Effectiveness and Safety of Korean Medicine for Trigeminal Neuralgia: A Case Report ※
Ji Min Bae
1, Dae Hun Kim
1, Byung Ryul Lee
2and Gi Young Yang
2,*1
Department of Acupuncture & Moxibustion, Pusan National University Korean Medicine Hospital
2
Department of Clinical Medicine, Pusan National University School of Korean Medicine
[Abstract]
Objectives : This study aims to report the effectiveness and safety of Korean medicine with thread embedding acupuncture in the treatment of trigeminal neuralgia (TN).
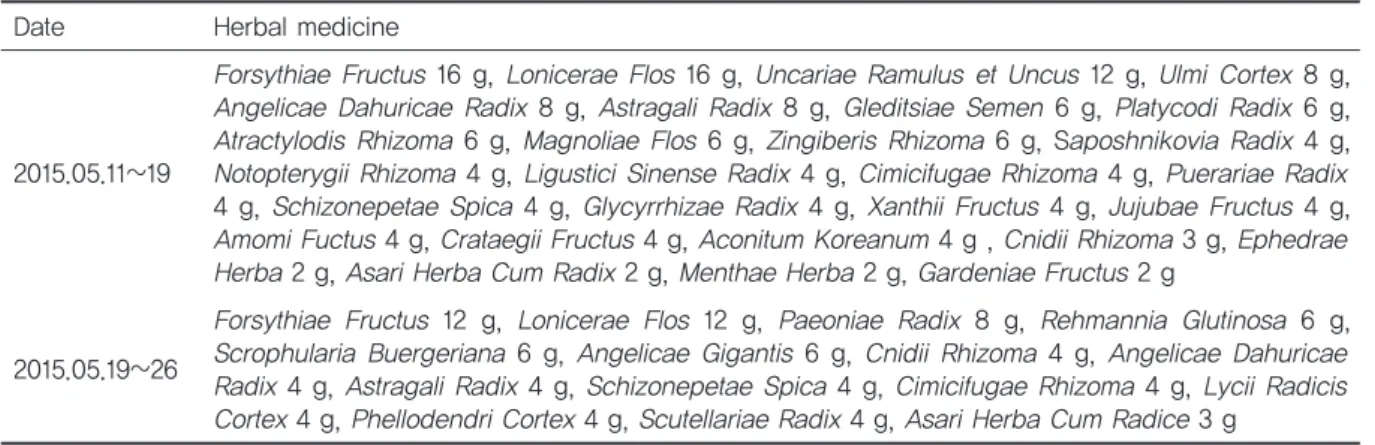
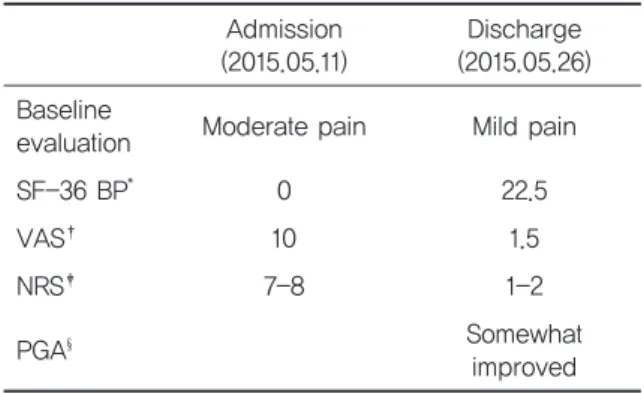
Methods : A 73-year-old man who had suffered from severe facial pain for one year and who had had a healthy tooth extracted due to the pain is reported. He could not eat or sleep due to the severe pain. Acupuncture, thread embedding acupuncture, cupping, herbal steam, and herbal medicines were used for the treatment. Numeric Rating Scale (NRS) and adverse events were checked daily, and other outcomes (Baseline Evaluation, Visual Analogue Scale [VAS], Short Form Health Survey 36-Bodily Pain [SF-36 BP], and Patient Global Assessment [PGA]) were measured at hospital admission and discharge. During the follow-up examinations, his pain was evaluated roughly, without using any formal measurements, on the basis of a global assessment.
Results : All measured parameters, including pain, quality of life, and patient satisfaction were noted to have improved at the time of discharge compared to admission: VAS from 10 to 1.5, NRS from 7–8 to 1–2, and SF-36 BP from 0 to 22.5, and the patient’s global assessment was somewhat improved. He did not take any analgesics after discharge and noted only mild ad- verse events, like pain where the acupuncture and thread embedding acupuncture needles were inserted. His pain relief was maintained for 6 months.
Conclusion : Korean medicine with thread embedding acupuncture might be a safe and effective treatment for TN. In the future, larger sample sizes and high quality randomized clinical trials are warranted to confirm its efficacy and safety.
※ This work was supported by clinical research grant from Pusan National University Hospital in 2016.
✱ Corresponding author : 20 Geumo-ro, Mulgeum-eup, Yangsan, Gyeongnam 50612, Republic of Korea
Tel : +82-55-360-5963 E-mail : [email protected] Key words :
Korean medicine;
Thread Embedding acupuncture;
Trigeminal neuralgia
Received : 2017. 01. 24.
Revised : 2017. 02. 02.
Accepted : 2017. 02. 03.
On-line : 2017. 02. 20.
This is an Open-Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by- nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.