서 론
당뇨 전단계(prediabetes)는 당뇨로 진행하는 중간 단계로서1) 우리
나라에서 최근 수년간 그 유병률이 증가 추세에 있으며 30세 이상 한국성인의 24.8%에 해당하는 830만 명이 당뇨 전단계에 해당하는 것으로 파악되고 있다.2) 미국 질병통제예방센터(Centers for Disease
Received March 9, 2017 Revised July 24, 2017 ` Accepted August 11, 2017
Corresponding author Yong-Jin Cho Tel: +82-41-570-2238, Fax: +82-41-574-7792 E-mail: [email protected]
ORCID: http://orcid.org/0000-0002-5932-1138
Copyright © 2018 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons At- tribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Original Article
https://doi.org/10.21215/kjfp.2018.8.1.47 eISSN 2233-9116
Korean J Fam Pract. 2018;8(1):47-51
Korean Journal of Family Practice
KJFP
건강검진 대상자에서 대장내시경 시행이 공복혈당장애 진단에 미치는 영향
김나래
1, 임재석
1, 조용진
1,*, 홍성호
2, 조주연
2, 오정은
1, 유병욱
2, 신경숙
3, 조 현
2, 신황식
1, 손두용
31순천향대학교 의과대학 천안병원 가정의학교실, 2순천향대학교 의과대학 서울병원 가정의학교실, 3순천향대학교 의과대학 구미병원 가정의학교실
The Effect of Colonoscopy on the Diagnosis of Impaired Fasting Glucose in Health Examination Subjects
Na-Rae Kim1, Jae-Seok Im1, Yong-Jin Cho1,*, Sung-Ho Hong2, Choo-Yon Cho2, Jung-Eun Oh1, Byung-Wook Yoo2, Kyung-Suk Shin3, Hyun Joe2, Hwang-Sik Shin1, Doo-Yong Son3
1Department of Family Medicine, Cheonan Hospital, Soon Chun Hyang University College of Medicine, Cheonan; 2Department of Family Medicine, Seoul Hospital, Soon Chun Hyang University College of Medicine, Seoul; 3Department of Family Medicine, Gumi Hospital, Soon Chun Hyang University College of Medicine, Gumi, Korea
Background: Early diagnosis of impaired fasting glucose (IFG) is important because 15%–30% of IFG patients are known to progress to diabetes mellitus in 5 years. In this study, patients were classified into two groups as follows: patients who underwent colonoscopy and who did not. We compared fasting glucose and glycated hemoglobin A1c (HbA1c) levels between the two groups. The fasting glucose levels of the subjects from each group whose HbA1c levels were between 5.7% and 6.4% were identified to determine how colonoscopy affects their fasting glucose levels.
Methods: The physical assessments, fasting glucose levels, and HbA1c levels of 19,707 patients who visited a Health Promotion Center were examined, and the subjects were divided into 3 subgroups according to HbA1c level (≤5.6%, 5.7%–6.0%, and ≥6.1%). Then, we compared fasting glucose levels between the colonoscopy and non-colonoscopy groups.
Results: The colonoscopy group showed a significant decrease in mean fasting glucose level in comparison with the non-colonoscopy group. The patients in the subgroups with HbA1c levels of ≤5.6% and 5.7%–6.0% who underwent colonoscopy presented significantly decreased fasting glucose levels. However, no significant difference was observed in the ≥6.1% subgroup.
Conclusion: We confirmed that the two subgroups with HbA1c levels of ≤5.6% and 5.7%–6.0% tended to exhibit decreased fasting glucose levels by prolonged fasting time according to performing colonoscopy, failing to diagnose IFG precisely. Therefore, we recommend to examine the HbA1c level on the day performing colonoscopy or to measure the fasting glucose level on another day to diagnose IFG.
Keywords: Colonoscopy; Glycated Hemoglobin A1c; Health Promotion; Impaired Fasting Glucose
Na-Rae Kim, et al. The Effect of Colonoscopy on Impaired Fasting Glucose
Korean Journal of Family Practice
KJFP
Control and Prevention, CDC)에서도 미국 성인의 3분의 1 이상인 8,600만 명이 당뇨 전단계에 해당되었으며, 5년 내에 15%–30%가 제 2 형 당뇨로 진행한다고 보고하였다.3)
당뇨 전단계를 진단하는 방법은 크게 3가지로 당화혈색소(glycat- ed hemoglobin A1c, HbA1c)가 5.7%–6.4%이거나, 공복혈당이 100–125 mg/dL인 경우, 그리고 2시간 경구 당부하검사(oral glucose tolerance test)에서 혈당이 140–199 mg/dL인 경우이다.4-6)
혈당에 영향을 미치는 요소에는 공복 시간, 수면, 스트레스 등의 여러 요소들이 있다. 대개 공복 시간이 길어지면 혈당수치는 감소하 는 것으로 알려져 있는데 Emberson 등7)의 연구에서는 6시간 이상 공복을 유지한 군의 경우 그렇지 않은 군에 비해 혈당수치가 감소함 을 확인하였고, 다른 연구에서는 공복 시간이 연장되면 체내 혈당 제거속도가 혈당의 방출량을 초과하여 혈당이 낮아지게 되며 공복 시간이 20–24시간까지 연장될 경우 혈당수치는 10%–15%까지도 감 소한다고 보고하였다.8) 수면 제한이 혈당의 대사에 영향을 미치는 영향에 대해 조사한 연구에서는 6일간 4시간으로 수면 제한을 실시 한 경우 혈당수치감소율이 수면을 제한하지 않은 군에 비해 40%나 낮은 것이 확인되었다.9) Finlayson과 Zimmerman10)은 당뇨가 없는 환 자에서 발생할 수 있는 고혈당의 원인에 대해 연구를 시행하였으며 스트레스가 혈당을 높일 수 있는 요인 중 하나로 지적되었고, 그 기 전으로는 스트레스에 의해 시상하부-뇌하수체-부신축이 활성화되 면 코르티솔의 분비가 유도되어 혈당수치가 증가하게 된다고 보고 하였다.
일반적으로 이루어지는 건강검진 시 혈당을 측정하게 되어있으나 검사 당일 대장내시경을 함께 시행하는 경우 대장내시경이 통상적 인 공복 시간에 비해 더 긴 공복 시간을 유지해야 하기 때문에 대장 내시경 시행이 혈당수치에 영향을 미칠 가능성에 대해 평가해 볼 필 요가 있다. 이를 위해 본 연구에서는 건강검진센터에 내원하여 대장 내시경을 시행한 군과 시행하지 않은 군의 공복혈당, 당화혈색소를 비교하고 두 군에서 당뇨 전단계인 HbA1c 5.7%–6.4%에 해당하는 수 검자들의 공복혈당을 비교하였다.
방 법
1. 연구 대상
2012년 1월부터 2016년 1월까지 30세 이상의 순천향대학교 천안병 원 건강검진센터를 방문한 21,817명을 대상으로 신체계측과 최소 8 시간의 금식 이후 공복혈당, 당화혈색소 및 기타 혈액검사를 시행하 였다. 이 중 당뇨, 고혈압, 이상지질혈증, 간질환, 빈혈로 진단받은 과 거력이 있거나, 검사에 영향을 줄 수 있는 약물 복용자를 제외하였
으며, 검진에서 공복 혈당이 126 mg/dL 이상이거나 당화혈색소 6.5%
이상인 자를 제외한 19,707명을 최종 연구 대상으로 하였다.
2. 연구 방법
수검자들을 대상으로 문진 및 신체계측, 혈액 검사를 시행하였다.
허리둘레는 가장 아래쪽 늑골 하부와 골반 장골능의 중간 지점에서 측정하였으며, 체질량지수는 몸무게(kg)를 키(m)의 제곱으로 나누 어 계산하였다. 수축기 혈압과 이완기 혈압(mmHg)은 5분 휴식 후 안정상태에서 수은 혈압계를 사용하여 총 2차례 측정하였으며, 본 연구에서는 2차례 측정값의 평균값을 사용하였다. 혈액검사는 최소 8시간 금식 후 정맥혈에서 채혈하여 공복혈당, 당화혈색소 등을 측 정하였다. 음주 및 흡연은 수검자 문진을 통해 조사하였으며 음주는 주당 음주 횟수와 주종, 1회 음주량을 통해 1주일 동안 섭취한 음주 량(g)을 계산하여 남성 40 g 이상, 여성 20 g 이상일 때 과음으로 정의 하였다. 흡연은 지금까지 한 번도 흡연을 하지 않은 비흡연자, 현재 흡연 중인 흡연자, 과거에 흡연한 적이 있는 금연자로 분류하였다. 대 장내시경 시행 여부에 따라서 대장내시경 시행군과 미시행군으로 나누었으며, 대장내시경을 시행하는 군은 수클리어(Suclear
®
;Pharm bio Korea Inc., Seoul, Korea) 1 L를 총 2회로 나누어 검사 전일 오후 7시, 검사 당일 오전 5시에 복용하였다.
3. 통계 분석
통계학적 분석은 SPSS for window 14.0 (SPSS Inc., Chicago, IL, USA) 을 이용하였으며, 결과값은 평균±표준편차로 표시하였다. 대장내시 경 시행군과 미시행군의 일반적 특성을 비교하기 위해 Student’s t-test 및 chi-square test를 사용하여 분석하였다. 당화혈색소 5.6% 이하, 5.7%부터 6.0%, 6.1% 이상의 세 군으로 나누어 각 군의 대장내시경 시 행 여부에 따른 공복혈당을 비교하기 위해 t-test를 시행하였으며, 선 형회귀분석을 이용하여 대장내시경 시행군과 미시행군의 당화혈색 소에 따른 공복혈당 변화를 비교하였다. 또한, 대장내시경 시행 여부 가 공복혈당에 단독적으로 미치는 영향을 알아보기 위해 다중선형 회귀분석을 사용하여 대장내시경 시행군과 미시행군간의 특성 차 이 보정을 하였다. 모든 통계의 유의수준은 신뢰구간 95%, P<0.05로 하였다.
결 과
1. 일반적 특성
총 연구 대상 19,707명 중 대장내시경을 시행한 군은 5,528명이었 으며, 시행하지 않은 군은 14,179명이었다. 대장내시경 시행군의 평균
김나래 외. 대장내시경 시행이 공복혈당장애 진단에 미치는 영향 Korean Journal of Family Practice
KJFP
나이는 42.57±9.11세로 미시행군의 41.38±9.06세와 유의한 차이가 있 었다(P=0.000). 또한 비만도(24.12±3.15 kg/m2 vs. 23.86±3.32 kg/m2, P=0.000)와 허리둘레(81.45±11.60 cm vs. 80.14±12.80 cm, P=0.000)도 두 군 간의 유의한 차이를 보였다. 대장내시경 시행군과 미시행군 간 의 수축기 혈압(116.98±11.36 mmHg vs. 115.90±11.86 mmHg, P= 0.000) 및 이완기 혈압(71.85±8.20 mmHg vs. 71.09±8.42 mmHg, P= 0.009)도 시행군에서 유의하게 높았다. 대장내시경 시행군의 공복 혈당은 90.28±10.62 mg/dL로 미시행군의 92.15±9.21 mg/dL에 비해 유의하게 낮 았으며(P= 0.000), 당화혈색소는 대장내시경 시행군에서 5.45%±0.29%로 미시행군의 5.47%±0.27%와 유의한 차이가 있었다 (P=0.002). 대장내시경을 시행한 군에서는 과음을 한 비율이 55.5%였
으며, 미시행군의 과음 비율은 49.0%로 빈도수에 통계적 유의한 차 이를 보였으며(P=0.000), 흡연력에서는 대장내시경 시행군과 미시행 군 간의 비흡연자, 흡연자, 금연자(48.0% vs. 54.8%, 25.7% vs. 23.1%, 26.3%
vs. 22.1%, P=0.000) 각각에 대하여 유의한 차이가 있었다(Table 1).
2. 대장내시경 시행 유무에 따른 당화혈색소군 간의 혈당 비교 당화혈색소 5.6% 이하(Group I)는 15,109명이었으며, 5.7%에서 6.0%
(Group II)까지는 4,140명, 6.1% 이상(Group III)은 456명이었다. Group I의 대장내시경 시행군의 공복혈당은 88.45±9.40 mg/dL로 미시행군 의 공복혈당인 90.66±7.97 mg/dL에 비해 통계적으로 유의하게 낮았 으며(P=0.000), Group II의 대장내시경 시행군 공복혈당 역시 95.21±10.91 mg/dL로 미시행군 공복혈당 95.94±9.84 mg/dL보다 유의 하게 낮았다(P=0.004). 하지만 Group III의 대장내시경 시행군의 공 복혈당과 미시행군의 공복혈당 사이 통계적 유의한 차이는 보이지 않았다(Table 2).
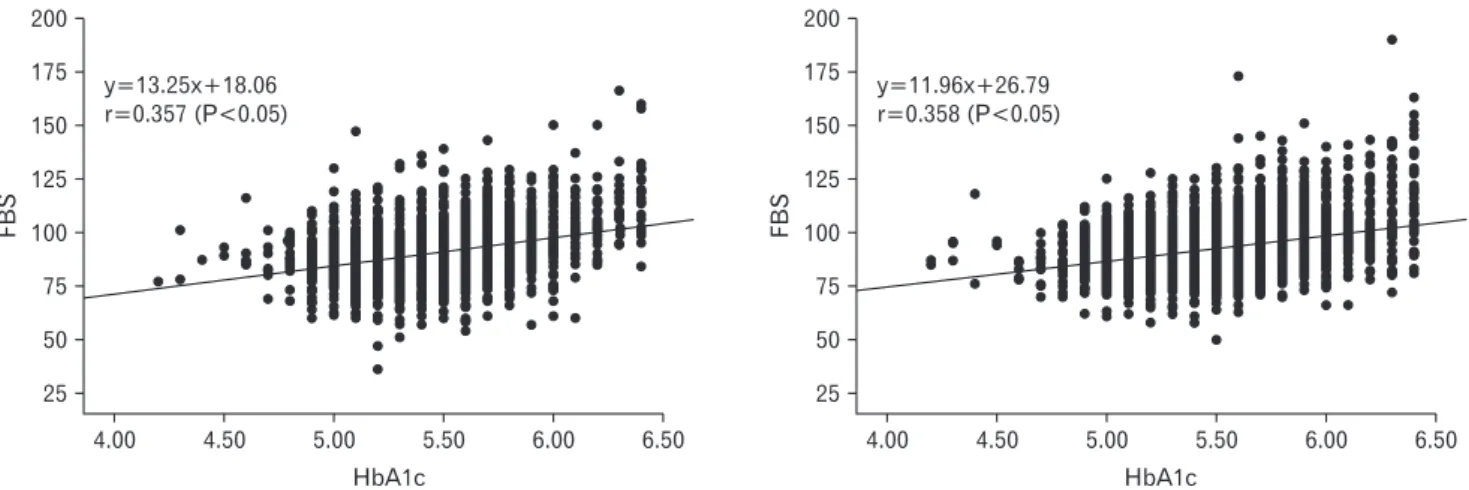
대장내시경 시행군과 미시행군의 당화혈색소에 대응되는 공복혈 당 수치를 단순회귀분석을 사용하여 구하였다. 당뇨 전단계를 진단 할 수 있는 cut-off value인 당화혈색소 5.7%에 대응되는 공복혈당은 대장내시경 시행군에서는 93.57 mg/dL이었으며, 대장내시경 미시행 군은 94.93 mg/dL로 나타났다(P=0.000) (Figure 1).
대장내시경 시행군과 미시행군 간의 특성 차이 보정을 위해 Table 1에서 통계학적으로 유의미한 차이를 보인 항목을 다중선형회귀분 석을 이용하여 분석하였고 후진 제거법을 사용하여 유의한 변수를 선별하였으며 최종 변수로 Table 3에 기술된 항목이 선택되었다. 단 순선형회귀분석을 이용하여 대장내시경 시행 여부가 혈당에 미치 는 영향을 분석하였을 때 베타값 -1.871, 표준오차 0.153으로 유의한 감소를 보였으며, 최종변수를 보정한 결과 대장내시경 시행군에서 미시행군보다 공복혈당이 베타값 -1.981, 표준오차 0.139로 유의한 차 이를 보였고, 대장내시경 시행 여부만을 분석하였을 때보다 공복혈 당 차이가 더 크게 나타났다(Table 3).
Table 1. Clinical characteristics of study subjects Variable Colonoscopy group
(n=5,528)
Non-colonoscopy
group (n=14,179) P-value
Age (y) 42.57±9.11 41.38±9.06 0.000
BMI (kg/m2) 24.12±3.15 23.86±3.32 0.000
WC (cm) 81.45±11.60 80.14±12.80 0.000
SBP (mmHg) 116.98±11.36 115.90±11.86 0.000
DBP (mmHg) 71.85±8.20 71.09±8.42 0.009
FBS (mg/dL) 90.28±10.62 92.15±9.21 0.000
HbA1c (%) 5.45±0.29 5.47±0.28 0.002
TG (mg/dL) 106.96±71.50 123.29±75.23 0.000
HDL-C (mg/dL) 57.43±15.25 56.29±14.66 0.005
LDL-C (mg/dL) 120.14±33.02 111.25±30.47 0.000
AST (IU/L) 27.43±16.04 21.19±12.58 0.000
ALT (IU/L) 28.80±23.77 22.98±20.81 0.000
r-GT (IU/L) 37.51±51.97 32.37±43.61 0.000
UA (mg/dL) 5.47±1.39 5.26±1.42 0.014
hs-CRP (mg/L) 1.25±3.43 1.09±2.82 0.002
Problem drinker 3,070 (55.5) 6,952 (49.0) 0.000
Smoker 0.000
Never 2,654 (48.0) 7,776 (54.8)
Current 1,419 (25.7) 3,271 (23.1)
Former 1,455 (26.3) 3,132 (22.1)
Values are presented as means±standard deviation or number (%).
BMI, body mass index; WC, waist circumference; SBP, systolic blood pressure;
DBP, diastolic blood pressure; FBS, fasting blood sugar; HbA1c, glycated hemo- globin A1c; TG, triglyceride; HDL-C, high density lipoprotein-cholesterol; LDL-C, low density lipoprotein-cholesterol; AST, aspartate aminotransferase; ALT, ala- nine aminotransferase; r-GT, gamma glutamyl-transpeptidase; UA, uric acid; hs- CRP, high sensitivity C-reactive protein.
P-values are calculated from t-test an chi-square test.
Table 2. Comparison of fasting glucose level between colonoscopy group and non-colonoscopy group
Group Group I
HbA1c ≤5.6 (n=15,109) P-value Group II
HbA1c 5.7–6.0 (n=4,140) P- value Group III
HbA1c ≥6.1 (n=458) P-value
Colonoscopy group 88.45±9.40 0.000 95.21±10.91 0.004 108.08±14.97 0.086
Non-colonoscopy group 90.66±7.97 95.94±9.84 106.80±16.19
Values are presented as means±standard deviation.
HbA1c, glycated hemoglobin A1c.
P-values are calculated from t-test.
Na-Rae Kim, et al. The Effect of Colonoscopy on Impaired Fasting Glucose
Korean Journal of Family Practice
KJFP
고 찰
당뇨 전단계는 아직 당뇨병으로 이환되지 않은 높은 정상범주의 혈당수치를 나타내는 상태로 제 2형 당뇨로 진행될 수 있는 가능성 을 높일 뿐 아니라 심혈관계 질환의 발생 위험을 증가시키고 예후에 도 나쁜 영향을 미치는 것으로 알려져 있다.11,12) 하지만 적절한 육체 활동, 정상체중 유지 등을 포함한 생활습관개선 및 약물을 통한 치 료가 당뇨 전단계에서 당뇨병으로의 이환의 예방에 효과가 있다는
연구결과가 보고되고 있어13-18) 당뇨 전단계를 조기에 진단하고 적절 한 치료를 시행하는 것이 환자의 향후 예후에 매우 중요하다고 할 수 있겠다.
위의 결과에서 당화혈색소가 5.6% 이하인 군에서 대장내시경을 시행한 군의 공복혈당이 유의하게 낮은 것으로 확인되었고, 당화혈 색소가 5.7%–6.0%인 군에서도 대장내시경 시행 군에서 공복혈당 수 치가 유의하게 낮게 측정되었다. 또한, 당뇨 전단계를 진단할 수 있는 당화혈색소 5.7%에 대응하는 공복혈당 수치가 대장내시경 시행 군 에서 미시행군에 비해 더 낮은 결과를 보여 공복 시간이 길어질수록 혈당이 감소한다는 기존의 연구들과 본 연구의 결과가 일치하였 다.7,8,19)
당화혈색소 5.6%–6.0% 사이에 해당하는 당뇨 전단계 환자들에서 대장내시경 시행에 따른 긴 공복 시간은 통상적 공복 시간에 따른 공복혈당보다 더 낮은 수치를 보이게 되고, 이로 인하여 당뇨 전단계 환자들을 진단함에 있어서 어려움이 야기될 수 있음을 확인하였다.
본 연구에서는 대장내시경을 위한 수클리어 복용,20) 검사 전날 수
면 부족,9,21) 대장내시경 시행에 따른 스트레스 등에 의한 호르몬의
변동10) 등의 변수들을 통제하지 못해 연구결과의 신뢰도를 떨어뜨 린다는 점 등이 제한점이 될 수 있다. 그러나 약 2만 명에 가까운 환 자들을 대상으로 대규모 연구를 시행하였고, 대장내시경 시행으로 인한 긴 공복 시간에 따른 혈당 변화에 대한 연구가 이루어진 사례 를 거의 찾아보기 어렵다는 점 등에서 본 연구가 의의가 있을 것으 로 생각된다.
결론적으로 본 연구는 대장내시경을 시행할 경우 공복 시간의 연 장으로 인해 당화혈색소가 높은 군에서 공복혈당이 낮게 측정될 수 있으므로 공복혈당장애를 진단하지 못할 가능성이 있음을 확인하 였다. 따라서 공복혈당장애를 진단함에 있어 대장내시경이 예정되 Table 3. Multiple linear regression analysis for influencing factors on
fasting glucose
Variable β Standard error P-value
Colonoscopy* -1.981 0.139 0.000
Age (y) 0.100 0.007 0.000
BMI (kg/m2) 0.186 0.025 0.000
WC (cm) 0.021 0.006 0.001
SBP (mmHg) 0.068 0.009 0.000
DBP (mmHg) 0.054 0.012 0.000
HbA1c (%) 9.926 0.226 0.000
TG (mg/dL) 0.013 0.001 0.000
HDL-C (mg/dL) -0.011 0.005 0.025
LDL-C (mg/dL) 0.007 0.002 0.001
AST (IU/L) -0.011 0.005 0.039
r-GT (IU/L) 0.020 0.002 0.000
Problem drinker 1.391 0.127 0.000
BMI, body mass index; WC, waist circumference; SBP, systolic blood pressure;
DBP, diastolic blood pressure; HbA1c, glycated hemoglobin A1c; TG, triglycer- ide; HDL-C, high density lipoprotein-cholesterol; LDL-C, low density lipoprotein- cholesterol; AST, aspartate aminotransferase; r-GT, gamma glutamyl-transpepti- dase.
*Subjects who underwent colonoscopy.
P-values are calculated from multiple linear regression analysis.
Figure 1. Comparison of fasting blood glucose which corresponds to different HbA1c level between colonoscopy group and non-colonoscopy group. The fasting blood glucose that corresponded to HbA1c 5.7% was 93.57 mg/dL in the colonoscopy group (left), and 94.93 mg/dL in the non-colonoscopy group (right).
HbA1c, glycated hemoglobin A1c; FBS, fasting blood sugar.
4.00 200 175 150 125 100 75 50
6.50
FBS
HbA1c 25
y=13.25x+18.06 r=0.357 (P<0.05)
6.00 5.50
5.00
4.50 4.00
200 175 150 125 100 75 50
6.50
FBS
25
y=11.96x+26.79 r=0.358 (P<0.05)
6.00 5.50
5.00 4.50
HbA1c
김나래 외. 대장내시경 시행이 공복혈당장애 진단에 미치는 영향 Korean Journal of Family Practice
KJFP
어 있는 수검자들의 경우 추후 공복혈당 수치에 대한 검사를 시행하 거나 또 다른 당뇨 전단계 진단방법인 당화혈색소 수치 측정을 대장 내시경 시행 시에 추가하는 등 여러 보완적인 방법이 필요할 것으로 보인다.
요 약
연구배경:
공복혈당장애가 있는 사람의 15%–30%는 5년 안에 당뇨 로 진행될 수 있으므로 공복혈당장애를 조기에 진단하는 것이 중요 하다. 본 연구는 대장내시경을 시행한 수검자 군과 시행하지 않은 수 검자 군의 공복혈당, 당화혈색소를 비교하고, 두 군에서 당화혈색소 5.7%–6.4%인 수검자들의 공복혈당을 비교하여 대장내시경 시행이 해 당 수검자들의 공복 혈당수치에 미치는 영향을 확인하고자 하였다.방법:
순천향대학교 천안병원 건강검진센터 수검자 19,707명을 대 상으로 신체계측과 공복혈당, 당화혈색소 등을 분석하였으며, 당화 혈색소 5.6% 이하, 5.7%부터 6.0%, 6.1% 이상의 세 군으로 나누어 각 군의 대장내시경 시행 유무에 따른 공복혈당을 비교하였다.결과:
대장내시경을 시행한 군에서는 시행하지 않은 군에 비해 공 복혈당 평균 수치의 유의한 감소를 보였으며, 당화혈색소 5.6% 이하, 5.7%부터 6.0%의 두 군에서 대장내시경 시행 시 공복 혈당이 통계적 으로 유의하게 감소하였으나 당화혈색소 6.1% 이상 군에서는 그 결 과가 유의한 차이를 보이지 않았다.결론:
본 연구는 대장내시경을 시행할 경우 공복 시간의 연장으로 인해 당화혈색소가 5.6% 이하인 군과 5.7%–6.0% 사이인 군에서 공복 혈당이 낮게 측정되는 경향을 보였고, 그에 따라 공복혈당장애를 진 단하지 못할 가능성이 있음을 확인하였다. 따라서 공복혈당장애를 진단함에 있어 대장내시경 시행 시 당화혈색소 수치를 동시에 측정 하거나 추후 공복혈당 수치에 대한 검사가 필요하다.중심단어:
대장내시경; 당화혈색소; 건강검진; 공복혈당장애 REFERENCES1. Chun KH. Evidence-based management and treatment of high-risk indi- viduals with pre-diabetes. J Korean Med Assoc 2011; 54: 1020-7.
2. Korean Diabetes Association. Diabetes Fact Sheet in Korea 2016 [Internet].
Korean Diabetes Association (KR): c2011. [cited 2017 Feb 20]. Available from: http://www.diabetes.or.kr.
3. Centers for Disease Control and Prevention. National Diabetes Statistics Report: Estimates of Diabetes and Its Burden in the United States, 2014 [In- ternet]. Atlanta (GA): US Department of Health and Human Services. [cited 2017 Feb 20]. Available from: https://www.cdc.gov/diabetes/pdfs/
data/2014-report-estimates-of-diabetes-and-its-burden-in-the-united- states.pdf.
4. Expert Committee on the Diagnosis and Classification of Diabetes Mellitus.
Report of the expert committee on the diagnosis and classification of diabe- tes mellitus. Diabetes Care 2003; 26 Suppl 1: S5-20.
5. American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2010; 33 Suppl 1: S62-9.
6. International Expert Committee. International Expert Committee report on the role of the A1C assay in the diagnosis of diabetes. Diabetes Care 2009; 32: 1327-34.
7. Emberson JR, Whincup PH, Walker M, Thomas M, Alberti KG. Biochemi- cal measures in a population-based study: effect of fasting duration and time of day. Ann Clin Biochem 2002; 39: 493-501.
8. Gerich JE. Physiology of glucose homeostasis. Diabetes Obes Metab 2000; 2:
345-50.
9. Spiegel K, Tasali E, Leproult R, Van Cauter E. Effects of poor and short sleep on glucose metabolism and obesity risk. Nat Rev Endocrinol 2009; 5: 253-61.
10. Finlayson C, Zimmerman D. Hyperglycemia not due to diabetes mellitus.
Clinical Pediatric Emergency Medicine 2009; 10: 252-5.
11. Huang Y, Cai X, Mai W, Li M, Hu Y. Association between prediabetes and risk of cardiovascular disease and all cause mortality: systematic review and meta-analysis. BMJ 2016; 355: i5953.
12. Mijajlović MD, Aleksić VM, Šternić NM, Mirković MM, Bornstein NM.
Role of prediabetes in stroke. Neuropsychiatr Dis Treat 2017; 13: 259-67.
13. Eriksson KF, Lindgärde F. Prevention of type 2 (non-insulin-dependent) di- abetes mellitus by diet and physical exercise. The 6-year Malmö feasibility study. Diabetologia 1991; 34: 891-8.
14. Carey VJ, Walters EE, Colditz GA, Solomon CG, Willett WC, Rosner BA, et al. Body fat distribution and risk of non-insulin-dependent diabetes melli- tus in women. The Nurses’ Health Study. Am J Epidemiol 1997; 145: 614-9.
15. Chiasson JL, Josse RG, Gomis R, Hanefeld M, Karasik A, Laakso M; STOP- NIDDM Trail Research Group. Acarbose for prevention of type 2 diabetes mellitus: the STOP-NIDDM randomised trial. Lancet 2002; 359: 2072-7.
16. Knowler WC, Hamman RF, Edelstein SL, Barrett-Connor E, Ehrmann DA, Walker EA, et al. Prevention of type 2 diabetes with troglitazone in the Dia- betes Prevention Program. Diabetes 2005; 54: 1150-6.
17. Knowler WC, Barrett-Connor E, Fowler SE, Hamman RF, Lachin JM, Walk- er EA, et al. Reduction in the incidence of type 2 diabetes with lifestyle inter- vention or metformin. N Engl J Med 2002; 346: 393-403.
18. DREAM (Diabetes REduction Assessment with ramipril and rosiglitazone Medication) Trial Investigators, Gerstein HC, Yusuf S, Bosch J, Pogue J, Sher- idan P, et al. Effect of rosiglitazone on the frequency of diabetes in patients with impaired glucose tolerance or impaired fasting glucose: a randomised controlled trial. Lancet 2006; 368: 1096-105.
19. Hulmán A, Færch K, Vistisen D, Karsai J, Nyári TA, Tabák AG, et al. Effect of time of day and fasting duration on measures of glycaemia: analysis from the Whitehall II Study. Diabetologia 2013; 56: 294-7.
20. Rex DK, McGowan J, Cleveland Mv, Di Palma JA. A randomized, controlled trial of oral sulfate solution plus polyethylene glycol as a bowel preparation for colonoscopy. Gastrointest Endosc 2014; 80: 482-91.
21. Morselli L, Leproult R, Balbo M, Spiegel K. Role of sleep duration in the reg- ulation of glucose metabolism and appetite. Best Pract Res Clin Endocrinol Metab 2010; 24: 687-702.