부산대학교 의학전문대학원 안과학교실1, 이춘식 안과의원2, 메리놀병원 안과3
목적: 범위가 좁은 국소적 망막신경섬유층(RNFL) 결손 중 망막신경섬유층사진에서는 발견되지만 빛간섭단층촬영(OCT)에서는 발견되지 않는 경우들에 대해 분석해 보고자 하였다.
대상과 방법: 망막신경섬유층사진에서는 결손을 보이지만 OCT의 RNFL thickness average analysis에서는 발견되지 않았던 14눈(17 곳)을 대상으로 하여, OCT scan image 및 analysis image와 비교분석하였다.
결과: 10° 이하 범위의 망막신경섬유층 결손은 71.4%에서 OCT scan image부터 망막신경섬유층의 감소 부위가 보이지 않았다. 11∼
30° 범위의 결손은 모두 scan image에서는 망막신경섬유층의 감소 부위가 확인되었으나, 자동화된 컴퓨터 알고리즘에 의해 두께를 측정하는 과정인 analysis image에서는 감소 부위를 나타내지 못하였다.
결론: 국소적 망막신경섬유층 결손이 OCT로 발견하기 어려운 경우는 20° 이하가 대부분이었으며, 10° 보다 좁은 경우는 OCT scan 자체의 한계가, 11∼30° 범위의 결손은 RNFL thickness analysis 단계의 문제가 영향을 줄 것으로 생각된다.
<대한안과학회지 2009;50(4):558-564>
■ 접 수 일: 2008년 5월 28일 ■ 심사통과일: 2008년 11월 25일
■ 통 신 저 자: 제 승 연
부산시 중구 대청동 3가 9-1 이춘식 안과
Tel: 051-465-6761, Fax: 051-242-7341 E-mail: [email protected]
* 본 연구는 2009년도 부산대학교병원 임상연구비 지원으로 이루어졌음.
녹내장은 망막신경절세포의 점진적 소실과 망막신경섬유 층의 두께 감소에 기인하여 비가역적 시신경손상 및 시야 장애를 일으키는 진행성 질환이다.1,2그러나 초기에는 자각 증상이 없는 경우가 대부분이고 시야장애가 많이 진행한 말기에 이르러서야 시력저하 또는 시야협착의 증상이 나타 나며 시신경손상은 비가역적이기 때문에 조기진단과 예방 및 적절한 치료가 중요하다.
임상에서 녹내장성 손상은 안압측정, 시야검사, 시신경유두 및 망막신경섬유층 검사를 통해 진단하고 있다. 하지만 안압 측정은 정상안압녹내장의 조기발견에 도움을 주지 못하고, 시 신경유두 검사는 검사자에 따른 결과의 차이가 크며, 정상안 에서도 시신경유두 형태의 개인차가 심하므로 녹내장 초기환 자의 미세한 변화를 알기 어렵다.3또한 시야검사도 시신경축 삭의 손실이 상당히 진행된 후에야 시야결손이 나타나는 문제 점을 가지고 있어 녹내장의 조기진단에는 한계가 있다.4,5
녹내장의 진행에 있어 망막신경섬유층의 손상은 시신경 유두의 변화나 시야검사상 결손보다 먼저 발생한다고 알려져 있다.6-8 이러한 망막신경섬유층의 손상을 평가하기 위해 이전부터 무적색광안저촬영을 통한 망막신경섬유층사진이 이용되었으며 최근에는 망막신경섬유층의 두께를 측정하고
객관적으로 비교할 수 있는 기구로 빛간섭단층촬영기(OCT) 가 주로 사용되고 있다. 망막신경섬유층 사진은 망막신경섬 유층 결손을 발견하는 데는 유용한 도구이지만 평가 자체 가 주관적이고, 산동을 해야 한다는 단점과 함께 매질의 혼 탁이 있을 때는 진단의 한계가 있다.
반면에 OCT는 적외선 계열의 광선을 이용해 약 10 μm의 높은 해상력으로 B-scan과 유사하게 조직 내에서 반사되는 빛의 시간 차이를 광학적 간섭계를 사용하여 망막신경섬유 층의 두께를 정량적으로 측정하는 기구로써 국소적인 망막 신경섬유층 결손을 진단하는데 있어 민감도와 특이도가 아주 뛰어난 것으로 여러 연구에서 보고되고 있다.9-14그러나 망 막신경섬유층 결손이 망막신경섬유층사진에서는 확인되나 OCT에서는 발견되지 않는 위음성의 경우 그 원인분석에 대한 보고는 아직 없는 실정이다.
이에 저자들은 망막신경섬유층사진에서 국소적인 결손을 보이지만 OCT의 RNFL thickness average analysis에서는 결손이 발견되지 않았던 경우들의 원인을 분석하고자 하였다.
대상과 방법
2006년 5월부터 2007년 8월까지 본원 녹내장크리닉을 방문하여 병력, 시력 및 굴절검사, 안압측정, 세극등검사, 시야검사, 시신경 및 망막신경섬유층 사진촬영, 빛간섭단층 촬영을 시행한 환자 중 망막신경섬유층사진에서는 국소적인 결손을 보이지만 빛간섭단층촬영의 RNFL thickness ave- rage analysis에서는 결손이 발견되지 않았던 14눈을 대상
A B
RNFL THICKNESS AVERAGE ANALYSIS
OD
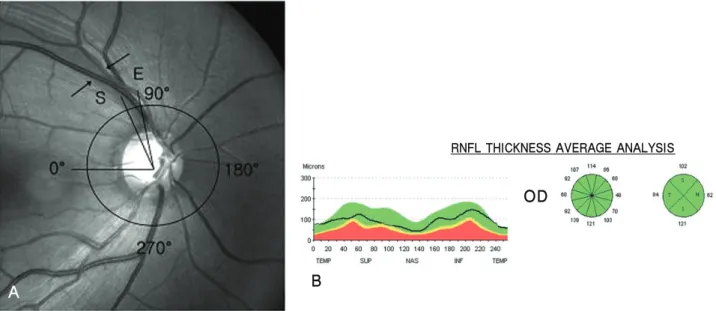
Figure 1.False negative findings of OCT and measurement of the location and width of RNFL defect on red-free fundus photograph. Localized, wedge-shaped RNFL defect was identified on red-free fundus photograph (A, arrows). But RNFL thickness throughout 360° (12 zones) were measured normally on RNFL thickness average analysis of OCT (B).
The diameter and the location of the circle were determined as they corresponded as closely as possible to the circle displayed in the fundus image of RNFL thickness report. A reference line was drawn horizontally through the center of the circle. The temporal meeting point of the line with the circle was set at 0°. The directional angle was assessed in a clockwise direction for right eyes and a counterclockwise direction for left eyes. The start (S) and end (E) points of each RNFL defect, where the borders of the defect met with the circle, were determined (A).
으로 하여 단면연구를 시행하였다. 병력상 다른 안질환이 있거나 안외상 및 안내수술의 과거력이 있는 경우는 대상 에서 제외하였다.
망막신경섬유층 사진은 먼저 환자의 눈에 1% tropicamide 와 2.5% phenylephrine을 점안하여 산동시킨 후 숙련된 1명 의 기술자가 VISUPAC-FF450plus IR (Carl Zeiss Meditec, Inc., Jena, Germany)을 이용하여 무적색광안저촬영을 시행 하였다.
국소적 망막신경섬유층 결손은 시신경유두와 연결되고 시신경유두에서 부채꼴 모양 또는 쐐기 모양으로 퍼져 나가는 형태이며 선모양이나 방추형(slit-like or spindle-like)이 아닌 형태로 정의하였다.
빛간섭단층촬영도 같은 방법으로 산동시킨 후 숙련된 1명의 기술자가 Stratus OCT (Carl Zeiss Meditec, Inc., Dublin, CA)를 이용하여 fast RNFL thickness 3.4 type으로 검사하였다. 기계 내부에서 조준광선이 깜박거리게 하여 주 시점에 검사하고자 하는 눈을 주시하도록 하는 대상안 내측 주시(internal fixation) 방법을 사용하여 안구를 고정시키고, 시신경유두 중심을 기준으로 직경 3.4 mm 지점의 망막신경 섬유층 두께를 측정하였다. 망막신경섬유층사진에서는 뚜 렷한 국소적인 결손이 보이지만 OCT의 RNFL thickness average analysis에서 결손부위에 해당하는 망막신경섬유
층의 두께가 정상범위의 5% 이상인 녹색 또는 흰색으로 나타날 때를 위음성으로 판정하였다(Fig. 1).
OCT의 위음성이 발견된 14눈을 대상으로 망막신경섬유 층 결손의 위치 및 범위를 결정하기 위해 망막신경섬유층 사진을 출력하였고 시신경유두를 중심으로 원을 그렸다. 원 의 크기와 위치는 OCT의 RNFL thickness report의 fundus image에 표시된 원을 참고하였다. 원의 중심에서 이측으로 직선을 그어 원과 만나는 점을 0°로 정하고, 상측을 90°, 비 측을 180°, 하측을 270°로 하였다. 결손의 경계가 원과 만 나는 시작과 끝점에서 원의 중심을 연결하여 결손의 위치 와 범위를 정하였다(Fig. 1).
OCT의 위음성의 원인을 알아보기 위해 망막신경섬유층 사진에서 발견되는 국소적인 결손의 위치에 해당하는 부 위를 RNFL thickness report의 OCT image의 동일한 위치 에 변환식을 사용하여 표시하였고 자동화된 컴퓨터 알고 리즘에 의해 두께를 측정하는 과정인 “layer on”이 되기 전인 scan image 및 “layer on”이 된 analysis image에서 결손의 인식유무를 각각 조사하였다(Fig. 2).
결 과
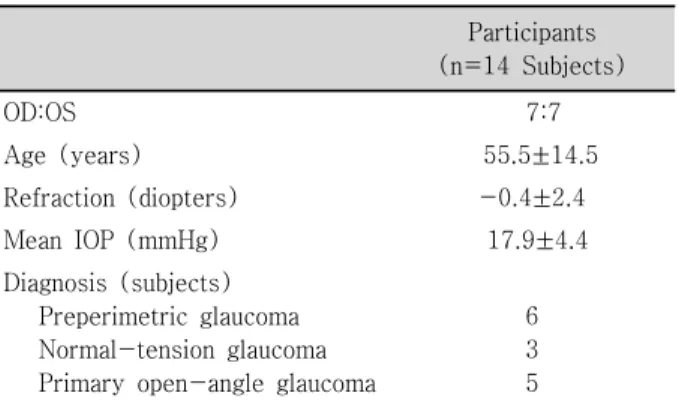
14눈 중 우안이 7눈(50%), 좌안이 7눈(50%)이었다.
A
B
C
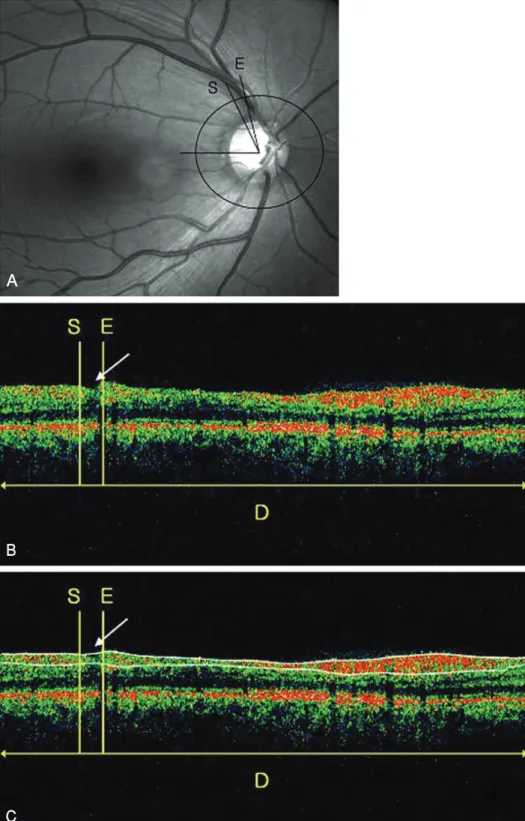
Figure 2. Analysis of causes about false negative response of OCT. (A) Localized RNFL defect was detected on red-free fundus photograph. The start (S) and end (E) points of RNFL defect were assessed as angular measure from 0° on reference line. The measured values were then converted to linear measures by multiplying by the result by D in millimeter and dividing 360°. (B) RNFL defects were identified in topographically matched region as a deflection on OCT scan image of RNFL thickness report (arrow). (C) RNFL defects were not indentified in topographically matched region on OCT analysis image of RNFL thickness report (arrow), which display the results of measuring the RNFL thickness as two white lines through automated computer algorithm, so-called “layer on”.
A
B
C
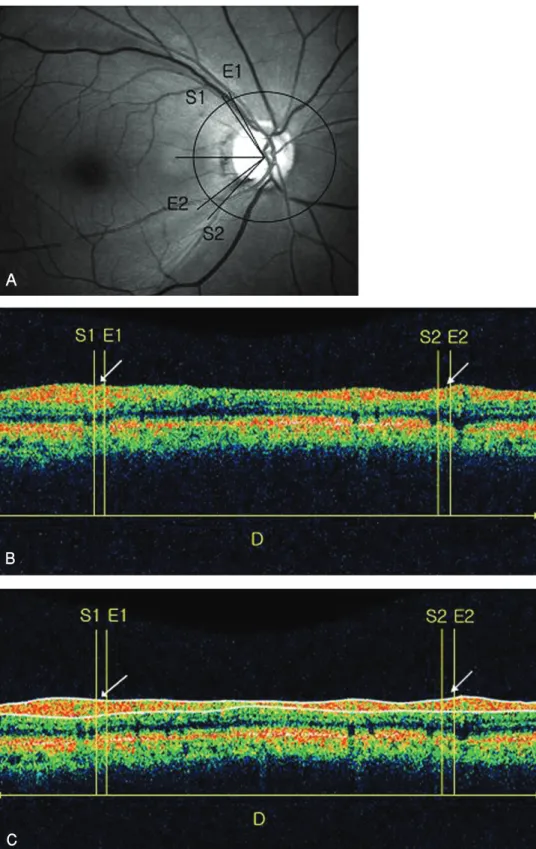
Figure 3. Analysis of causes about false negativeness of OCT. (A) Two localized RNFL defects were detected on red-free fundus photograph. The start (S1, S2) and end (E1, E2) points of RNFL defect were assessed as angular measure from 0° on the reference line. The measured values were then converted to linear measures by multiplying by the result by D in millimeter and dividing 360°. (B) RNFL defects were not already identified in topographically matched region as a deflection on OCT scan image of RNFL thickness report (arrow). (C) RNFL defects were not also indentified in topographically matched region on OCT analysis image of RNFL thickness report (arrow).
Mean IOP (mmHg) 17.9±4.4 Diagnosis (subjects)
Preperimetric glaucoma Normal-tension glaucoma Primary open-angle glaucoma
6 3 5
Location of RNFL defects No. of RNFL defects (%)
Superotemporal 9(52.9)
Inferotemporal 8(47.1)
Total 17(100)
Table 2. Location of localized RNFL defects detected by red-free fundus photography
Angular width of RNFL defects
No. of RNFL defects (%)
Causes of false negativeness of OCT (no. of RNFL defects)
≤10° 7(41.2) Scan (5), analysis (2)
11∼20° 8(47.0) Analysis (8)
21∼30° 2(11.8) Analysis (2)
Total 17(100) (17)
Table 3.Analysis of causes according to angular width of localized RNFL defects not detected by OCT
평균연령은 55.5±14.5세(26∼74세)였고 평균굴절력은 -0.4±2.4 diopters (-7.5∼+2.5 diopters)였으며 초진 당시 평균안압은 17.9±4.4 mmHg (14∼30 mmHg)였다.
14눈 중 시야결손 전 녹내장이 6눈, 정상안압녹내장이 3눈, 일차성 개방각녹내장이 5눈이었다(Table 1).
망막신경섬유층 사진을 분석한 결과 14눈 중 3눈(21.4%) 에서는 국소적 망막신경섬유층 손이 각각 2군데에서 발견 되어 총 17곳을 조사하였다. 망막신경섬유층 결손의 위치는 상이측이 9곳(52.9%), 하이측이 8곳(47.1%)으로 나타났 고(Table 2), 평균범위는 15.1±6.6° (7∼30°)였으며 10°
이하가 7곳(41.2%), 11∼20°가 8곳(47.0%), 21∼30°가 2곳(11.8%)이었다(Table 3).
OCT의 위음성의 원인을 알아보기 위해 RNFL thickness report의 OCT image를 분석한 결과 10° 이하 범위의 결손 은 7곳 중 5곳(71.4%)에서 “layer on”이 되기 전인 scan image부터 망막신경섬유층의 감소 부위가 보이지 않았다
손에 포함되어 있거나 인접해 있었다.
고 찰
녹내장과 그 진행의 진단은 시야결손을 동반하는 특징적 인 시신경유두의 변화를 포함하여 주관적으로 이루어진다.
시신경유두의 병적 변화는 시야결손에 선행하며, 시신경축 삭의 30~50%가 손상 받더라도 시야검사상 변화가 나타나 지 않는다.4,15 또한 망막신경섬유층의 두께 감소는 시야검 사상 결손과 시신경유두의 변화가 발견되기 전 녹내장성 손상의 민감한 척도라고 알려져 있다.6,7,16특히 Sommer et al6은 시야검사상 결손이 나타나기 6년 전에 환자의 60%에 서 망막신경섬유층의 결손이 있다고 보고하였다. 따라서 최 근에는 시야검사상 결손이 발견되기 전의 녹내장을 조기진 단하고 진행여부를 조기발견하는 방법으로 망막신경섬유층 의 두께를 측정하는 것에 대한 관심이 증대되어 왔다.
망막신경섬유층의 두께를 측정하는 기기로는 Heidelberg retina tomograph (HRT), Scanning laser polarimetry (SLP;
GDx-nerve fiber analyzer), Optical coherence tomograph (OCT) 등이 있는데 HRT는 주로 시신경유두의 형태 측정 에 이용되며, SLP는 망막신경섬유층이 복굴절을 일으키는 유일한 구조물이 아니기 때문에 오차가 발생될 수 있다는 단점이 있다.17,18
OCT는 840 nm의 적외선 계열의 레이저광선을 이용하여 망막에서 반사되어 나오는 빛의 정도에 따라 색깔을 다르 게 표시하여 망막의 단층면 영상을 얻을 수 있는 검사 장비 로써 최근 망막과 시신경유두의 다양한 질환을 조기진단하 는데 매우 유용하다고 알려져 있다.9또한 10 μm 정도의 우 수한 해상력으로 망막의 앞쪽 부분에 있는 망막신경섬유층 을 구분한 뒤 자동화된 컴퓨터 알고리즘에 의해 망막신경 섬유층의 두께를 정량화하여 위, 아래, 비측, 이측의 사분면 별 두께와 12분(clock hour)된 구획의 두께 및 전체 평균 두께를 구할 수 있다. 특히 망막신경섬유층 두께의 분석 시 자체적으로 정상과 정상범위를 벗어나는 경우 색깔로 구별 해주는 프로그램을 내장하고 있는데 붉은색은 망막신경섬 유층의 두께가 정상범위의 1% 미만인 경우, 노란색은 1%
이상 5% 미만인 경우, 녹색은 5% 이상 95% 이하인 경우 이며 95%를 초과하면 흰색으로 표시된다. 본 연구에서는
무적색광안저촬영을 통해 얻은 망막신경섬유층 사진에서는 뚜렷한 국소적인 결손이 보이지만 OCT의 RNFL thickness average analysis에서 그 결손부위에 해당하는 망막신경섬 유층의 두께가 정상범위의 5% 이상인 녹색 또는 흰색으로 나타날 때를 OCT의 위음성으로 판정하였다.
여러 장점으로 인해 최근까지 망막신경섬유층의 결손에 대해 OCT를 이용한 많은 연구가 보고되어 왔는데 Teesalu et al13은 녹내장 6눈을 대상으로 망막신경섬유층사진에서 보이는 망막신경섬유층 결손에 해당하는 지역을 선형으로 스캔하여 주위 정상 망막신경섬유층과 확연히 구분되어 신 호강도가 감소함을 관찰하였다. Zangwill et al19과 Soliman et al20은 OCT에서 측정된 망막신경섬유층의 두께 감소는 망막신경섬유층사진에서 나타나는 결손의 정도와 상당한 관련이 있다고 보고하였으며 최근 Hwang et al10은 OCT에 서 나타나는 국소적인 망막신경섬유층 결손의 위치와 범위 도 망막신경섬유층사진에서 나타나는 결손과 일치한다고 보고하였다.
또한 국소적인 망막신경섬유층의 결손을 발견하는데 있 어 OCT의 민감도와 특이도에 대한 많은 연구도 보고되었 는데 초기에 개발된 OCT를 사용한 Pieroth et al14은 민감 도와 특이도가 각각 65%와 81%로 보고하였고 본 연구에 서 사용된 Stratus OCT를 사용한 Jeoung et al11은 85.9%
와 97.4%로 향상된 결과를 보고하였으며 Budenz et al12도 비슷한 84%와 98%로 보고하였다. 하지만 이러한 연구에 서도 15%에 달하는 OCT의 위음성에 대한 분석은 없었다.
본 연구의 결과를 살펴보면 OCT에서 위음성으로 나타난 경우는 망막신경섬유층사진에서 나타난 결손의 평균범위가 15.1±6.6°로 모두 30° 이하였으며 그 중 88%가 20° 이하 였다. 특히 10° 이하 범위의 결손은 OCT scan 자체의 한계 로 인해 결손부위가 scan image상에 잘 보이지 않았고, 11
∼30° 범위의 결손은 OCT scan image에서는 결손이 보이 지만 RNFL thickness analysis 단계의 자동화된 컴퓨터 알 고리즘이 좁은 결손부위를 인식하지 못하고 뛰어 넘어 망 막신경섬유층이 정상적인 것처럼 두께를 잘못 측정하는 것 이 원인이었다. 그 외의 원인으로 본 연구에서는 조사되지 않았지만 망막신경섬유층 결손의 두께가 얇은 경우도 고려 될 수 있겠다. 저자들은 이런 요인들이 OCT의 민감도 감소 에 영향을 주는 것으로 생각한다. 또한 본 연구에서는 망막 의 혈관이 망막신경섬유층 결손에 포함되거나 인접한 경우 가 많았는데, 이러한 망막혈관이 OCT의 scan이나 analysis 단계에 영향을 주는지에 대해서는 좀 더 연구가 필요할 것 이다.
결론적으로, 녹내장 환자에서 OCT를 이용하여 국소적 망막신경섬유층의 결손을 검사할 때 위음성을 보이는 경우
는 20° 이하의 좁은 범위가 대부분이었다. OCT scan 자체 의 한계와 RNFL thickness analysis 단계에서 결손부위를 인식하지 못하는 문제들을 개선한다면 위음성의 정도를 감소 시킬 수 있을 것으로 생각되며, 위음성이 의심되는 경우에 는 OCT의 scan image와 analysis image를 같이 분석하면 도움이 될 것으로 생각한다.
참고문헌
1) Sommer A, Miller NR, Pollack I, et al. The nerve fiber layer in the diagnosis of glaucoma. Arch Ophthalmol 1977;95:2149-56.
2) Gupta N, Weinreb RN. New definitions of glaucoma. Curr Opin Ophthalmol 1997;8:38-41.
3) Varma R, Steinmann WC, Scott IU. Expert agreement in evalua- ting the optic disc for glaucoma. Ophthalmology 1992;99: 215-21.
4) Quigley HA, Addicks EM, Green WR. Optic nerve damage in human glaucoma; III. Quantitative correlation of nerve fiber loss and visual field defects in glaucoma, ischemic neuropathy, papilledema and toxic neuropathy. Arch Ophthalmol 1982;100:
135-46.
5) Caprioli J, Miller JM, Sears M. Quantitative evaluation of the optic nerve head in patients with unilateral visual field loss from primary open angle glaucoma. Ophthalmology 1987;94:1484-7.
6) Sommer A, Katz J, Quigley HA, et al. Clinically detectable nerve fiber atrophy precedes the onset of glaucomatous field loss. Arch Ophthalmol 1991;109:77-83.
7) Tuulonen A, Lehtola J, Airaksinen PJ. Nerve fiber layer defects with normal visual fields; Do normal optic disc and normal visual field indicate absence of glaucomatous abnormality? Ophthal- mology 1993;100:587-98.
8) Quigley HA, Katz J, Derick RJ, et al. An evaluation of optic disc and nerve fiber layer examinations in monitoring progression of early glaucoma damage. Ophthalmology 1992;99:19-28.
9) Schuman JS, Hee MR, Puliafito CA, et al. Quantification of nerve fiber layer thickness in normal and glaucomatous eyes using optical coherence tomography. Arch Ophthalmol 1995;113:586- 96.
10) Hwang JM, Kim TW, Park KH, et al. Correlation between topographic profiles of localized retinal nerve fiber layer defects as determined by optical coherence tomography and red-free fundus photography. J Glaucoma 2006;15:223-8.
11) Jeoung JW, Park KH, Kim TW, et al. Diagnostic ability of optical coherence tomography with a normative database to detect localized retinal nerve fiber layer defects. Ophthalmology 2005;
112:2157-63.
12) Budenz DL, Michael A, Chang RT, et al. Sensitivity and specificity of the stratus OCT for perimetric glaucoma. Ophthalmology 2005;112:3-9.
13) Teesalu P, Tuulonen A, Airaksinen PJ. Optical coherence tomo- graphy and localized defects of the retinal nerve fiber layer. Acta Ophthalmol Scand 2000;78:49-52.
14) Pieroth L, Schuman JS, Hertzmark E, et al. Evaluation of focal defects of the nerve fiber layer using optical coherence tomo- graphy. Ophthalmology 1999;106:570-9.
15) Mikelberg FS, Yidegiligne HM, Shulzer M. Optic nerve axon
=ABSTRACT=
Analysis of Localized Retinal Nerve Fiber Layer Defects not Detected by Optical Coherence Tomography
Young Sang Han, MD1, Seung Youn Jea, MD, PhD2, Su Jin Kim, MD1, Joo Eun Lee, MD, PhD3, Ji Eun Lee, MD, PhD1, Gi Hong Koo, MD1
Department of Ophthalmology, College of Medicine, Pusan National University1, Busan, Korea, Lee Chun Sik、s Eye Clinic2, Busan, Korea,
Department of Ophthalmology, Maryknoll Hospital3, Busan, Korea
Purpose: To analyze localized RNFL defect cases that were identified in retinal nerve fiber layer (RNFL) fundus photographs but not in optical coherence tomography (OCT).
Methods: Analysis of OCT scans and images was performed for 14 eyes (17 locations) that showed localized RNFL defects in RNFL fundus photographs but not in RNFL thickness average analysis.
Results: With respect to the range of RNFL defects, 41.2% were less than 10°, 47.0% were 11 to 20°, and 11.8% were 21 to 30°.
In 71.4% of the RNFL cases the defects were less than 10°and the decrease of RNFL thickness was not readily observable on the OCT scan images. In all cases of RNFL defects in the 11 to 30°range the decrease in RNFL thickness could be assessed on the OCT scan images. Nonetheless, the decrease of RNFL thickness could not be seen on the OCT analysis images in which the results of the RNFL thickness made through an automated computer algorithm were displayed.
Conclusions: The range of localized RNFL defects that were difficult to detect with OCT consisted of those cases that were almost less than 20°. The limitations of the OCT scan itself in patients with RNFL with an angular width defect less than 10°and the problems of RNFL thickness analysis processing in patients with an angular width of 11 to 30°may decrease the sensitivity of OCT in diagnosing RNFL defects.
J Korean Ophthalmol Soc 2009;50(4):558-564
Key Words: Optical coherence tomography, RNFL defect, RNFL fundus photograph
Address reprint requests to Seung-Youn Jea, MD, PhD Department of Ophthalmology, Lee Chun Sik’s Eye Clinic of Korea
#9-1 Daecheong-dong, Jung-gu, Busan 600-093, Korea
Tel: 82-51-465-6761, Fax: 82-51-242-7341, E-mail: [email protected] scanning laser polarimetry. Am J Ophthalmol 2000;129:715-22.
18) Morgan JE, Waldock A. Scanning laser polarimetry of the normal human retinal nerve fiber layer: A quantitative analysis. Am J
graphy and red-free photography. Am J Ophthalmol 2002;133:
187-95.