Received: July 7, 2017 Revised: September 7, 2017 Accepted: September 16, 2017
Copyright © 2017. The Korean Academy of Oral &
Maxillofacial Implantology
This is an Open Access article distributed under the terms of the Creative Commons Attrib- ution Non-Commercial License (http://creative- commons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
pISSN : 1229-5418
Implantology 2017; 21(3): 188-196 https://doi.org/10.12972/implantology.20170015
eISSN : 0000-0000 OPEN ACCESS
Anterior Restoration Splinting Implant with Natural Tooth: A Clinical Report
Seoung-Jin Hong, Yi-Hyung Woo, Kung-Rock Kwon, Janghyun Paek*
Department of Prosthodontics, School of Dentistry, KyungHee University, Seoul, Korea
*Corresponding author: Janghyun Paek, [email protected]
Abstract
The maxillary anterior region is considered the “esthetic zone” because of its importance on facial appearance and high visibility. Especially in the anterior region, implant prosthesis with proper soft tissue contours is important for successful esthetic results, this method may also help to reduce soft tissue complications with a gradual molding of the soft tissues profile.
Commonly, it is recommended that dental implants should not be splinted with natural teeth due to the difference in biomechanics and mobility. However, in some cases, the splinting of a natural tooth with an implant seems to be needed. Several studies have described clinical cases where fixed partial dentures are supported by a connection between implants and natural teeth.
In a 39-year-old man who showed periapical abscess of maxillary right central incisor, extraction were planned and after healing period, provisional crown was restored. After transferring the emergence profile of provisional crown, splinted zirconia prostheses were delivered.
Keywords: Dental implants, Emergence profile, Natural tooth splinting
I. Introduction
Implant prostheses are ideal when they are in harmony with the surrounding soft tissue profile and imitate natural teeth1. This is even more important when the missing tooth to be replaced in the anterior area. The extraction of tooth usually results in change and collapse of the soft tissue, sometimes resulting in improper soft tissue profile2. Hence, the preservation or improvement of the existing soft tissue profile is important for implant restoration in the esthetic region. Provisional implant restorations enable to modify soft tissue profile1-6 at implant placement, at implant exposed, and even at the definitive impression process6-8. Emergence profile transfer technique is a method of transferring the profile of the provisional implant prosthesis to the definitive cast for the fabrication of a definitive prosthesis with proper emergence profile and contour9.
A 39-year-old male patient visited to the KyungHee University Dental Hospital with periapical abscess in the right maxillary central incisor. After clinical and radiographic examination, the tooth was planned to be extracted. The patient didn’t want to prepare the additional adjacent teeth. The right maxillary central incisor was planned to restore implant restoration and the left maxillary central incisor decided to proceed re-endodontic treatment and crown restoration (Fig. 1). Because of relatively young age of the patient, there was a lot of interest in esthetic results. Therefore, we planned to make provisional implant restoration and make a definitive prosthesis duplicating the emergence profile of the provisional restoration, and planned to use zirconia abutment when restoring the definitive prosthesis. First, preparation of maxillary left central incisor was done and maxillary right central incisor was extracted and cantilever provisional restoration was restored (Fig.
2, 3). Re-endodontic treatment of maxillary left central incisor was also progressed. After 3 months
Fig. 1. Pre-operative periapical radiograph on first visit.
Seoung-Jin Hong et al. : Anterior Restoration Splinting Implant with Natural Tooth: A Clinical Report. Implantology 2017
Fig. 2. Maxillary left incisor was prepared after extraction of maxillary right central incisor.
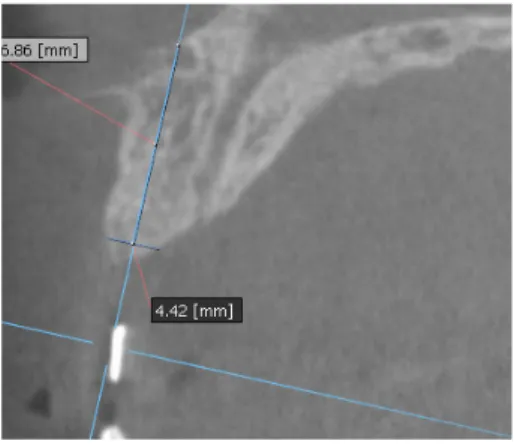
healing periods, implant placement was planned under evaluation of cone beam computed tomography scan with radiographic stent (Fig. 4). Implant placement was guided by surgical stent with bone graft (Bio-oss, Geistlich Pharma AG, Wolhusen, Switzerland) (Fig. 5, 6) and there were no systemic diseases would become problematic for implant surgery. Clinical and radiographic evaluation neither described any obvious active infection. Internal submerged type implant (4.0
Fig. 4. CT was taken.
Seoung-Jin Hong et al. : Anterior Restoration Splinting Implant with Natural Tooth: A Clinical Report. Implantology 2017
Fig. 5. Implant placement using surgical guide.
Fig. 3. Cantilever type provisional prostheses was delivered.
Seoung-Jin Hong et al. : Anterior Restoration Splinting Implant with Natural Tooth: A Clinical Report. Implantology 2017
mm×12.0 mm Implantium, Dentium, Korea) was placed and healing abutment was tightened. After surgery, provisional restoration was modified (Fig. 7). 3 months after implant surgery, fixture level impression was taken using pick-up impression coping (DPU 40 15 HL, Dentium, Korea) for provisional restoration (Fig. 8). Then, provisional crown with plastic provisional abutment (RAB 45 20 PHL, Dentium, Korea) was set for gingival molding (Fig. 9). During 3 weeks of provisional restoration period, the patient was satisfied with the function and the appearance of the provisional
Fig. 6. Bone graft after implant placement.
Seoung-Jin Hong et al. : Anterior Restoration Splinting Implant with Natural Tooth: A Clinical Report. Implantology 2017
Fig. 7. Correction of the cantilever type provisional prosthesis.
Seoung-Jin Hong et al. : Anterior Restoration Splinting Implant with Natural Tooth: A Clinical Report. Implantology 2017
Fig. 8. Pick-up impression for provisional restoration.
restoration. To transfer the emergence profile of provisional restoration, transfer technique was used with polyvinylsiloxane impression material (Silagum, light body and putty, GmbH, Germany) (Fig.
10) and impression coping was modified. The final fixture level impression was taken using polyvinylsiloxane impression material (Express light body and regular body, 3M ESPE, St Paul, MN, USA) after connection of modified pick-up impression coping (Fig. 11). A CAD/CAM zirconia abutment was milled and abutment adapted. Resin material (Pattern Resin LS; GC, America) and
Fig. 9. Gingival shaping with provisional prosthesis.
Seoung-Jin Hong et al. : Anterior Restoration Splinting Implant with Natural Tooth: A Clinical Report. Implantology 2017
Fig. 10. Emergence profile of implant provisional prosthesis was transferred.
Seoung-Jin Hong et al. : Anterior Restoration Splinting Implant with Natural Tooth: A Clinical Report. Implantology 2017
Fig. 11. Customized impression coping.
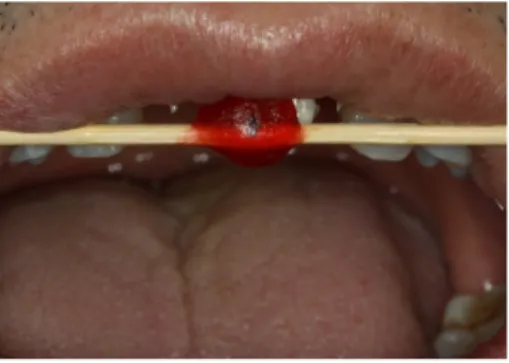
wooden sticks were used for delivery to laboratory of anterior teeth horizontal line. Midline also marked (Fig. 12). Splinted porcelain fused to zirconia prosthesis was fabricated. The root of the maxillary left central incisor being short and the prognosis being poor, so the crown was splinted with the maxillary right maxillary incisor implant prosthesis. The definitive crown and abutment were delivered to patient (Fig. 13). The esthetic, marginal fit was evaluated and the zirconia abutment was tightened to 30 Ncm using torque controller and splinted maxillary right and left definitive prostheses was set final cementation with resin-modified glass ionomer cement (FujiCEMTM, GC, Japan). Within the 3 years follow-up after treatment, the patient satisfied with the functional and esthetic outcomes, and the gingival architecture preserved that form.
III. Discussion
In some cases, clinicians may not be able to connect a provisional prosthesis immediately after Fig. 12. Horizontal line and midline are marked.
Seoung-Jin Hong et al. : Anterior Restoration Splinting Implant with Natural Tooth: A Clinical Report. Implantology 2017
Fig. 13. Splinted prosthesis was delivered.
Seoung-Jin Hong et al. : Anterior Restoration Splinting Implant with Natural Tooth: A Clinical Report. Implantology 2017
gingival contouring10. Relatively narrow healing abutment may results in improper soft tissue profile, usually larger than healing abutment, but proper emergence profile of a definitive restoration is placed. Whereby soft tissue complications result from placing a definitive restoration with a larger emergence profile compared with a relatively narrow healing abutment. Because, definitive restoration with the wider diameter may inflict pressure on thick soft tissue around the prosthesis9. Clinicians fabricate definitive restorations with proper soft tissue contours with this technique where a provisional prosthesis was not placed immediately after implant placement or uncovering, but at the final impression session. Even though appointment time at the definitive impression procedure may slightly increase because the modified impression coping is fabricated, this technique may minimize the patient’s soft tissue complications by staged contouring of the soft tissues11. Spyropoulou et al.5 and Schoenbaum et al.12 used emergence profile transfer technique by direct adding autopolymerized acrylic resin, quickly around the impression coping tightened on the implant. However, the patient’s discomfort and irritation of the peri-implant tissue could be increased by this direct adding technique. This alternative impression method is suitable for sensitive patients, who are easy to soft tissue change and to the irritation generated by the monomer and the heat caused by the autopolymerized acrylic resin. A limitation of this technique waiting time while the modifying impression coping.
Originally, the Branemark protocol13 for dental implant recommended that dental implants should be functioned independently from natural teeth due to the difference in biomechanics. In fact, natural teeth have a much larger physiological mobility than implants, which are rigidly ankylosed to bone.
Natural teeth with a healthy periodontium demonstrate a mobility of about 50-200 µm whenever a force of 0.1 N is applied14. On the other hand, mobility of an osseointegrated dental implant is less than 10 µm upon similar forces15. In some cases, however, the splinting of a natural tooth with an implant seems inevitable. Several studies have described clinical cases where fixed partial dentures are restored with a connection between implants and natural teeth16,17. These studies indicated the possibility of splinting implants to natural teeth in a fixed partial denture with a relatively good prognosis. In some studies have showed the good long-term prognosis of connecting implants to natural teeth18,19. In this case report, natural tooth restoration was splinted with implant restoration.
This resulted in a favorable prognosis for both implant and natural tooth, providing adequate support and stability.
References
1. Al-Harbi SA. Nonsurgical management of interdental papilla associated with multiple maxillary anterior implants: a clinical report. J Prosthet Dent. 2005; 93(3): 212-216.
2. Suda N, Huang L, Machida Y. Contour changes and growth and development of the alveolar ridge following multi-extractions of the maxillary deciduous incisors. Shikwa Gakuho. 1984; 84(10): 1737- 1745.
3. Kan JY, Rungcharassaeng K, Lozada J. Immediate placement and provisionalization of maxillary anterior single implants: 1-year prospective study. Int J Oral Maxillofac Implants. 2003; 18(1): 31-39.
4. Al-Harbi SA, Edgin WA. Preservation of soft tissue contours with immediate screw-retained provisional implant crown. J Prosthet Dent. 2007; 98(4): 329-332.
5. Spyropoulou PE, Razzoog M, Sierraalta M. Restoring implants in the esthetic zone after sculpting and capturing the periimplant tissues in rest position: a clinical report. J Prosthet Dent. 2009; 102(6):
345-347.
6. Ntounis A, Petropoulou A. A technique for managing and accurate registration of periimplant soft tissues. J Prosthet Dent. 2010; 104(4): 276-279.
7. Shimizu H, Namikawa H. The body plan of the cnidarian medusa: distinct differences in positional origins of polyp tentacles and medusa tentacles. Evol Dev. 2009; 11(6): 619-621.
8. Yilmaz B, McGlumphy E, Purcell B. An alternative direct technique for the fabrication of an implant- supported, screw-retained fixed interim restoration. J Prosthet Dent. 2012; 107(2): 137-139.
9. Gava R, Beltrami GC, Grezzana L. Metoxibutropate. G Clin Med. 1989; 70(10): 619-620.
10. Son MK, Jang HS. Gingival recontouring by provisional implant restoration for optimal emergence profile: report of two cases. J Periodontal Implant Sci. 2011; 41(6): 302-308.
11. Santosa RE. Provisional restoration options in implant dentistry. Aust Dent J. 2007; 52(3): 234-242;
quiz 54.
12. Schoenbaum TR, Han TJ. Direct custom implant impression copings for the preservation of the pontic receptor site architecture. J Prosthet Dent. 2012; 107(3): 203-206.
13. Branemark PI, Hansson BO, Adell R, et al. Osseointegrated implants in the treatment of the edentulous jaw. Experience from a 10-year period. Scand J Plast Reconstr Surg Suppl. 1977; 16: 1-132.
14. Borszewski J. Two cases of giant myomas of the stomach. Pol Tyg Lek (Wars). 1951; 6(29-30): 920-924.
15. Cohen SR, Orenstein JH. The use of attachments in combination implant and natural-tooth fixed partial dentures: a technical report. Int J Oral Maxillofac Implants. 1994; 9(2): 230-234.
16. Kay HB. Free-standing versus implant-tooth-interconnected restorations: understanding the prosthodontic perspective. Int J Periodontics Restorative Dent. 1993; 13(1): 47-69.
17. Weinberg LA. The biomechanics of force distribution in implant-supported prostheses. Int J Oral Maxillofac Implants. 1993; 8(1): 19-31.
18. Chee WW, Mordohai N. Tooth-to-implant connection: a systematic review of the literature and a case report utilizing a new connection design. Clin Implant Dent Relat Res. 2010; 12(2): 122-133.
19. Lang NP, Pjetursson BE, Tan K, et al. A systematic review of the survival and complication rates of fixed partial dentures (FPDs) after an observation period of at least 5 years. II. Combined tooth--implant- supported FPDs. Clin Oral Implants Res. 2004; 15(6): 643-53.