대한소화기학회지 2004;44:179~185 REVIEW
서 론
1)우리나라에서 식도암은 연간1,500여 명이 발생하며 남 자 암 환자 발생률에서 위를 차지한다7 .1 주로 남자에게 호 발(95%)하며 지난, 20년 간 점진적으로 증가 추세를 보이 고 있다 서양에서는 선암이 증가하고 있으나 우리나라를. , 포함한 동아시아권에서는 편평상피암이 아직까지 대부분을 차지한다.
식도암은 대개 증상이 나타난 후에 진단이 되고 진단 시, 접수: 2004년 월 일8 9
연락처 김성배: , 138-736, 서울 송파구 풍납 동2 388-1 서울아산병원 내과
Tel: (02) 3010-3217, Fax: (02) 3010-6961 E-mail: [email protected]
이미 풍부한 점막하 림프 조직을 통하여 주위 조직으로 전 이된 경우가 흔하다.22)수술 단독 치료가 국소적 식도암의 표준 치료로 알려져 있으나 종양 완전 절제와 림프절곽청, 술을 시행한다 하더라도 결국 전신 또는 국소 재발로 인하 여 년 생존율이5 15-39%에 불과할 정도로 예후가 불량하 다.3 이를 극복하기 위해 수술 이외에 화학요법 방사선요, 법을 병용하는 복합 치료(combined-modality therapy)연구 가 진행되어 왔다 복합 치료에 대한 수많은 제 상 제 상. 2 , 3 임상 연구가 진행되었음에도 불구하고 국소적 식도암에서,
Correspondence to: Sung-Bae Kim, M.D.
Department of Internal Medicine, Asan Medical Center 388-1 Pungnap-2dong, Songpa-gu, Seoul 138-736, Korea Tel: +82-2-3010-3217, Fax: +82-2-3010-6961 E-mail: [email protected]
국소적 식도암에서 복합 치료
울산대학교 의과대학 내과학교실
김 성 배
Combined-modality Therapy for Locoregional Esophageal Cancer Combined-modality Therapy for Locoregional Esophageal Cancer Combined-modality Therapy for Locoregional Esophageal Cancer Combined-modality Therapy for Locoregional Esophageal Cancer
Sung-Bae Kim, Sung-Bae Kim, Sung-Bae Kim, Sung-Bae Kim, M.D.
Department of Internal Medicine, University of Ulsan College of Medicine, Seoul, Korea
Treatment for patients with esophageal cancer remains unsatisfactory. Although surgery alone or chemo- radiotherapy have been generally accepted as reasonable options for patients with locoregional esophageal cancer, 5-year survival rate of either management is about 20%. The limited success of single modality treatment using radiotherapy or surgery has led to the investigation of multimodality therapies, combining chemotherapy, radiotherapy, and surgery. However, the appropriateness of such therapies remains unanswered. A number of prospective randomized trials of trimodality therapy versus surgery alone suggest benefits of combined-modality therapy. Concurrent chemoradiotherapy is an alternative treatment in selected resectable cases to show potential benefits in survival and local control. Patients with complete response following neoadjuvant therapy have consistent, substantial benefits in survival. Pretreatment staging is necessary for standardization of patients undergoing treatment protocols and for outcome evaluation. Biologic markers can be used to predict response to therapy and might allow designation of treatment based on the individual tumor. In the future, clinical trials testing optimal integration of preoperative regimen including new drugs may impact on the prognosis of esophageal cancer. (Korean J Gastro (Korean J Gastro (Korean J Gastro (Korean J Gastroenterol 2004;44:179-185) enterol 2004;44:179-185) enterol 2004;44:179-185) enterol 2004;44:179-185)
Key Key Key
Key Words: Words: Words: Esophageal cancer; Chemoradiotherapy; Combined-modality Words:
대한소화기학회지 제 권 제 호: 44 4 , 2004
180
복합치료의 효과가 아직도 논란의 대상이 되는 것은 대부 분 연구에 포함된 환자의 수가 적고 보고마다 종양 병기와, 치료 계획의 차이가 있어 치료 성적을 직접 비교하는 것이 어렵기 때문이다.
본 글에서는 식도암의 치료 원칙과 여러 방법의 복합 치 료 중 관심을 끌고 있는 수술 전 선행화학요법(preoperative
수술 전 화학 방사선 동시 치료
chemotherapy), - (preoperative 근치적 화학 방사선 동시 치료
chemoradiotherapy), - (definitive 수술 후 보조화학요법
chemoradiotherapy), (postoperative 에 관한 무작위 비교 임상 연구 결 adjuvant chemotherapy)
과를 중심으로 복합 치료의 치료 성적과 문제점을 살펴보 고자 한다.
식도암의 치료 원칙
식도암 치료는 완치 목적의 근치적 치료와 증상 완화 목 적의 고식적 치료로 크게 구분할 수 있다 조기 식도암에서. 수술 단독 치료만 시행하는 것에 이견이 없으나 국소적 진, 행성 식도암에서 적절한 치료 방법의 선택은 대부분 진단 시 식도암의 병기와 환자의 활동 능력에 의해 결정된다
국소적 식도암이라도 식도 외 주위 장기 침범으 (Table 1).
로 인하여Horner 증후군 반회신경마비에 따른 애성 상부, , 쇄골 림프절 침범 기관지식도루가 발생한 경우는 수술 절, 제가 불가능한 경우에 해당한다 전이성 식도암에서는 중. 앙 생존기간이 개월에 불과하고 항암제에 반응을 보인다6 , 하더라도 일시적이다 반면 국소적 식도암의 일부 환자에. , 서는 장기 생존 완치 을 기대할 수 있어 환자의 전신상태가( ) 양호한 국소적 식도암 환자의 경우 적극적인 치료를 고려 해야 한다 방사선 단독 치료는 근치적 치료로 간주하기는. 어려우며 수술 전 및 수술 후 방사선 치료는 무작위 비교, 연구에서 수술 단독 치료에 비해 치료 성적의 차이가 없어 여기서 다루지 않는다.
수술 전 선행화학요법 (Preoperative chemotherapy)
수술 전 화학요법을 시행하는 목적은 병기 하강(down- 을 통해 수술 시 완전 절제율을 높이고 미세 전이
staging) ,
부위를 조기에 제거함으로써 궁극적으로 생존 기간을 연장 하는 것이다 수술 전 선행화학요법에 관한 무작위 비교 연. Table 1.
Table 1.Table 1.
Table 1. Options in the Definitive Treatment for Esophageal Cancer
Indication Recommendation Evidence
Surgery alone Best single modality therapy. As yet no other options definitively proven to be superior
Long-term survival results well docu- mented
Primary radiotherapy Used only for patients who are not candidates for concurrent chemoradiation or with small early tumors
Long-term survival 0-10% for locally advanced disease and 15-25% for early disease. Randomized trials have demon- strated a survival and local control benefit when chemotherapy is added Definitive chemoradiotherapy Appropriate choice for nonoperative man-
agement
Randomized trials have demonstrated 5-year survival of 9-27%
Preoperative radiotherapy No known benefit 5 randomized trials Postoperative radiotherapy No known benefit
Used for known residual disease
2 randomized trials
Preoperative chemoradiotherapy Accepted alternative approach, although further data demonstrating a survival benefit are needed. Substantial local control benefit
Promising results in phase II trials. Mixed results in modestly powered randomized trials. A definitive large randomized U.S.
intergroup trial closed with low recruitment Preoperative chemotherapy Possible improvement in outcome Mixed results in two large randomized
trials
Postoperative chemotherapy No known survival benefit 3 randomized trials-improvement in DFS in 1 randomized trial
DFS, disease free survival.
김성배 국소적 식도암에서 복합 치료.
181
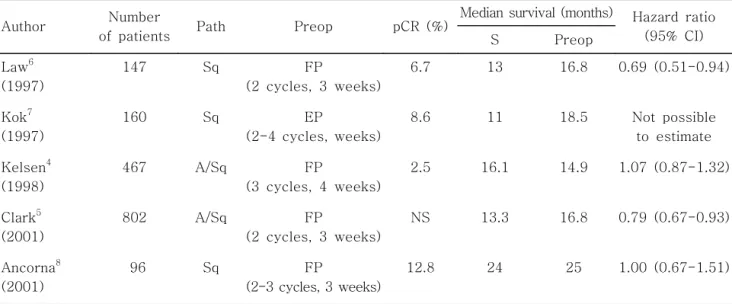
구4-8중 다음의 가지 연구가 흔히 인용된다2 (Table 2).
등
Kelsen 4이 1998년에 발표한 다기관 North America Intergroup Trial(INT 0113)은467명을 대상으로 5-FU,
를 수술 전
CDDP 4주 간격으로 회 수술 후 회 투여하였3 , 2 다 이 연구에서 선행화학요법에 따른 수술 유병률 사망률. , 은 증가하지 않았으나 절제연에 종양이 남아 있는 경우, (R1 는 선행화학요법군에서 수술 단독군에 비해 유의 resection)
하게 적었다(4%, 15%, p=0.001).원격 전이는 선행화학요 법군에서 수술 단독군에 비해 적은 경향이나(41%, 50%,
중앙 생존 기간의 차이는 없었다 현재까지 가장
p=0.21), . 규
모가 큰 선행화학요법 연구는2002년 영국에서Clark등5이 보고한 것으로802명의 환자가 참여하였다. 5-FU, CDDP를 매 주마다 회 투여 후 수술을 하였는데 선행화학요법으3 2 , 로 인한 수술 유병률 사망률은 증가하지 않았다, . Intention 에 따른 선행화학요법군과 수술 단독군의 중앙 to analysis
생존 기간은 각각16.8개월과13.3개월 년 생존율은 각각, 2 와 로 선행화학요법군의 치료 성적이 우월하였다
43% 34% .
수술 시 완전 절제(R0 resection)율도 선행화학요법군에서 높 았다. 영국에서는 이 논문이 발표된 후 회의2 5-FU, CDDP 선행화학요법이 식도암의 표준 치료로 인정되고 있다.9
위의 두 보고 사이에는 수술 단독군의 년 생존율이2 로 일치한다는 공통점과 항암제의 용량 투여 계획
34% ,
(CDDP 100 mg/m2대 80 mg/m2, 3회 대 회 주 간격 대2 , 4 주 간격 수술 시기 일 대 일 그리고 수술 탈락률
3 ), (93 63 ),
대 의 차이점이 있는데 수술
[93/234 (40%) 52/400 (13%)] , 전 투여한 항암제로 수술 기회를 놓쳐 오히려 치료 성적이 낮아질 수 있음을 시사한다 통계적으로 충분한 환자 수가.
포함된 위의 개 연구2 4,5와 개의, 2 meta-analysis3,10에서 상반 된 결과가 나와 현 시점에서 수술 전 선행화학요법을 임상 에 일반화하여 그대로 적용할 수는 없다. National Compre-
치료 지침
hensive Cancer Network (NCCN) 11도 이러한 치 료를 표준 치료로 인정하지 않고 있다.
수술 전 화학 방사선 동시 치료 - (Preoperative chemoradiotherapy)
항문암 직장암 비소세포폐암에서 수술 전 화학 방사선, , - 병용 치료에 따른 결과가 향상되면서 식도암에서도 이를 적용하고자 하는 시도가 활발히 진행되어 왔다(Table 3).
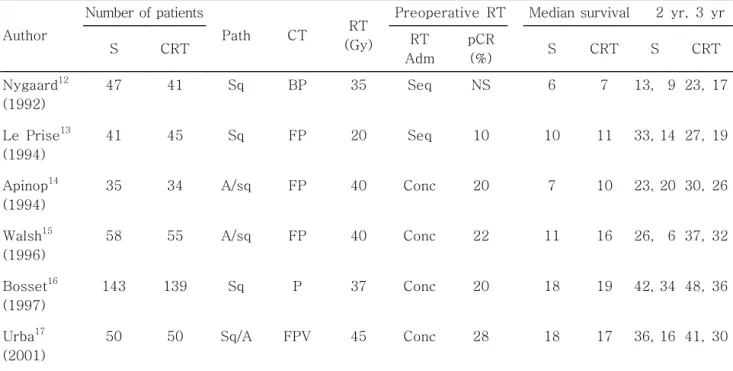
개의 무작위 비교 연구
6 12-17에서 가장 먼저 발표된 것이
년 스칸디나비아에서 등
1992 Nygaard 12이 보고한 것인데, 수술 단독 치료 수술 전 선행화학요법 수술 전 방사선 치료, , , 수술 전 화학 방사선 병용 치료 개의 치료군으로 비교하- 4 였다 식도암에서 현재 사용하지 않는. bleomycin이 사용되 었고 방사선 조사량이, 35 Gy로 적으며 화학 방사선 치료, - 가 동시 투여가 아닌 순차적으로 투여되었다는 사실이 본 연구의 문제점으로 지적된다. 113명의 식도암 선암 환자만 을 대상으로 수술 단독 치료와 수술 전 화학 방사선 동시- 치료(5-FU, CDDP, RT 40 Gy)를 무작위 비교 연구하였는 데 중, 앙 생존 기간은16개월 대11개월로 복합 치료군에서 생존 기간이 연장되었고(p=0.01), 병리적 완전 반응률은 이었다 수술 전 화학 방사선 동시 치료군의 년 생존율
25% . - 3
은32%,수술 단독군은6%이었다 수술 단독군에서 년 생. 3 존율이 6%로 지나치게 낮은 것이 문제점으로 지적된다.15 Table 2.
Table 2.Table 2.
Table 2. Randomized Trials of Preoperative Chemotherapy vs. Surgery Alone in Resectable Esophageal Cancer
Author Number
of patients Path Preop pCR (%) Median survival (months) Hazard ratio (95% CI)
S Preop
Law6 (1997)
147 Sq FP
(2 cycles, 3 weeks)
6.7 13 16.8 0.69 (0.51-0.94)
Kok7 (1997)
160 Sq EP
(2-4 cycles, weeks)
8.6 11 18.5 Not possible to estimate Kelsen4
(1998)
467 A/Sq FP
(3 cycles, 4 weeks)
2.5 16.1 14.9 1.07 (0.87-1.32)
Clark5 (2001)
802 A/Sq FP
(2 cycles, 3 weeks)
NS 13.3 16.8 0.79 (0.67-0.93)
Ancorna8 (2001)
96 Sq FP
(2-3 cycles, 3 weeks)
12.8 24 25 1.00 (0.67-1.51)
Path, pathology; Sq, squamous cell carcinoma; A, adenocarcinoma; pCR, pathologic complete response rate; S, surgery alone;
Preop, preoperative; FP, 5-FU, CDDP; EP, etoposide, CDDP; NS, not stated.
The Korean Journal of Gastroenterology: Vol. 44, No. 4, 2004
182
명의 식도암 환자를 대상으로 경열공 식도절제술 100
(transhiatal esophagectomy)을 시행한 수술 단독군과 항암 제(5-FU, CDDP, vinblastine)와 방사선45 Gy를 투여한 후 수술한 복합 치료군으로 비교하였을 때 병리적 완전 반응, 률은28%,중앙 생존 기간은 수술 단독군이17.6개월 복합, 치료군이16.9개월이었고 년 생존율은 각각, 3 16%, 30%이 었다(p=0.15).비록 통계적으로 유의한 차이는 보이지 않으 나 복합 치료군에서 생존율이 높은 경향을 보였다 이는 표. 본 수가 통계적 검정력을 가질 정도로 충분하지 않아 양군 간의 차이를 나타내지 않은 것으로 해석된다 다른. 2, 3상 연구와 마찬가지로 병리적 완전 반응을 보인 경우 그렇지, 않은 경우에 비해 생존 기간이 연장되었다.17
서울아산병원에서는1993년 월부터5 1996년 월 사이에3 명의 수술 가능한 국소적 식도암 환자를 대상으로 수술 88
전 화학 과분할 방사선 동시 치료를 시행하였다 수술에 동- . 의하지 않은 경우에는 근치적 화학 방사선 동시 치료로- 4주 기의5-FU, CDDP항암제를 투여하고 방사선, 60 Gy를 조 사하였다 중앙값. 77개월의 추적 검사 결과, intention to
에서 복합 치료를 받은 환자의 평균 생존 기간은
analysis 18
개월이고 년 생존율은, 5 23%이었다 실제 복합 치료를 받은. 환자의 경우는 평균 생존 기간은35.7개월이고 년 생존율, 5 은36.6%이었다 등록 시 수술에 동의한. 52명 환자 중41명
에서 화학 방사선 동시 치료 후 수술을 시행하
(79%) - 였고, 36
명에서 완전 절제가 가능하였으며, 43%에서 병리적 완전관 해를 보였다 수술 단독으로 치료한. matched historical 군 과 비교이기는 하나 복합 치료군에서 의미 control (n=40) ,
있게 생존 기간이 연장되었다(p=0.04).18-20 이후 본원에서 수술 전 화학 방사선 동시 치료와 수술 단독 치료를 비교하- 는 상 연구는 추적관찰 중앙값3 25개월째 시행한interim 결과 복합 치료군에서 상 연구와 비슷한 결과인
analysis 2
의 비교적 높은 병리적 관해를 얻었으나 중앙 생존 기 43%
간은28.3개월 수술 단독군은( 27.3개월 로 통계적으로 우위) 한 차이를 나타내지는 못하였다 이는 복합 치료군에서 상. 대적으로 수술 탈락률이 많이 발생한 것과 관련이 있으며, 분석에서는 복합 치료군의 생존이 우월한 경향 per protocol
을 보였다.21
에서 명의
Cancer and Leukemia Group B (CALGB) 400 환자를 대상으로 수술 전 화학 방사선 동시 치료와 수술 단- 독 치료 간의 비교 연구를 시작하였으나 환자 등록이 부진 하여 조기 중단하였다.22 궁극적으로 이러한 다영역 치료의 우월성을 증명하려면 대규모의 무작위 비교 연구를 시행해 야 하나 앞서 언급하였듯이, 400명 이상의 환자 등록을 해 야 하는 현실적 어려움이 있다. European Organization for
에서 병기 Research and Treatment of Cancer (EORTC) I, II Table 3
Table 3Table 3
Table 3 Randomized Trials of Preoperative Chemoradiotherapy vs. Surgery Alone in Resectable Esophageal Cancer
Author
Number of patients
Path CT RT (Gy)
Preoperative RT Median survival 2 yr, 3 yr
S CRT RT
Adm
pCR
(%) S CRT S CRT
Nygaard12 (1992)
47 41 Sq BP 35 Seq NS 6 7 13, 9 23, 17
Le Prise13 (1994)
41 45 Sq FP 20 Seq 10 10 11 33, 14 27, 19
Apinop14 (1994)
35 34 A/sq FP 40 Conc 20 7 10 23, 20 30, 26
Walsh15 (1996)
58 55 A/sq FP 40 Conc 22 11 16 26, 6 37, 32
Bosset16 (1997)
143 139 Sq P 37 Conc 20 18 19 42, 34 48, 36
Urba17 (2001)
50 50 Sq/A FPV 45 Conc 28 18 17 36, 16 41, 30
S; surgery alone; CRT, preoperative chemoradiotherapy; Path, pathology; CT, chemotherapy; RT, radiotherapy; RT Adm, radiotherapy administration; pCR, pathologic complete response; BP, bleomycin, CDDP; FP, 5-FU, CDDP; FPV, 5-FU, CDDP, vinblastine; Sq, squamous cell carcinoma; P, CDDP; A, adenocarcinoma; Seq, sequential; Conc, concurrent; NS, not stated; Pt, patients.
Kim SB. Combined-modality Therapy for Locoregional Esophageal Cancer
183
기 편평상피암 선암을 대상으로 수술 전 화학 방사선 동시, - 치료와 수술 단독 치료를 비교하는 상 연구가 진행 중이3 다.23
수술 전 화학 방사선 동시 치료에 대한 개의- 2 meta- analysis24,25는 수술 전 화학 방사선 동시 치료로 수술 사망- 률이 높아질 위험성은 있으나 년 사망률은 수술 단독 치, 3 료에 비해 유의하게 낮았다 또한 병리적 완전 반응률이 수. 술 전 화학 방사선 동시 치료는- 25-30%로 선행화학요법의 에 비해 높으나 치료 자체의 부작용도 크므로 진단
5-15% , ,
시 식도암 병기와 환자의 활동 능력 의료진의 경험 복합, , 치료에 대한 환자의 적극성 등을 바탕으로 제한적으로 시 행하는 것이 바람직하다.
근치적 화학 방사선 치료 - (Definitive chemoradiotherapy)
지난 년 간 근치적 화학 방사선 동시 치료는15 - 1)의학적 으로 수술을 견디기 어려운 환자, 2) 기술적으로 종양 절제 가 어려운 경우, 3)후두 인두절제술- (laryngopharyngectomy) 이 필요한 경부식도암 환자, 4)수술을 거부하는 환자, 5)비 수술적 방법을 선호하는 의료 집단, 6) 식도절제술에 관한 경험 있는 외과의사가 없는 병원에서 주로 사용되어 왔다.
년
1992 Radiation Therapy Oncology Group (RTOG) 85- 연구
01 26와 년 후 발표된 최종 보고7 27에 따르면 화학 방사- 선 동시 치료(RT 50 Gy, 5-FU, CDDP 4 )회 와 방사선 단독치 료(64 Gy)를 비교하였을 때 중앙 생존 기간은 각각, 14.1개 월, 9.3개월 년 생존율은 각각, 5 27%, 0%이었다(p<0.0001).
등록을 종료한 후 새로운 환자69명을 대상으로 앞서와 같 은 화학 방사선 동시 치료를 하였을 때 중앙 생존 기간은-
개월 년 생존율은 이었다
17.2 , 3 30% .28이상과 같이 화학 방- 사선 동시 치료가 방사선 단독 치료보다 성적이 우월하기 는 하나, 3, 4등급의 부작용이44%,생명에 위험을 줄 정도 의 부작용이 20%로 방사선 단독 치료군25%, 3%에 비해 많아 환자의 전신상태가 화학 방사선 동시 치료를 견디기- 어려운 경우에는 방사선 단독 치료만을 할 수도 있다.
수술 후 보조화학요법
(Postoperative adjuvant chemotherapy)
유방암 대장암과는 달리 식도암에서는 수술 후 보조화, 학요법에 대한 연구가 비교적 적은 데 이는 식도암 자체의, 빈도가 낮고 수술 후 합병증에 따른 환자 전신상태의 기능, 저하로 생존 기간의 작은 차이를 밝힐 만큼의 충분한 환자 를 연구에 참여시키기 어렵기 때문이다.아직까지 무작위 비교 연구에서 보조화학요법군과 수술
단독 치료군 간에 생존 기간의 차이는 없으나,29-31수술 후 회 항암제 투여시 수술 단독군에 비해 무병 5-FU, CDDP 2
생존 기간이 연장됨이 보고31된 이후 수술 후 보조화학요법 에 대한 관심을 갖게 하였다 수술 후 미세적 또는 육안적. 으로 암이 남아 있을 경우 국소적 식도암에서 화학 방사선- 동시 치료가 방사선 단독 치료에 비해 우월함을 고려할 때 환자의 전신상황이 허락하면 수술 후 보조 방사선 단독 치 료보다는 화학 방사선 동시 치료를 하는 것이 바람직할 것- 으로 예상한다.
내시경 치료(Endoscopic therapy)
근치적 치료가 어려운 경우 또는 근치적 치료 전 연하 곤란을 해소하기 위해 과거에는 내시경을 이용한 삽관술이 시도되었으나 현재는, self-expandable metallic stent가 많이 사용되고 있다.32 내시경 점막절제술은 표재성 식도암에 사 용할 수 있는 한 가지 치료법으로 식염수를 점막하층에 주 입하여 수포를 만들고 점막층과 점막하층을 벌어지게 함, 으로써 전기 조작에 의해 융기된 점막하부 병변을 제거하 는 것인데 작은 표재성 병변이나 미세침습성 병변 제거에 사용할 수 있으나 전통적인 수술 치료와 동등한 효과가 있, 는지에 관해서는 좀더 많은 자료가 필요하다.33 그 외 내시 경을 통한 레이저소작술 전기소작술 광역학 치료가 식도, , 암 치료에 일부 사용되고 있다.
향후 과제
Taxane (docetaxel, paclitaxel), irinotecan, epidermal growth 억제제
factor receptor (Irressa )와 같은 새로운 약제를 사용 하여 치료 성적을 향상시키려는 노력34,35과 치료 전 환자의 병기를 정확히 평가하는 것이 무엇보다 복합 치료의 효과 를 비교 판정하는 데 중요하므로 양성자단층촬영과 림프, 절 침범 유무 평가를 위해 최소 침습 수술의 보완이 필요하 다 또한 복합 치료에 따른 불필요한 독성과 수술 치료의 지. 연을 막기 위해서 어떤 환자가 화학 방사선 치료에 반응 또- 는 불응하는지를 예측하는 데 도움이 될 수 있는 functional imaging, molecular markers,36gene expression profile연구 들이 뒷받침되어야 하겠다.
결 론
복합 치료 시에는 치료 방법 각각의 강도와 순서 등을 적절하게 조합하는 것이 무엇보다 중요하다 이것의 적정. 성은 전체 생존 무병 생존 병리적 완전 반응 독성 삶의, , , , 질을 척도로 평가할 수 있다 식도암의 치료 성적을 향상시.
대한소화기학회지 제 권 제 호: 44 4 , 2004
184
키기 위해서는 치료와 관련된 구성원 간의 팀을 통한 치료 적 접근과 새로운 약제를 포함해서 복합 치료의 적절성을 평가하는 보다 많은 비교 임상 연구가 필요하다.
참고문헌
1. 통계청 자료 사망원인별 통계. . 2002.
(http://www.ns.go.kr)
2. Schrump DS, Altorki NK, Forastiere AA, Minsky BD.
Cancer of the esophagus. In: De Vita VT, Hellman S, Rosenberg SA. Cancer principles and practice of oncology.
6th ed. Philadelphia: Lippincott, 2001:1051-1091.
3. Malthaner R, Fenlon D. Preoperative chemotherapy for respectable thoracic esophageal cancer (Cochrane Review).
The Cochrane Library, Issue 3. Oxford: Update software 2001.
4. Kelsen DP, Gomseber R, Pajak TF, et al. Chemotherapy followed by surgery compared with surgery alone for localized esophageal cancer. N Eng J Med 1998;339:
1979-1984.
5. Medical research council oesophageal cancer working party.
Surgical resection with or without preoperative chemo- radiotherapy in esophageal cancer: a randomized controlled trial. Lancet 2002;359:1727-1733.
6. Law S, Fok M, Chow S, et al. Preoperative chemotherapy versus surgical therapy alone for squamous cell carcinoma of the esophagus: a prospective randomized trial. J Thorac Cardiovasc Surg 1997;114:210-217.
7. Kok TC, Lanschot JV, Siersema PD, et al. Neoadjuvant chemotherapy in operable esophageal squamous cell cancer:
final report of a phase III multicentre randomized controlled trial. Proc Am Soc Clin Oncol 1997;16(abstr):277A.
8. Ancona E, Ruol A, Santi S, et al. Only pathologic complete response to neoadjuvant chemotherapy improves signi- ficantly the long term survival of patients with resectable esophageal squamous cell carcinoma: final report of a randomized, controlled trial of preoperative chemotherapy versus surgery alone. Cancer 2001;91:2165-2174.
9. Clark PI. Neoadjuvant chemotherapy in esophageal cancer.
Proceeding of cancer of the esophagus and gastric cardia:
from gene to cure 2003;91(abstr):25A.
10. Urschel JD, Vasan H, Blewett CJ. A meta-analysis of randomized controlled trials that compared neoadjuvant chemotherapy and surgery to surgery alone for resectable esophageal cancer. Am J Surg 2002;183:274-279.
11. National comprehensive cancer network (http://www.nccn.org).
12. Nygaard K, Hagen S, Hansen HS, et al. Preoperative radiotherapy prolongs survival in operable esophageal carcinoma: a randomized, multicenter study of preoperative radiotherapy and chemotherapy. The second Scandinavian trial in esophageal cancer. J Surg 1992;16:1104-1109.
13. Le prise E, Etienne PL, Meunier B, et al. A randomized study of chemotherapy, radiation therapy, and surgery versus surgery for localized squamous cell carcinoma of the esophagus. Cancer 1994;73:1779-1784.
14. Apinop C, Puttisak P, Preecha N. A prospective study of combined therapy in esophageal cancer. Hepatogastro- enterology 1994;41:391-393.
15. Walsh TN, Noonan N, Hollywood D, et al. A comparison of multimodal therapy and surgery for esophageal adeno- carcinoma. N Engl J Med 1996;335:462-467.
16. Bosset JF, Gignoux M, Triboulet JP, et al. Chemo- radiotherapy followed by surgery compared with surgery alone in squamous cell cancer of the esophagus. N Engl J Med 1997;337:161-167.
17. Urba SG, Orringer MB, Turrisi A, et al. A randomized trial of preoperative chemoradiation versus surgery alone in patients with locoregional esophageal cancer. J Clin Oncol 2000;19:303-313.
18. Kim SB, Kim SH, Lee KH, et al. Concurrent chemo- radiotherapy followed by surgery for locoregional esophageal cancer: preliminary report. J Korean Med Sci 1995;1:111-120.
19. Kim JH, Choi EK, Kim SB, et al. Preoperative hyper- fractionationed radiotherapy with concurrent chemotherapy in resectable esophageal cancer. Int J Radiat Oncol Biol Phys 2001;50:1-12.
20. Lee JL, Kim SB, Jung HY, et al. The efficacy of neoadjuvant chemoradiotherapy in resectable esophageal squamous cell carcinoma: a single institutional study. Acta Oncol 2003;42:207-217.
21. Lee JL, Park SI, Kim SB, et al. A single institutional phase III trial of preoperative chemotherapy with hyper- fractionation radiotherapy plus surgery versus surgery alone for resectable esophageal squamous cell carcinoma. Ann Oncol 2004;15:947-954.
22. Kelsen D. Preoperative chemoradiotherapy for esophageal cancer. J Clin Oncol 2001;19:283-285.
23. Bosset JF, Mercier M, Triboulet JP, et al. Surgical resection with and without chemotherapy in oesophageal cancer.
Lancet 2002;360:1173-1174.
24. Fiorica F, Di Bona D, Schepis F, et al. Preoperative chemoradiotherapy for oesophageal cancer: a systematic
김성배 국소적 식도암에서 복합 치료.
185
review and meta-analysis. Gut 2004;53:925-930.
25. Urschel KD. Vasan H. A meta-analysis of randomized controlled trials that compared neoadjuvant chemoradiation and surgery to surgery alone for resectable esophageal cancer. Am J Surg 2003;18:538-543.
26. Herskovic A, Martz K, Al-Sarraf M, et al. Combined chemotherapy and radiotherapy compared with radiotherapy alone in patients with cancer of the esophagus. N Engl J Med 1992;326:1593-1598.
27. Cooper JS, Guo MD, Herskovic A, et al. Chemoradiotherapy of locally advanced esophageal cancer: long-term follow-up of a prospective randomized trial (RTOG 85-01). Radiation therapy oncology group. JAMA 1999;281:1623-1627.
28. Al-Sarraf M, Martz K, Kerskovic A, et al. Progress report of combined chemoradiotherapy versus radiotherapy alone inpatients with esophageal cancer; an Intergroup study. J Clin Oncol 1997;15:277-284.
29. Pouliquen X, Levard H, Hay JM, McGee K, Fingerhut A, Langlois-Zantin O. 5-Fluorouracil and cisplatin therapy after palliative surgical resection of squamous cell carcinoma of the esophagus. A multicenter randomized trial. French associations for surgical research. Ann Surg 1996;223:
127-133.
30. Ando N, Iizuka T, Kakegawa T, et al. A randomized trial of surgery with and without chemotherapy for localized squamous carcinoma of the thoracic esophagus: the Japan
Clinical Oncology Group Study. J Thorac Cardiovasc Surg 1997;114:205-209.
31. Ando N, Iizuka T, Ide H, et al. Surgery plus chemotherapy compared with surgery alone for localized squamous cell carcinoma of the thoracic esophagus: a Japan clinical oncology group study-JCOG9204. J Clin Oncol 2003;
21:4592-4596.
32. Song HY, Park SI, Jung HY, et al. Benign and malignant esophageal strictures: treatment wiith a polyurethane- covered retrievable expandable metallic stent. Radiology 1997;203:747-752.
33. Lamber R. Endoscopic mucosectomy: an alternative treatment for superficial esophageal cancer. Recent Results Cancer Res 2000;155:183-192.
34. Bains MS, Stojadinovic A, Minsky B, et al. A phase II trial of preoperative combined-modality therapy for localized esophageal carcinoma: initial results. J Thorac Cardovasc Surg 2002;124:270-277.
35. Ilson DH, Minsky B, Kelsen D. Irinotecan, cisplatin, and radiation in esophageal cancer. Oncology (Huntingt) 2002;
16:11S-15S.
36. Kim SB, Kim SH, Jung HY, et al. The prognostic signi- ficance of the p53 overexpression on complete response and survival in preoperative chemoradiotherapy treated squamous cell esophageal carcinoma. J Korean Cancer Assoc 1998;30:
278-287.