Downloadedfromhttp://journals.lww.com/ijobyBhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdgGj2MwlZLeI=on04/26/2021
Downloadedfrom http://journals.lww.com/ijoby BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdgGj2MwlZLeI=on
04/26/2021
November 2020 Photo Essay 2507
Discussion
TSC is a rare phakomatosis characterized by multiple systemic hamartomas. It is inherited as autosomal dominant disorder with high penetrance and variable phenotypic expression.[2]
RAH are primary ophthalmic features of TSC.[3] RAH are noted as subtle greying of retina and are often missed unless carefully searched. It can manifest morphologically as (a) translucent flat tumors, (b) whitish nodular (mulberry lesion) mass or (c) Mixed variety.[4] Dilated fundus evaluation is a simple and cost-effective way to clinically diagnose such disorders before other invasive investigations are undertaken to confirm TSC.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Northrup H, Krueger DA, Roberds S, Smith K, Sampson J, Korf B, et al. Tuberous sclerosis complex diagnostic criteria update:
Recommendations of the 2012 International Tuberous Sclerosis Complex Consensus Conference. Pediatr Neurol 2013;49:243-54.
2. Schwartz RA, Fernandez G, Kotulska K, Jozwiak S. Tuberous sclerosis complex: Advances in diagnosis, genetics, and management. J Am Acad Dermatol 2007;57:189-202.
3. Rowley SA, O’Callaghan FJ, Osborne JP. Ophthalmic manifestations of tuberous sclerosis: A population based study. Br J Ophthalmol 2001;85:420-3.
4. Kandt RS. Tuberous sclerosis complex and neurofibromatosis type 1: The two most common neurocutaneous diseases. Neurol Clin 2002;20:941-64.
Department of Ophthalmology, Keimyung University School of Medicine, Dongsan Medical Center, South Korea
Correspondence to: Dr. Yu Cheol Kim, Department of Ophthalmology, Keimyung University School of Medicine, 1095 Dalgubeol-daero, Dalseo-gu, Daegu, 42601, Republic of Korea. E-mail: [email protected] Received: 29-May-2020 Revision: 18-Jun-2020
Accepted: 21-Jul-2020 Published: 26-Oct-2020
Cite this article as: Lee JK, Kim YC. Bilateral isolated choroidal melanocytosis with hypopigmented posterior pole. Indian J Ophthalmol 2020;68:2507-9.
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution‑NonCommercial‑ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non‑commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
For reprints contact: [email protected] Access this article online
Quick Response Code: Website:
www.ijo.in DOI:
10.4103/ijo.IJO_1731_20 PMID:
*****
B i l a t e r a l i s o l a t e d c h o r o i d a l melanocytosis with hypopigmented posterior pole
Jae Kyoung Lee, Yu Cheol Kim
Key words: Choroidal melanocytosis, hyperpigmentation, hypopigmentation
The presence of choroidal melanocytic hyperpigmentation without any associated scleral or skin pigmentation was first defined by Ausburger et al.[1] as “isolated choroidal melanocytosis”
in 11 Caucasian individuals. Isolated choroidal melanocytosis must be evaluated closely; the differential diagnoses include ocular or oculodermal melanocytosis, choroidal nevus,
melanoma, bilateral diffuse uveal melanocytic proliferation, and systemic conditions, such as Waardenburg syndrome. Only a few cases have been reported since,[2,3] and most reports focused mainly on choroidal hyperpigmentation itself, concentrating on the range, shape, and bilaterality of pigmentation. Herein, we present a unique case of bilateral isolated choroidal melanocytosis with hypopigmented posterior pole.
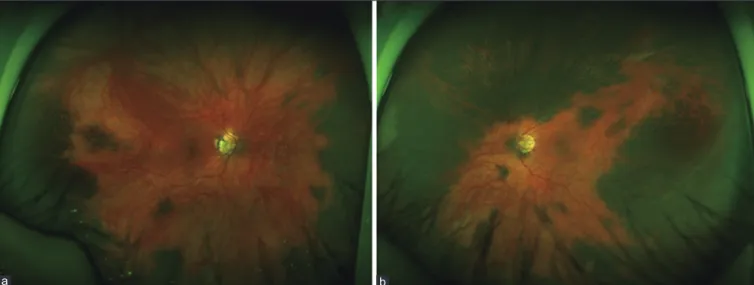
Ultrawide-field color photographs [Fig. 1] showed central hypopigmentation with peripheral choroidal hyperpigmentation around the 360° field in both eyes.
Due to the depigmentation, both posterior fundi appeared yellow-orange as in Vogt-Koyanagi-Harada disease. Fluorescein angiography [Fig. 2] and fundus autofluorescence [Fig. 3] were normal and no hyperfluorescence was found in pigmented lesions. Optical coherence tomography [Fig. 4] showed normal structures of the retinal pigment epithelial layer, choroid, and retina. Given the rarity of hypopigmentation among Asians, our case is unique, as peripheral choroid hyperpigmentation and central hypopigmentation existed simultaneously.
Discussion
Two possible hypothetical explanations can be proposed for our patient’s funduscopic findings. Autoimmunity offers one explanation. Similar to what is seen in Vogt-Koyanagi-Harada disease, choroidal hyperpigmentation may have triggered
2508 Indian Journal of Ophthalmology Volume 68 Issue 11
Figure 2: Fundus fluorescein angiography of the 102°‑field (a: right eye, b: left eye) and 55°‑field (c: right eye, d: left eye) showing a normal angiographic pattern
a b
c d
Figure 1: Ultrawide‑field color photographs of the right (a) and left (b) eyes show peripheral, flat, and diffuse choroidal hyperpigmentation around the 360° field
a b
an autoimmune response to melanocytes, leading to hypopigmentation at the posterior pole. Another possibility is racial differences in choroidal pigmentation and melanoma incidence. Hypopigmented fundus and choroidal melanoma are more prevalent among Caucasians than Asians.[4] Our patient may have pigmentary features similar to that of Caucasians;
therefore, hyperpigmentation and hypopigmentation could coexist.
Moreover, choroidal melanocytosis may be a risk factor for malignancy,[5] similar to ocular or oculodermal melanocytosis.
Our case highlights the need for further research to better understand this condition.
Financial support and sponsorship Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Augsburger JJ, Trichopoulos N, Correa ZM, Hershberger V. Isolated choroidal melanocytosis: A distinct clinical entity? Graefes Arch Clin Exp Ophthalmol 2006;244:1522-7.
2. Fine HF, Brue C, Eandi C, Jacobs MI, Pulitzer M, Yannuzzi LA.
Bilateral isolated choroidal melanocytosis. Retin Cases Brief Rep 2009;3:272-4.
Figure 3: Fundus autofluorescence images of the right (a) and left (b) eyes reveal normal autofluorescence distribution but vitreous floaters are detected
a b
Figure 4: Color fundus photographs and optical coherence tomography images of the right (a) and left (b) eyes demonstrate hypopigmented fundus with normal retinal and choroidal structures
b a
November 2020 Photo Essay 2509 3. Heinz KD, Demirci H, Elner VM. Bilateral annular isolated choroidal
melanocytosis. Ophthalmic Surg Lasers Imaging Retina 2019;50:e74-e76.
4. Kaliki S, Shields CL, Shields JA. Uveal melanoma: Estimating prognosis. Indian J Ophthalmol 2015;63:93-102.
5. Shields CL, Kaliki S, Livesey M, Walker B, Garoon R, Bucci M, et al.
Association of ocular and oculodermal melanocytosis with the rate of uveal melanoma metastasis: Analysis of 7872 consecutive eyes.
JAMA Ophthalmol 2013;131:993-1103.
Department of Uvea, Medical Research Foundation, Chennai, Tamil Nadu, India
Correspondence to: Dr. Sudha K Ganesh, Department of Uveitis, Medical Research Foundation, No 18 College Road, Chennai - 600 006, Tamil Nadu, India. E-mail: [email protected]
Received: 11-Mar-2020 Revision: 18-May-2020 Accepted: 25-Jun-2020 Published: 26-Oct-2020
Recurrent posterior scleritis with secondary choroidal osteoma in a child
Nivedita Nair, Sharanya Abraham, Sudha K Ganesh
Key words: Choroidal osteoma, immunoglobulin G4 (IgG4) disease, posterior scleritis
Posterior scleritis common in adults is characterized by disc swelling, retinal striae and T-sign on ultrasound. Pediatric posterior scleritis is a rare entity. Choroidal osteoma (CO) may be secondary to inflammatory etiologies like idiopathic orbital inflammation and sclero-uveitis.
A 12-year old boy, presented with intermittent dull aching pain and decreased vision in the right eye (RE) for 3 years and was on systemic steroid therapy. Fundus photographs taken 6 months back revealed an elevated choroidal lesion superior, nasal and temporal to the optic disc [Fig. 1a] with hyperfluorescence and delayed staining on the corresponding fluorescein angiogram (FA) [Fig. 1b and c] and T-sign on B-scan ultrasound (USG) [Fig. 2].
We noted best-corrected visual acuity of 20/30 in RE and a nontender periorbital fullness superolaterally. The eye was quiet. The juxtapapillary choroidal lesion had decreased in size, with well-defined borders [Fig. 3a]. There was normal autofluorescence [Fig. 3b].
On FA, hyperfluorescence had resolved [Fig. 3c].
Indocyanine green angiogram showed hypocyanescence [Fig. 3d]. There was no T-sign on USG, but a high-reflective spike adjacent to the optic disc suggestive of calcification was
seen [Fig. 4]. Optical coherence tomography showed a thick hyper-reflective layered matrix [Fig. 5]. Serum IgG4 was raised (3.12 g/L reference 0.012–1.699). Mantoux, QuantiFERON TB-gold, RA, ANA, c and p ANCA were negative. The left eye was normal. Pediatric evaluation was normal. Oral steroids were tapered and regular ophthalmic and pediatric follow-up was advised.
Discussion
A diagnosis of recurrent posterior scleritis and “possible”
IgG4-related ophthalmic disease was considered based on recommended criteria.[1] The choroidal osteoma in our case appears to be secondary to inflammation-induced dystrophic ossification. Systemic surveillance was recommended as IgG4-related multifocal fibrosclerosis, pseudotumor, retroperitoneal fibrosis, autoimmune pancreatitis, and thyroiditis have been observed.[2,3]
IgG4-related ocular inflammation is characterized by IgG4 positive plasmacytic infiltration, fibrosis of the involved organs, and elevated serum IgG4 levels. Histopathology from tissue confirms the diagnosis.[1] While oral steroids are the first-line treatment in IgG4 disease, immunomodulators and Rituximab could be considered for recurrences.[4]
IgG4-related disease is an emerging diagnosis to consider in recurrent ocular inflammation. Early diagnosis prevents extensive investigations and multiple biopsies.
The unique association of two lesser known entities like secondary choroidal osteoma and IgG4 inflammatory disease with recurrent posterior scleritis is highlighted in this report.
Acknowledgement
We wish to acknowledge Dr. Santanu Mondal, Medical Retina
& Uvea Consultant, Disha Eye Hospital, Behala, Kolkata 700034, for some of the early clinical photographs.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published
Cite this article as: Nair N, Abraham S, Ganesh SK. Recurrent posterior scleritis with secondary choroidal osteoma in a child. Indian J Ophthalmol 2020;68:2509-11.
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution‑NonCommercial‑ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non‑commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
For reprints contact: [email protected] Access this article online
Quick Response Code: Website:
www.ijo.in DOI:
10.4103/ijo.IJO_521_20 PMID:
*****