REPO RT
Int J Thyroidol 2017 November 10(2): 127-132 https://doi.org/10.11106/ijt.2017.10.2.127Received August 2, 2017 / Revised 1st September 22, 2017, 2nd November 6, 2017 / Accepted November 10, 2017 Correspondence: Dohee Kim, MD, PhD, Division of Endocrinology, Department of Internal Medicine, Dankook University College of Medicine, 119 Dandae-ro, Dongnam-gu, Cheonan 31116, Korea
Tel: 82-41-550-3934, Fax: 82-41-556-3256, E-mail: [email protected]
Copyright ⓒ 2017, the Korean Thyroid Association. All rights reserved.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creative- commons.org/licenses/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Anaplastic Transformation of Follicular Thyroid Cancer in the Lung, Liver, Bone, and Adrenal Gland
Wonae Lee
1and Dohee Kim
2,3Departments of Pathology1, Internal Medicine2, Dankook University College of Medicine, Department of Kinesiologic Medical Science, Graduate, Dankook University3, Cheonan, Korea
Anaplastic transformation of differentiated thyroid cancer at distant metastatic sites is extremely rare and has a poor prognosis. It usually occurs in the thyroid gland or cervical lymph nodes. Here we report a case of anaplastic transformation arising at multiple distant metastatic sites including the lung, liver, adrenal gland, bone, and lymph nodes in a patient 3 years after total thyroidectomy for follicular thyroid cancer.
Key Words: Cell transformation, Neoplastic, Thyroid carcinoma, Anaplastic, Thyroid cancer, Follicular, Thyroid cancer, Papillary
Introduction
Anaplastic thyroid carcinoma (ATC) is a rare but highly lethal form of thyroid cancer.1) ATC can arise de novo or, more commonly, through anaplastic transformation (or dedifferentiation) of preexisting dif- ferentiated thyroid cancer (DTC), including papillary thyroid carcinoma (PTC) or follicular thyroid carcinoma (FTC). Anaplastic transformation primarily occurs in the thyroid gland or in the cervical lymph nodes and less often in distant metastatic sites.2-6)
Here we report a very rare case of anaplastic transformation arising at multiple distant metastatic sites including the lung, liver, adrenal gland, bone, and lymph nodes in a patient 3 years after total thyroi- dectomy for FTC.
Case Report
A 72-year-old man was admitted on July 2015 with aggravated cough and sputum lasting 1 month, which had been unresponsive to medical treatment in a local clinic. He also had left-sided chest discomfort, fatigue, and poor oral intake. He underwent total thy- roidectomy with central neck dissection due to a growing bulky thyroid mass on April 2012. Macrosco- pic examination revealed a huge, partly encapsulated but overtly infiltrative solid tumor, which occupied al- most the entire left lobe and isthmus. The tumor measured approximately 7.5 cm at its widest point.
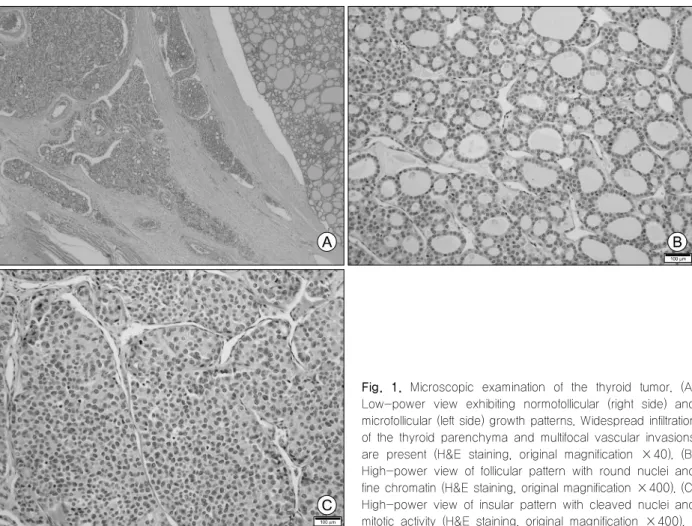
The cut surface of the tumor was fleshy, firm, and tan white with a large area of cystic infarct. Microscopic examination revealed a variety of architectural patterns from area to area, including normofollicular, micro- follicular, trabecular, and insular patterns (Fig. 1A). No
Fig. 1. Microscopic examination of the thyroid tumor. (A) Low-power view exhibiting normofollicular (right side) and microfollicular (left side) growth patterns. Widespread infiltration of the thyroid parenchyma and multifocal vascular invasions are present (H&E staining, original magnification ×40). (B) High-power view of follicular pattern with round nuclei and fine chromatin (H&E staining, original magnification ×400). (C) High-power view of insular pattern with cleaved nuclei and mitotic activity (H&E staining, original magnification ×400).
papillary structures were noted. The majority of the tu- mor cells was cuboidal and had round to ovoid nuclei with relatively fine chromatin and inconspicuous nu- cleoli (Fig. 1B). Mitotic figures were infrequently noted.
The tumor contained a minor component showing more serious atypia such as an insular pattern, cleaved nuclei, and occasional mitotic figures (Fig.
1C). The tumor revealed widespread extension to the thyroid parenchyma, perithyroidal soft tissue, and subcutaneous soft tissue. Multiple foci of vascular in- vasion were also present (Fig. 1A). No lymph node metastasis was noted. A diagnosis of widely invasive follicular carcinoma was made. He has been taking a daily dose of 0.15 mg of levothyroxine since the sur- gery and calcitriol and calcium carbonate for post- operative hypoparathyroidism. A radioactive iodine (RAI) ablation (150 mCi [5.5 GBq] of 131I) was administered 4 months after the surgery (August 2012). A post- therapeutic whole-body scan (RxWBS) revealed no
uptake at the neck but functioning metastases to the sternum and both lungs (Fig. 2A), consistent with the findings of positron emission tomography-computed tomography (PET-CT), which was performed before the surgery (Fig. 2B). A stimulated serum thyroglobulin level was 53,980 ng/mL with a thyrotropin (TSH) level 51.71 mIU/L (0.25-4.0) with negative anti-thyro- globulin antibody. He had then been treated with ster- num excision for sternum metastasis on August 2013 and two additional rounds of RAI therapy for multiple lung metastasis on April 2013 (150 mCi of 131I) and January 2014 (200 mCi of 131I). The last RxWBS showed significantly decreased uptake in the sternum and both lungs (Fig. 2A), and his stimulated serum thyroglobulin level decreased to 14,170 ng/mL.
Thereafter, his unstimulated serum thyroglobulin level increased from 3,786 ng/mL to 12,380 ng/mL 3 months and 1 year after the third RAI therapy, re- spectively (Fig. 3). We recommended additional RAI
Fig. 2. Follow-up of images during the clinical course. (A) Post-therapeutic whole body scan (RxWBS). The first RxWBS revealed no uptake at the neck but functioning metastases to the sternum and both lungs (left). The second RxWBS showed much improved metastases in both lungs compared with the first RxWBS (center). The third RxWBS showed significantly decreased uptake in the sternum (right). (B) Positron emission tomography-computed tomography (PET-CT) scan. The initial PET-CT revealed hypermetabolic lesions in the left thyroid lobe, sternal manubrium, and both lungs. The second PET-CT scan showed decreased extent and numeric changes of pulmonary nodules and no change in the sternum. The third PET-CT showed significantly decreased metabolic and extent change in the sternum. The last PET-CT scan on admission showed multiple hypermetabolic lesions in the lung; liver; left adrenal gland; along the whole body skeletal system; in and around the skin area in front of the sternum; and in the lymph nodes along the anterior mediastinal, left hilar, retrocaval, and left common iliac areas.
therapy, but he was reluctant to undergo it. Mean- while, he complained of pain at the surgical site of the sternum from bone cement bulging. The sternum was reconstructed on May 2015 and the surgical biopsy of excised soft tissue revealed only dense fibrosis with no evidence of malignancy. A chest X-ray showed no apparent metastatic nodules in the lung, and he did not complain of any symptoms. His condition was
good enough to travel with family until 1 month before admission.
On admission, laboratory investigations were within normal limits, but his unstimulated serum thyroglobulin level increased to 23,330 ng/mL. A chest X-ray showed a new large mass in the retrocardiac area of the left lower lung zone and several small nodular opacities in both lungs. The chest CT revealed a new
Fig. 4. Microscopic examination of the lung biopsy specimen. (A) Low-power view exhibiting diffuse infiltrate of anaplastic cells associated with extensive necrosis and acute inflammation (right side). There is a small focus of well-formed follicular architecture composed of well-differentiated follicular cells (left side) (H&E staining, original magnification ×100). (B) Higher magnification of anaplastic cells showing pleomorphic nuclei and macronucleoli (H&E staining, original magnification ×400).
Fig. 3. Follow-up of thyroglobulin levels during the clinical course. Thyroglobulin levels were greatly decreased after two surgeries and three rounds of RITx. However, thereafter, thyroglobulin levels continuously increased throughout the course. Ex: excision, RAITx: radioactive iodine therapy, TSH:
thyroid stimulating hormone, TT: total thyroidectomy heterogeneous enhancing irregular mass, approx- imately 6.4 cm in size abutting the mediastinal pleura in the left lower lobe suggesting metastasis or primary lung cancer and increased size and number of multi- ple small and tiny nodules in both lungs suggesting hematogenous metastases compared with previous CT. Additionally, newly enlarged lymph nodes in the left supraclavicular area and a few heterogeneous
enhanced masses in the sternal resection site of the upper anterior chest wall appeared, all suggesting metastases. Abdominal CT also showed two new low-density, heterogeneous enhanced masses in the liver and heterogeneous enhanced masses in left adrenal gland, approximately 1.2 cm and 2.8 cm in size, suggesting metastases. PET-CT showed a large, hypermetabolic lesion in the left lower lung and multi- ple hypermetabolic lesions in the liver, left adrenal gland, multiple whole-body skeletal areas including the sternum; multiple lymph nodes along the anterior mediastinum, left hilar, retrocaval, and left common iliac areas; and both lung fields (Fig. 2B). Fibrous tissue or necrotic endoluminal mass lesion was observed in the left lower posterior basal segmental bronchus by bronchoscopy, suspicious of bronchogenic carcinoma.
Bronchoscopic washing and biopsy showed only ne- crotic cells and extensive necrosis, respectively. CT- and fluoroscopy-guided percutaneous core needle biopsy was done for the left lower lung mass. The lung biopsy specimen showed diffuse infiltrate of anaplastic cells with single or multiple pleomorphic nuclei and macronucleoli (Fig. 4). Extensive coagulation necrosis and exuberant acute inflammation were present.
There was a minor component showing well-differ- entiated follicular cells arranged in a normofollicular pattern. Immunohistochemically, pan-keratin (AE1/AE3)
and galectin-3 were expressed in both the anaplastic cells and the well differentiated follicular cells; how- ever, thyroid transcription factor-1 (TTF-1) and thyro- globulin were negative in the anaplastic cells and positive in the well-differentiated follicular cells. The di- agnosis of metastatic anaplastic carcinoma of thyroid origin was made. He was only treated with antibiotics for combined pneumonia and antitussives and an- algesics for cough and left-sided chest pain.
However, his general condition deteriorated soon after, and he ultimately died from respiratory failure 1 month after admission.
Discussion
ATC is an aggressive form of thyroid cancer with a poor prognosis; median survival time is only 5-6 months, and 1-year survival is approximately 20%. It accounts for 1.7% of all thyroid cancers.1) Although the pathogenesis of ATC remains unclear, anaplastic transformation from preexisting DTC has become a well-documented occurrence.2,5) In many cases (20- 90%), patients have a history of a previously resected DTC or an ATC with a coexisting DTC after a histo- logical examination.1,2,5) In addition, transitional zones between the differentiated and undifferentiated com- ponents or preserved immunohistochemical staining for thyroglobulin, TTF-1, and paired box protein Pax-8 (PAX-8) in staining in well-differentiated areas suggests the anaplastic transformation of preexisting DTC.1,5) The most common coexisting DTC is a well- differentiated PTC (often the tall cell variant) followed by the conventional or oncocytic (Hürthle cell) type FTC.1,2,5) Although anaplastic transformation of DTC most commonly occurs in the thyroid gland and re- gional lymph nodes,2-6) previous studies have re- ported limited cases of occurrence at distant meta- static sites, including the pelvis,3) retroperitoneum,4,7) lung,5,6,8-11) mandible,12) submandibular space,13) liver,14) breast,15) and shoulder.16) These cases reported ana- plastic transformation from PTC at distant metastatic sites with three exceptions. These three cases (in- cluding our patient) were from FTC.3,7) In these cases, development of anaplastic transformation ranged from
4 to 30 years after the primary diagnosis of DTC.3-16) Therefore, it should be noted that anaplastic trans- formation can occur in metastatic sites even after long-term follow-up.5) Autopsy studies have demon- strated that ATC is often widely metastatic at the time of death, with two or more metastatic sites found in the vast majority of cases (84%). The most common metastatic sites are the lungs (78%), followed by the intrathoracic lymph nodes (58%), neck lymph nodes (51%), pleura (29%), adrenal glands (24%), liver (20%), and brain (18%).4,10,17) Poor prognostic factors in pa- tients with ATC include the presence of acute symp- toms such as a tumor size >5 cm, distant metastases, and leukocytosis in addition to male gender, age >60 years, and the presence of extrathyroidal involve- ment.1,3,4)
Advances in molecular technologies have aided the understanding of the molecular pathogenesis of poorly differentiated thyroid cancer (PDTC) and ATC by sug- gesting a stepwise tumoral progression. This pro- gression begins with well-differentiated cells, which turn into poorly differentiated cells, and finally, the de- velopment of ATCs.18,19) While BRAF and RAS muta- tions are the main drivers of aggressive thyroid carci- noma, ATCs have a greater mutational burden. This burden includes a higher frequency of mutations in TP53, the TERT promoter, the PI3K/AKT/mTOR path- way effectors, SWI/SNF subunits, and histone methyl- transferases compared with PDTCs. ATC is also char- acterized by genomic complexity and profound un- differentiation.18,19) In addition, RI therapy has been as- sociated with an increase in the probability of ana- plastic transformation of DTC.5,14,20) Sera et al.20) ex- amined 32 DTC patients with distant metastasis and followed up for 10 years or until death. The authors reported that ineffective 131I therapy to show insufficient accumulation of 131I might trigger early anaplastic changes via a p53 gene mutation with poor pro- gnosis. Postoperative 131I therapy was performed in 11 of 15 cases including ours.3-8,10,12,14,16) However, fur- ther studies are needed as it remains unclear whether
131I therapy is associated with the pathogenesis of anaplastic transformation.5)
In conclusion, we report a case of anaplastic trans-
formation of FTC in multiple distant metastatic sites in- cluding the lung, liver, adrenal gland, multiple skeletal areas, and lymph nodes over a very short time period during simultaneous treatment for FTC which demon- strated a relatively stable clinical course. Although this event is extremely rare, clinicians should be aware of the possibility of anaplastic transformation of DTC in distant metastatic sites. Active surveillance and long- term follow-up are imperative in high-risk patients because DTC is characterized by exceptionally rapid progression with a dire prognosis and drastically af- fects the treatment modality and prognosis.
References
1) Smallridge RC, Ain KB, Asa SL, Bible KC, Brierley JD, Burman KD, et al. American Thyroid Association guidelines for management of patients with anaplastic thyroid cancer. Thyroid 2012;22(11):1104-39.
2) Wiseman SM, Loree TR, Rigual NR, Hicks WL Jr, Douglas WG, Anderson GR, et al. Anaplastic transformation of thyroid cancer: review of clinical, pathologic, and molecular evidence provides new insights into disease biology and future therapy.
Head Neck 2003;25(8):662-70.
3) Nakayama R, Horiuchi K, Susa M, Hosaka S, Hayashi Y, Kameyama K, et al. Anaplastic transformation of follicular thyroid carcinoma in a metastatic skeletal lesion presenting with paraneoplastic leukocytosis. Thyroid 2012;22(2):200-4.
4) Solomon JP, Wen F, Jih LJ. Anaplastic transformation of papillary thyroid cancer in the retroperitoneum. Case Rep Pathol 2015;2015:241308.
5) Abe T, Suzuki M, Shimizu K, Shinagawa N, Oizumi S, Matsuno Y, et al. Anaplastic transformation of papillary thyroid carcinoma in multiple lung metastases presenting with a malignant pleural effusion: a case report. J Med Case Rep 2014;8:460.
6) Al-Qsous W, Miller ID. Anaplastic transformation in lung metastases of differentiated papillary thyroid carcinoma: an autopsy case report and review of the literature. Ann Diagn Pathol 2010;14(1):41-3.
7) Sotome K, Onishi T, Hirano A, Nakamaru M, Furukawa A, Miyazaki H, et al. A rare case of anaplastic transformation within the metastatic site of the retroperitoneal region in a patient 17 years after total thyroidectomy for papillary carcinoma of the thyroid beginning with multiple bone metastases. Thyroid
2007;17(12):1309-11.
8) Moore JH Jr, Bacharach B, Choi HY. Anaplastic transformation of metastatic follicular carcinoma of the thyroid.
J Surg Oncol 1985;29(4):216-21.
9) Khairy G. Anaplastic transformation of differentiated thyroid carcinoma. Int J Health Sci (Qassim) 2009;3(1):93-6.
10) Benedict M, Costa J. Metastatic papillary thyroid carcinoma with multifocal synchronous transformation to anaplastic thyroid carcinoma. Case Rep Pathol 2016;2016:4863405.
11) Kim JS, Moon HJ, Han JS, Kim MJ. Importance of regular follow-up examination during active surveillance: a case of anaplastic transformation of papillary thyroid microcarcinoma.
Int J Thyroidol 2016;9(2):185-9.
12) Ambelil M, Sultana S, Roy S, Gonzalez MM. Anaplastic transformation in mandibular metastases of follicular variant of papillary thyroid carcinoma: a case report and review of the literature. Ann Clin Lab Sci 2016;46(5):552-6.
13) Sumida T, Hamakawa H, Imaoka M, Okamoto N, Takarada M, Tanioka H, et al. A case of submandibular malignant rhabdoid tumor transformed from papillary thyroid carcinoma.
J Oral Pathol Med 2001;30(7):443-7.
14) Takeshita Y, Takamura T, Minato H, Misu H, Ando H, Yamashita T, et al. Transformation of p53-positive papillary thyroid carcinoma to anaplastic carcinoma of the liver following postoperative radioactive iodine-131 therapy. Intern Med 2008;
47(19):1709-12.
15) Angeles-Angeles A, Chable-Montero F, Martinez-Benitez B, Albores-Saavedra J. Unusual metastases of papillary thyroid carcinoma: report of 2 cases. Ann Diagn Pathol 2009;13(3):
189-96.
16) Kaushal S, Sharma MC, Mathur SR, Rastogi S, Bal CS, Chumber S. Anaplastic transformation of metastatic papillary thyroid carcinoma at shoulder mimicking soft tissue sarcoma.
Indian J Pathol Microbiol 2011;54(4):796-9.
17) Besic N, Gazic B. Sites of metastases of anaplastic thyroid carcinoma: autopsy findings in 45 cases from a single institution.
Thyroid 2013;23(6):709-13.
18) Xu B, Ghossein R. Genomic landscape of poorly differentiated and anaplastic thyroid carcinoma. Endocr Pathol 2016;
27(3):205-12.
19) Landa I, Ibrahimpasic T, Boucai L, Sinha R, Knauf JA, Shah RH, et al. Genomic and transcriptomic hallmarks of poorly differentiated and anaplastic thyroid cancers. J Clin Invest 2016;
126(3):1052-66.
20) Sera N, Ashizawa K, Ando T, Ide A, Abe Y, Usa T, et al.
Anaplastic changes associated with p53 gene mutation in differentiated thyroid carcinoma after insufficient radioactive iodine (131I) therapy. Thyroid 2000;10(11):975-9.