine, Incheon St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Incheon, Korea
Endoscopic submucosal dissection (ESD) for early gastric cancer (EGC) is a widely accepted and well established procedure because of its curative potential and low invasiveness compared with surgery. Perforation is a potential major complication during ESD, and non-surgical treatments such as endoscopic closure with clips are sufficient in most cases. Here, we report a case of perigastric abscess that occurred as a complication of ESD for EGC. The patient improved with administration of antibiotics without surgical intervention. (Korean J Gastroenterol 2016;67:142-145)
Key Words: Endoscopic submucosal dissection; Early gastric cancer; Perigastric abscess
Received September 5, 2015. Revised November 23, 2015. Accepted December 16, 2015.
CC This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Copyright © 2016. Korean Society of Gastroenterology.
교신저자: 김병욱, 21431, 인천시 부평구 동수로 56, 가톨릭대학교 인천성모병원 소화기내과
Correspondence to: Byung-Wook Kim, Division of Gastroenterology, Department of Internal Medicine, The Catholic University of Korea, Incheon St. Mary’s Hospital, 56 Dongsu-ro, Bupyeong-gu, Incheon 21431, Korea. Tel: +82-32-280-5052, Fax: +82-32-280-5987, E-mail: [email protected]
Financial support: None. Conflict of interest: None.
INTRODUCTION
Perforation is a potential major complication of endo- scopic submucosal dissection (ESD) for gastric epithelial neoplasia. The risk of perforation during ESD is reported to be up to 8%.1 When perforation occurs during ESD, non-surgi- cal management such as endoscopic closure with clips al- lows fast recovery and is sufficient in most cases.2 We re- cently diagnosed and successfully managed with antibiotics a patient with perigastric abscess formation after a mi- cro-perforation during ESD. Although phlegmonous gastric and gastric wall abscess after ESD have been reported, peri- gastric abscess as a complication after ESD has never been published in the English literature.
CASE REPORT
A 63-year-old woman was admitted to our hospital for en- doscopic resection of a gastric epithelial neoplasia. The pa- tient’s medical history was unremarkable except for 10 years of hypertension. She received ESD for early gastric cancer (EGC) with en bloc resection (Fig. 1) without complications.
The resected lesion was measured at 4.5×3.4 cm, histo- pathologic examination revealed tubular adenocarcinoma with moderate differentiation limited to the lamina propria, and lymphovascular invasion was not detected. The size of the adenocarcinoma was measured at 3.0×1.6 cm. She did not complain of any peritoneal irritation signs such as ab- dominal pain and rebound tenderness after the procedure.
However, free air was detected on routine chest X-rays taken
Jung JY, et al. Perigastric Abscess as a Complication of ESD for EGC 143
Vol. 67 No. 3, March 2016
Fig. 1. Procedure of endoscopic sub- mucosal dissection for the lesion. (A) A slightly depressed intramural hemo- rrhagic lesion is noted at the lesser curvature side of the distal corpus. (B) After spraying indigo carmine, mark- ing was done with argon plasma laser.
(C) Precut with hook knife was perfor- med. (D) Dissection of the submu- cosal layer was performed.
Fig. 2. (A) Chest radiograph imme- diately after endoscopic submucosal dissection. Intraperitoneal free air is noted on the right subdiaphragmatic area (arrow). (B) Chest radiograph 4 days after Endoscopic submucosal dissection. The amount of intraperi- toneal free air markedly decreased (arrow).
immediately after the procedure (Fig. 2A). Intravenous pan- toprazole was started on the day of ESD and flomoxef was ad- ministered for three days. Since she did not complain of any peritoneal irritation signs, oral feeding was started two days after ESD. Four days after ESD, chest X-ray showed minimal free air at the right subdiaphragmatic space (Fig. 2B) and lab-
oratory findings revealed leukocyte counts at 5,700/L (reference value, 4,000-9,900/L). She was discharged four days after ESD.
She returned to the outpatient clinic 10 days after ESD complaining of mild epigastric pain but no other symptoms.
Oral proton pump inhibitor was prescribed for one month.
144 정지윤 등. 조기위암의 점막하박리술 후 발생한 위주변 농양
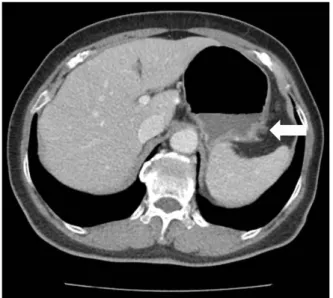
The Korean Journal of Gastroenterology Fig. 3. Initial abdominal computed tomography. It reveals loculated
fluid collection at the perigastric area of fundus (arrow).
Fig. 4. Abdominal computed tomography after 5 weeks. It shows resolution of the previous peri-gastric fluid collection (arrow).
However, three weeks after ESD she came to the emergency room complaining of chilling, myalgia and substernal pain of three days duration. Physical examination revealed a soft abdo- men and no palpable mass. Laboratory examination showed in- creased CRP up to 92.4 mg/L (reference value, 0-5 mg/L) and leukocyte counts of 9,400/L. Abdominal CT showed locu- lated fluid collections abutting the proximal part of the stom- ach, suggesting perigastric abscess (Fig. 3). Empirical anti- biotics for perigastric abscess were administered: intra- venous ceftriaxone with metronidazole for 10 days followed by oral cefditoren for 21 days. Antibiotics were chosen follow- ing the advice of the infectious disease specialist. Blood cul- ture did not harvest any microorganisms. The patient was dis- charged on the ninth hospital day in much improved condition.
An abdominal CT was performed five weeks after initial ab- dominal CT and revealed regression of the perigastric ab- scess (Fig. 4). The patient has been examined regularly in the outpatient clinic for four months, and she has not experi- enced any other events.
DISCUSSION
The exact pathogenesis of perigastric abscess is un- known. It is probably caused by bacterial infection of the se- rosal side of the gastric wall by direct invasion through a breach in the gastric mucosa or secondary to hematogenous spread from a distant infectious source.3 A previous study re-
ported that 38.1% of patients who underwent ESD for gastric neoplasia showed intraperitoneal free air by abdominal CT.4 It is thus plausible that the micro-perforation during ESD might provide an entry of microorganisms into the peritoneal cavity. We assume that contaminated materials might have flowed along the serosal surface of the stomach and finally settled into the lowest part of stomach, the greater curvature side of the fundus, during the procedure in our case.
A previous report described mean fasting periods of 5.3 days for perforations occurring after ESD.5 However, abdo- men CTs after ESD revealed higher rates of perforation not detected on chest X-rays.4 Most of these perforations would go unnoticed since abdomen CTs are not performed routinely. This suggests that perforations after ESD should not be managed in the same manner. It is our policy that pa- tients with minimal intraperitoneal air after ESD without any peritoneal irritation sign are managed as if they have no complications.
Nasogastric tube insertion and intravenous antibiotics might be helpful, but the effectiveness of these treatments and choice of antibiotics are an open question.6,7 European guidelines for ESD suggest broad spectrum antibiotics for perforations complicating gastric ESD. However, there are no guidelines for antibiotic or other management for micro-per- foration immediately after gastric ESD.8
Traditionally, surgery with broad spectrum antibiotics has been used for treating gastric wall abscess. Some reports
Jung JY, et al. Perigastric Abscess as a Complication of ESD for EGC 145
Vol. 67 No. 3, March 2016
suggest endoscopic drainage as an effective treatment for gastric wall abscess.2,3,9-11 However, standard recommenda- tions for perigastric abscess treatment are not established due to limited reports.12 In this case, we administered anti- biotics only without radiologic or endoscopic intervention.
This resulted in complete resolution of the perigastric abscess. Gastric irrigation with saline solution before ESD re- duces the bacterial colony count from gastric juice.13 This pretreatment might be helpful when the possibility of proce- dure-related infection is very high.
A risk of disseminating malignancy in the peritoneal cavity associated with any invasive procedure should be consid- ered, as in our case. Fortunately, peritoneal dissemination is unlikely to occur after gastric perforations during endoscopic resection.14 The patient did not require emergency surgery because the perigastric abscess was localized, the symp- toms were tolerable and improved with conservative man- agement including antibiotics.
In conclusion, this is the first report, to the best of our knowledge, of a perigastric abscess after ESD for EGC suc- cessfully managed with antibiotics. When a patient shows any symptoms of systemic inflammation after ESD for gastric neoplasia, proper diagnostic tools such as abdomen CT should be conducted. Conservative treatment with anti- biotics might be a therapeutic option when the lesion is lo- calized without any sign of peritoneal irritation.
REFERENCES
1. Fujishiro M. Endoscopic submucosal dissection for stomach neoplasms. World J Gastroenterol 2006;12:5108-5112.
2. Minami S, Gotoda T, Ono H, Oda I, Hamanaka H. Complete endo- scopic closure of gastric perforation induced by endoscopic re- section of early gastric cancer using endoclips can prevent sur-
gery (with video). Gastrointest Endosc 2006;63:596-601.
3. Marcos WC, Petrini BG, Xavier RL, Starling RM, Couto JC, Ribeiro GJ. Gastric wall abscess--an uncommon condition treated by an alternative form. Clinics (Sao Paulo) 2010;65:819-821.
4. Cho SJ, Choi IJ, Kim SJ, et al. Clinical significance of intra- peritoneal air on computed tomography scan after endoscopic submucosal dissection in patients with gastric neoplasms. Surg Endosc 2014;28:307-313.
5. Fujishiro M, Yahagi N, Kakushima N, et al. Successful non- surgical management of perforation complicating endoscopic submucosal dissection of gastrointestinal epithelial neoplasms.
Endoscopy 2006;38:1001-1006.
6. Watari J, Tomita T, Toyoshima F, et al. Clinical outcomes and risk factors for perforation in gastric endoscopic submucosal dis- section: A prospective pilot study. World J Gastrointest Endosc 2013;5:281-287.
7. Jeon SW, Jung MK, Kim SK, et al. Clinical outcomes for perfo- rations during endoscopic submucosal dissection in patients with gastric lesions. Surg Endosc 2010;24:911-916.
8. Pimentel-Nunes P, Dinis-Ribeiro M, Ponchon T, et al. Endoscopic submucosal dissection: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2015;47:829-854.
9. Kiil C, Rosenberg J. Gastric intramural abscess successfully drained during gastroscopy. Gastrointest Endosc 2001;53:231- 232.
10. Choong NW, Levy MJ, Rajan E, Kolars JC. Intramural gastric ab- scess: case history and review. Gastrointest Endosc 2003;58:
627-629.
11. Kang BC, Kim KW, Lee SW, Kim JH. Gastric wall abscess: imaging diagnosis and endoscopic treatment. J Comput Assist Tomogr 1998;22:673-675.
12. Lee FI, Ong T, Thiarakan J. Perigastric abscess following Nissen fundoplication. Gastrointest Endosc 1995;41:620.
13. Mori H, Kobara H, Rafiq K, et al. Effects of gastric irrigation on bacterial counts before endoscopic submucosal dissection: a randomized case control prospective study. PLoS One 2013;8:
e65377.
14. Ikehara H, Gotoda T, Ono H, Oda I, Saito D. Gastric perforation during endoscopic resection for gastric carcinoma and the risk of peritoneal dissemination. Br J Surg 2007;94:992-995.