Comparison of Teriparatide and Calcitonin Treatment in Postmenopausal Korean Women with Osteoporosis
Woong Hwan Choi
1, Ghi Su Kim
2, Sung Kil Lim
3, Moo Il Kang
4, Hyun Koo Yoon
5, Yong Ki Min
6, Chan Soo Shin
7, Maria Yu
8, Belinda J Hall
8, Daniel Thiebaud
9Division of Endocrinology, College of Medicine, Hanyang University, Seoul, Korea1, Asan Medical Center, College of Medicine, University of Ulsan, Seoul, Korea2,
College of Medicine, Yonsei University, Seoul, Korea3, Catholic University of Korea, St. Mary’s Hospital, Seoul, Korea4,
School of Medicine, Sungkyunkwan University, Seoul, Korea5,
Samsung Medical Center, Seoul, Korea6, Seoul National University, Seoul, Korea7 Intercontinental Information Sciences (ICIS)8, Eli Lilly Australia Pty Limited9
목적: 이 연구의 목적은 골다공증으로 확진된 폐경 후 여성에서 teriparatide와 calcitonin치료가 요추와 대퇴골 골밀도와 생화학적 골 표지자 (bone-specific alkaline phosphatase [BSAP] and osteocalcin)에 미치는 효과와 안정성을 비교하는 것이다.
방법: 한국에서 시행된 이 개방 표지, 다기관, 대조군 연구에서 골다공증이 있는 70명의 폐경 후 여성이 teripa- ratide 20μg/일 (n=35) 또는, calcitonin 100 IU/일 (n=35)을 6개월 간 피하로 투여 받는 군으로 임의로 나누어졌 다. 모든 환자들은 연구 기간 동안 칼슘 (≥500 mg/일)과 비타민 D (200 to 400 IU/day)를 투여 받았다.
결과: 모든 환자들은 한국인으로, 연령은 55세에서 82세 사이로 (66±5 years; mean±SD) 이전에 1회 이상 골절을 경험한 적이 있었다. teriparatide군에서는, calcitonin군의 23명 (66%)의 환자에 비해 31명 (81%)의 환자가 이 연 구 계획을 모두 수행하였다 (P=.044). teriparatide 치료를 받은 환자들에서, 요추 골밀도가 4.2±5.9% (mean±SD;
P=.555) 증가하였고, calcitonin 치료를 받은 환자들에서 0.6±5.5% (mean±SD; P=.555)가 증가하였다. 양 군에서 치료 시작부터 종결 시점까지 요추 골밀도 변화의 보정된 평균 차이는 3.8% (95% CI: 0.94~6.57, P=.010)였다.
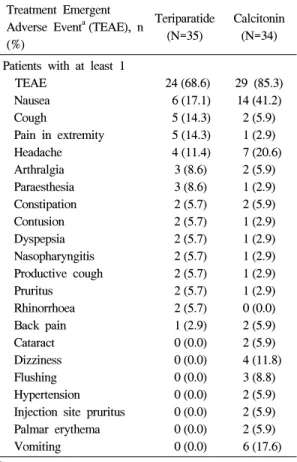
Teriparatide 치료는 전체 대퇴골 (P=.658), 전자 (P=.056), 또는 경부 (P=.442) 골밀도에 통계적으로 의미 있는 영향 을 미치지는 못했다. Calcitonin 치료는 전체 대퇴골 골밀도에서 2.2±4.6% (mean±SD; P=.029)의 통계적으로 의 미 있는 감소를 초래한 반면, 전자 (P=.641) 또는 대퇴골 경부 (P=.216) 골밀도에는 의미 있는 감소를 초래하지 않았 다. Teriparatide 치료는 혈청 bone-specific alkaline phosphatase (BSAP) and osteocalcin의 농도를 치료 시작 전보다 각각 116% (median change, range-31 to 599%; P<.001)와 172% (median change, range-62 to 571%; P<.001) 증가시켰다. Calcitonin 치료는 혈청 BSAP 또는 osteocalcin 농도에 통계적으로 의미 있는 영향을 미치지는 않았다. teriparatide 치료 군에서, calcitonin 치료 군에서는 85%에 비해, 69%의 환자가 1가지 이상의 치료와 연관된 부작용을 경험하였다 (P=.154). 양 치료 군에서 가장 흔한 치료와 연관된 부작용은 오심이었고, teri- paratide 치료 군에 비해 calcitonin 치료 군에서 더 많이 나타났다 (41% versus 17% respectively; P=.036). 양 치료군에서 기타 실험실 검사 또는 활력 징후의 임상적으로 의미 있는 차이는 관찰되지 않았다.
결론: 이 연구는 teriparatide가 요추 골밀도뿐만 아니라, 골형성 생화학적 표지자인 BSAP and osteocalcin의 증 가를 일으킨 것으로 보아, 한국의 폐경 후 여성의 골다공증에 효과적인 치료제라는 것을 보여준다. teriparatide 치료는 calcitonin치료에 비해 요추골 골밀도의 의미 있는 증가를 가져왔다. 두 치료 모두 모든 환자에서 안전하였 고, 특별한 부작용이 없었다.
중심단어: Teriparatide, Calcitonin, 골다공증, 폐경 후 여성
책임저자 : Daniel Thiebaud, Eli Lilly Australia Pty Limited
Tel: +61-2-93254606, Fax: +61-2-93254699, E-mail: [email protected]
* This study was supported by funding from Eli Lilly & Co.
Osteoporosis is a disease characterised by compro- mised bone strength leading to increased fracture susceptibility. Currently, the most common treatments for osteoporosis include calcium and vitamin D supplementation, estrogens, bisphosphonates, raloxi- fene, and calcitonin
1,2. These agents are all antire- sorptive, thus they stabilise bone mass and prevent further bone loss. This means that antiresorptive treat- ments can increase BMD and reduce fracture risk, however they do not usually produce large increases in bone mass.
Recently, the effects of the bone formation- stimu- lating agent teriparatide, biosynthetic human parathy- roid hormone (rhPTH [1-34]), have been demonstrated in women with postmenopausal osteoporosis. Teri- paratide treatment has been associated with increases in BMD and bone formation markers and importantly, a reduced fracture risk in these patients due to its anabolic action on bone
3,4. Dramatic increases in BMD have also been observed in postmenopausal women with osteoporosis receiving a combination of hormone replacement therapy (HRT) and teriparatide compared with HRT alone
5,6.
Calcitonin is a widely used treatment for osteo- porosis. It is a natural peptide secreted by the thyroid gland and has a well known role in humans in the short-term fine tuning of calcium homeostasis. Calci- tonin binds to high-affinity receptors on osteoclasts and causes an inhibition of activity
7. Clinical experi- ence has shown that the most effective form of calcitonin for osteoporosis treatment is salmon calci- tonin, available as a subcutaneous injection or nasal spray
8-10. Some early studies supported the use of calcitonin in the prevention and treatment of involu- tioal osteoporosis with the use of 100 IU of salmon calcitonin injected subcutaneousl y
11,12. Salmon calci- tonin is usually relatively safe, with some reports of transient facial flushing, nausea, mild inflammation at the injection site, and very rarely, vomiting and dia- rrhoea.
The current study was part of a registration study and it is the first study to compare teriparatide treat- ment with calcitonin treatment in Korean patients. The aims of this study were to compare in postmeno- pausal Korean women with established osteoporosis the effect of treatment with teriparatide 20μg/day administered subcutaneously with the effect of salmon calcitonin 100 IU/day administered subcutaneously on changes in BMD, biochemical bone markers (bone- specific alkaline phosphatase [BSAP] and osteocal- cin), and safety.
Methods 1. Study Design
This was an open-label, controlled, randomised study with two treatment arms conducted in seven centres in Korea (study code B3D-KL-GHCC). Se- venty postmenopausal women with established osteo- porosis, as determined by at least one prevalent vertebral or nonvertebral osteoporotic fracture, were enrolled. The study included a 6-month treatment phase after a screening period of 2 months. Eligibility requirements were fulfilled and baseline procedures were carried out during the screening phase. At this time, all patients began taking supplements of at least 500 mg/day of elemental calcium and 200 to 400 IU/day of vitamin D.
During the treatment phase, study visits occurred at 0 (baseline), 1, 3, and 6 months. Patients were ran- domised to treatment with either teriparatide (20μ g/day) or calcitonin (100 IU/day) at the baseline visit using the Interactive Voice Response System (IVRS).
Teriparatide 20μg (Forteo
Ⓡ, Eli Lilly & Co., Ltd.)
was provided in pre-filled cartridges placed in Gemini
PTH pen injection devices. Calcitonin was provided in
prefilled disposable syringes containing 100 IU of
salmon calcitonin (Miacalcic
Ⓡ, Novartis). Each pa-
tient was instructed to inject either teriparatide or
calcitonin into her left or right lower abdomen or outer thigh in the early morning on a daily basis during the study treatment. At the baseline visit, the patient administered the first dose of teriparatide or calcitonin under supervision at the study site. The last injection of teriparatide or calcitonin took place the day before the last visit (6 months).
2. Study Population
Postmenopausal women aged 55 to 85 years (at least 3 years had elapsed after menopause), inclusive, with established osteoporosis as defined by a previous, documented (X-ray), vertebral (evaluated on lateral views of the thoracic and lumbar spine) or nonvertebral osteoporotic fragility fracture (excluding major trauma), and who were free of severe or chronically disabling conditions other than osteo- porosis, were eligible for inclusion in this study. L-1 through L-4 vertebrae were required to be without artefacts or multiple vertebral fractures, and the reading of the BMD T-score was required to be in the range of -2.0 and -4.0 for at least one of the two sites measured (spine or hip). Patients with a history of diseases which affect bone metabolism, any secondary causes of osteoporosis, an increased base- line risk of osteosarcoma, significantly impaired hepa- tic, renal, or gastric function, a history of other malig- nant neoplasms in the 5 years prior to screening, a history of nephrolithiasis or urolithiasis in the 2 years prior to Visit 2, or treatment with any drug known to significantly affect bone metabolism in the 6 months prior to Visit 2, were excluded from the study.
3. Measures
The primary measure of efficacy was the percent change in lumbar spine BMD from baseline to endpoint measured by dual energy x-ray absorp- tiometry (DXA) at the end of 6 months or at the early
termination visit. Secondary measures of efficacy were the percent changes from baseline to endpoint in total hip, femoral neck, and trochanter BMD. All BMD measurements were performed using DXA using Hologic or Lunar equipment. Further secondary measures of efficacy were percent changes from baseline to 3 months and from baseline to endpoint (6 months or last observation carried forward [LOCF]) in the biochemical bone markers bone- specific alkaline phosphatase (BSAP) and osteocalcin. Adverse events were collected at every visit, regardless of relationship to study drug. These events were captured as actual terms and coded to Medical Dictionary for Regulatory Activities (MedDRA) terms. Physical examinations, including measurement of heart rate and blood pressure, and the recording of self-reported fractures were also carried out at each visit. Quantification of returned study materials at each visit allowed percent compliance to be calculated based on the amount of medication injected as a percentage of the total amount prescribed for that period. Any patient who missed more than 50% of the injectable study medi- cation in any one of the visit intervals was considered noncompliant.
4. Statistical Analyses
All efficacy analyses were performed on an
intention-to-treat (ITT) basis, and were based on data
from patients with at least one observation post-
randomisation. Safety analyses were performed on
patients who had taken at least one dose of study
medication. For confirmatory purposes, a per-protocol
population was used to assess the robustness of the
results from the analysis of the primary and secondary
efficacy variables. This population excluded patients
who violated the inclusion/exclusion criteria, who did
not complete the study, or who received prohibited
concomitant medications. A LOCF approach was used
for patients who discontinued prior to the end of the
treatment period.
For the BMD data, standardised values for lumbar spine and total hip (sBMD) were used for analysis.
For femoral neck and trochanter BMD, raw values were used for analysis. For change from baseline analysis, both change and percent change from base- line were calculated. The initial analysis of covariance (ANCOVA) model for BMD measures included effects of treatment, baseline value, centre, and treat- ment by centre interaction. None of the BMD vari- ables had significant treatment by centre interaction at a 0.10 level of significance. Therefore, all analyses were performed using ANCOVA without the interac- tion. Rank analysis of covariance was used for the biochemical bone marker (BSAP and osteocalcin) analysis since the data were generally not normally distributed. To analyse the changes from baseline within treatment groups, a paired t-test or signed-rank test was used. All statistical tests were two-sided and conducted at 0.05 level of significance.
The targeted number of patients to be included in this study was 64, as this was the number required (based on a dropout rate of approximately 20%) to provide 80% power to detect a treatment group difference of 4% at a two-sided 0.05 alpha level. No adjustments for multiple comparisons were made.
Results
1. Patient Disposition and Baseline Demo- graphics
A total of 156 patients were entered into the screening phase. Of these, 70 patients were enrolled into the study and randomly assigned to receive study treatment (n=35 teriparatide, n=35 calcitonin), compri- sing the ITT population. Efficacy analyses were carried out on ITT patients with at least one post- baseline measurement and were repeated on the per- protocol population for confirmatory purposes (n=51
overall; n=29 teriparatide, n=22 calcitonin). One patient in the calcitonin group did not meet protocol entry criteria and was withdrawn without receiving study medication, thus safety analyses were carried out on 69 patients.
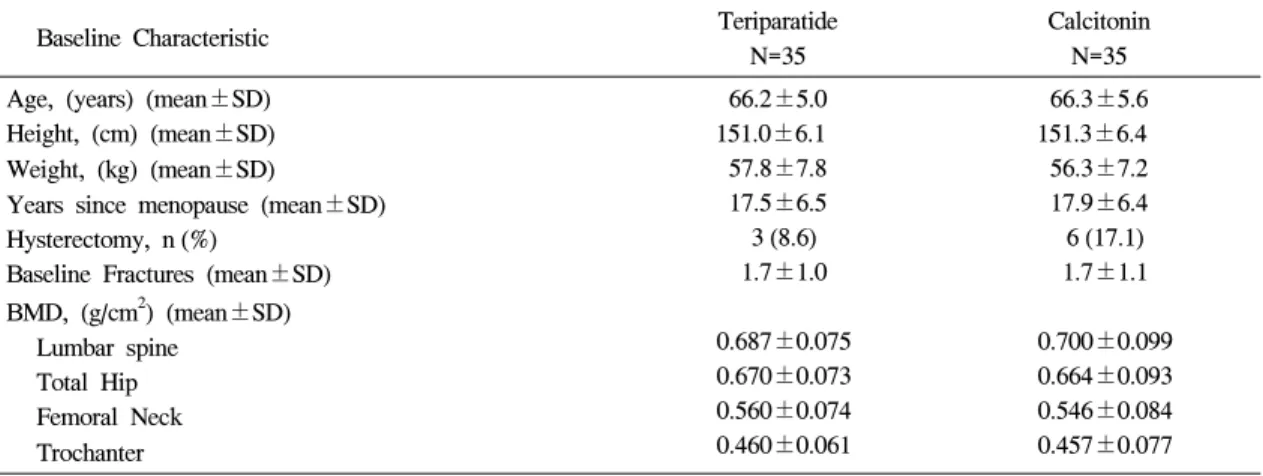
The specific characteristics of the patients that were examined at study enrolment were age, origin, height, and baseline fracture data. The mean age of all randomised patients was 66.2 years (66.2 years in the teriparatide group and 66.3 years in the calcitonin group). All randomised patients were Korean, with a mean height and weight prior to treatment of 151.16
cm (151.04 cm in the teriparatide group and 151.27 cm in the calcitonin group) and 57.03 kg (57.79 kg in the teriparatide group and 56.27 kg in the calcitonin group) respectively. The number of fractures present prior to study treatment was 61 in the teriparatide group and 59 in the calcitonin group, with the number of fractures per patient ranging from one to five in each group. These data as well as other baseline medical characteristics are summarised in Table 1.
The two treatment groups were generally well ba- lanced at baseline in terms of historical diagnoses, pre- existing conditions, previous osteoporosis medi- cation, and concomitant medication.
Of the 35 patients in the teriparatide group, 31 (88.6%) patients completed the protocol compared with 23 of the 35 (65.7%) patients in the calcitonin group (Table 2). This difference was statistically signi- ficant (P=.044). Patients who received calcitonin on average spent fewer days on therapy (131.9 days) than patients who received teriparatide (166.9 days). At the end of Month 1, average percentage compliance was lower in the calcitonin treatment group compared with the teriparatide treatment group, with values of 97.9%
and 78.3% respectively. Month 3 compliance was si-
milar for both treatment groups (90.3% and 90.2% for
teriparatide and calcitonin respectively), however, by
this time, 10 patients from the calcitonin group had
discontinued compared with one patient from the
Table 1. Patient characteristics
Baseline Characteristic Teriparatide
N=35
Calcitonin N=35 Age, (years) (mean±SD)
Height, (cm) (mean±SD) Weight, (kg) (mean±SD)
Years since menopause (mean±SD) Hysterectomy, n (%)
Baseline Fractures (mean±SD) BMD, (g/cm2) (mean±SD)
Lumbar spine Total Hip Femoral Neck Trochanter
66.2±5.0 151.0±6.1 57.8±7.8 17.5±6.5 3 (8.6) 1.7±1.0
0.687±0.075 0.670±0.073 0.560±0.074 0.460±0.061
66.3±5.6 151.3±6.4 56.3±7.2 17.9±6.4 6 (17.1) 1.7±1.1
0.700±0.099 0.664±0.093 0.546±0.084 0.457±0.077 Abbreviations, BMD=bone mineral density, SD=standard deviation.
Table 2. Completion rates and reasons for discontinuation
Teriparatide (N=35)
n, %
Calcitonin (N=35)
n, %
P-valuea
Completion Rate
Reason for discontinuation, Adverse Event
Personal conflict or other patient decision Protocol entry criteria not met
31 (88.6)
1 (2.9) 3 (8.6) 0 (0)
23 (65.7)
3 (8.6) 8 (22.9)
1 (2.9)
0.044
aFisher’s Exact Test
Fig. 1. Mean percent change in BMD from baseline to endpoint.
teriparatide group. Month 6 compliance was 95.8%
and 88.7% for the teriparatide and calcitonin treatment groups respectively.
2. Bone Mineral Density
The primary efficacy endpoint of this study was to compare the percentage change from baseline to endpoint in lumbar spine BMD. Teriparatide treatment was associated with a mean percentage increase from baseline in lumbar spine BMD of 4.2±5.9% (mean±
SD, P<.001). No statistically significant change in lumbar spine BMD was observed in the calcitonin treatment group (mean change from baseline of 0.6±5.5%, P=.555; Fig. 1). There was a statistically significant difference between the two treatment
groups in the percentage change from baseline to endpoint (adjusted mean difference of 3.8%, 95% CI:
0.94, 6.57, P=.010). Table 3 shows the adjusted mean
Table 3. Adjusted mean difference (AMD) between treatment groups for the percent change from baseline to endpoint in BMD superscript
Area ITT Population Per protocol population
AMD 95% CI P-valuea AMD 95% CI P-valuea
Lumbar Spine 3.76 0.94-6.57 0.0098 3.70 0.18-7.22 0.0399
Total Hip 1.85 -0.10-3.81 0.0629 2.44 0.14-4.74 0.0380
Femoral Neck 0.38 -2.28-3.04 0.7764 0.82 -2.30-3.94 0.6000
Trochanter 1.44 -0.64-3.51 0.1711 1.22 -1.36-3.80 0.3460
aP-value from ANCOVA with treatment, baseline and centre in the model, Abbreviations: BMD=bone mineral density.
Fig. 2. Median percentage change (± interquartile range (IQR)) in serum levels of (a) BSAP and (b) osteocalcin, from baseline to 3 and 6 months post-treatment.
difference between the two treatment groups for each of the BMD measurements for both the ITT and the per- protocol populations.
Teriparatide treatment had no significant effect on total hip BMD while calcitonin treatment was associated with a slight yet statistically significant mean decrease in total hip BMD of 2.2 ± 4.6%
compared to baseline (mean ± SD, P=.029; Fig. 1).
The difference between the two treatment groups in the mean percentage change from baseline to endpoint was not statistically significant in the ITT population
(adjusted mean difference of 1.9%, 95% CI: -0.10, 3.81, P=.063), however, it was statistically significant in the per-protocol population (adjusted mean diffe- rence of 2.4%, 95% CI: 0.14, 4.74, P=.038; Table 3).
No statistically significant differences were observed in either treatment group for the mean change from baseline to endpoint in femoral neck or trochanter BMD.
3. Bone Markers
Median baseline values for serum BSAP were 11.9 μg/L and 14.2μg/L in the teriparatide and calcitonin treatment groups respectively. In the teriparatide treat- ment group, there were median percentage increases in BSAP of 85% at 3 months (P<.001) and 116% at 6 months (P<.001) compared to baseline (Fig. 2a). In the calcitonin treatment group, the median percentage increases in BSAP were not statistically significant
(3.9% at 3 months and 3.5% at 6 months compared to baseline; P=.157 and P=.725 respectively). In addition, a statistically significant median percentage difference between the two treatment groups was observed at Months 3 and 6 (P<.001 for both periods).
Median baseline values for serum osteocalcin were
Table 4. Adverse events
Treatment Emergent Adverse Eventa(TEAE), n (%)Teriparatide (N=35)
Calcitonin (N=34) Patients with at least 1
TEAE Nausea Cough
Pain in extremity Headache Arthralgia Paraesthesia Constipation Contusion Dyspepsia Nasopharyngitis Productive cough Pruritus Rhinorrhoea Back pain Cataract Dizziness Flushing Hypertension Injection site pruritus Palmar erythema Vomiting
24 (68.6) 6 (17.1) 5 (14.3) 5 (14.3) 4 (11.4) 3 (8.6) 3 (8.6) 2 (5.7) 2 (5.7) 2 (5.7) 2 (5.7) 2 (5.7) 2 (5.7) 2 (5.7) 1 (2.9) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0)
29 (85.3) 14 (41.2) 2 (5.9) 1 (2.9) 7 (20.6)
2 (5.9) 1 (2.9) 2 (5.9) 1 (2.9) 1 (2.9) 1 (2.9) 1 (2.9) 1 (2.9) 0 (0.0) 2 (5.9) 2 (5.9) 4 (11.8)
3 (8.8) 2 (5.9) 2 (5.9) 2 (5.9) 6 (17.6)
aReported by at least 5% of patients from either treat- ment group.