골다공증이 있는 한국 폐경 여성에서 1년의 Teriparatide 치료 후 골밀도와 골교체 표지자
관동대학교 의과대학 제일병원 가정의학교실
박선영․배재훈․김주영․오한진․주일우
Bone Mineral Density and Bone Turnover Markers after One-year Teriparatide Treatment in Korean Postmenopausal Women with Osteoporosis
Seon Young Park, Jae Hoon Bae, Joo Young Kim, Han Jin Oh, Il Woo Joo Department of Family Medicine, Cheil General Hospital & Women’s Healthcare Center,
College of Medicine, Kwandong University, Seoul, Korea
Objectives: Recombinant teriparatide, a bone anabolic agent, is known to result in a net positive bone balance and reduce vertebral and nonvertebral fracture incidence. The objective of this study was to evaluate the changes of bone mineral density (BMD) and bone turnover markers after one-year teriparatide treatment in Korean postmenopausal women with osteoporosis.
Methods: The enrolled postmenopausal women with osteoporosis were administered teriparatide 20μg/
day injection for one year. BMD at the lumber spine and the hip were measured at baseline and after one year by dual-energy X-ray absorptiometry. Also, serum bone turnover markers, such as osteocalcin, C-telopeptide of collagen cross-links (CTX), and alkaline phosphatase were measured at baseline and after one year.
Results: Lumbar spine BMD increased from baseline (4.4%, P<0.01), but femoral neck BMD decreased from baseline (-9.7%, P<0.05). Bone turnover markers, such as osteocalcin (148.5%), CTX (67.6%), and alkaline phosphatase (56.7%) increased from baseline (P<0.001 for all).
Conclusion: One year of teriparatide treatment significantly increased lumbar spine BMD and bone turnover markers in Korean postmenopausal women with osteoporosis. The large-populated prospective study with longer administered period will be needed in the future.
Key Words: Osteoporosis, Teriparatide, Bone mineral density, Bone turnover marker, ostmenopausal women
Received: November 22, 2009 Revised: December 1, 2009 Accepted: December 21, 2009
Corresponding Author: Il Woo Joo, Department of Family Medicine, Cheil General Hospital & Women’s Healthcare Center, College of Medicine, Kwandong University, 1-19 Mukjeong- dong, Jung-gu, Seoul 100-380, Korea
Tel: +82-2-2000-7159, Fax: +82-2-2000-7896 E-mail: [email protected]
골다공증은 골 강도가 약화되어 골절의 위험을 증 가시키는 골격계 질환으로1, 미국의 경우 약 천만 명 이 골다공증에 이환되어 있으며 3천 4백만 명이 낮 은 골밀도로 인해 골다공증에 이환될 위험에 처해있 다고 한다2. 국내에서는 아직까지 골다공증에 대한
광범위한 역학조사가 없으나, 울산지역의 만 49~54 세 사이 폐경 주변기 여성 1,020명을 대상으로 이중 에너지 방사선 흡수법(duel-energy X-ray absorptio- metry, DXA)을 이용해 요추 및 대퇴골 골밀도를 측 정한 연구에서 요추 골다공증은 9.8%, 대퇴골 골다 공증은 1.4%를 보이고 있다3. 전 세계적으로 인구의 고령화에 발맞추어 골다공증의 유병률 또한 증가할 것이고, 이로 인한 사회경제적 손실 또한 함께 증가 할 것이다. 따라서 골다공증을 예방하고 진단하여 치료하는 것은 매우 중요하다.
골다공증의 치료 약제는 크게 골흡수 억제제와 골 형성 촉진제가 있다4,5. 재조합 부갑상선 호르몬인 teriparatide는 골형성 촉진제의 하나로 조골세포뿐 아니라 파골세포도 활성화시켜 골형성과 골흡수 모 두를 촉진시키지만, 간헐적으로 투여되었을 때에는 결과적으로 골형성을 유도한다6,7. Teriparatide는 여 러 임상연구에서 피질골과 해면골을 형성시키고8,9 골강도를 증가시킬 뿐 아니라10 척추 및 비척추 골절 을 감소시킴이 관찰되었다9. Teriparatide는 2002년 미 국에서 처음으로 승인받아 사용되기 시작하였고, 현 재 심한 골다공증의 치료와 골절의 위험이 높은 경 우 및 골흡수 억제제 치료에 만족스럽지 못한 반응 을 보이는 경우 처방하도록 권고되고 있다11,12. 국내 에서는 2007년부터 골다공증 치료제로 승인받아 사 용되고 있다.
지금까지 teriparatide의 골밀도 및 골절에 대한 효과 를 살펴본 국외의 연구들은 많았다. 대표적인 연구로 2008년에 발표된 EUROPOS (the EUROpean study of FOSteo)가 있다13-15. 이 연구는 골다공증이 있는 폐경 여성을 대상으로 2년 동안 진행되었는데, 전체 대상 자들은 1년 동안 공통적으로 teriparatide 치료를 받았 고 그 후 1년은 세부연구목적에 따라 두 군으로 나뉘 어 연구가 진행되었다. 그러나 아직까지 국내에서는 teriparatide의 골밀도 및 골절에 대한 효과를 알아 본 연구가 없다. 현재 국내에서 teriparatide는 비급여로 처방되는 고가의 약제이고 매일 피하주사를 해야 하 는 번거로움 등으로 인해 치료가 제한적으로 이루어 지고 있으며 환자의 대부분은 teriparatide 치료 전에 골흡수 억제제로 장기간 치료받게 된다. 따라서 본 연구에서는 골다공증으로 인해 골흡수 억제제로 치
료를 받아오던 한국의 폐경 여성에게 1년간 teri- paratide를 투여했을 때 보이는 요추와 대퇴골의 골밀 도 및 골교체 표지자의 변화를 살펴보기로 하였다.
대상 및 방법
1. 연구 대상자
골다공증이 있는 폐경 여성으로 골흡수 억제제로 치료를 1년 이상 받은 사람 가운데 2007년 5월부터 2009년 4월까지 서울 소재 일개 종합병원 갱년기 클 리닉을 방문하여 teriparatide로 약제 변경을 한 후 1 년 동안 치료받은 자를 대상으로 후향적 연구를 시 행하였다.
골다공증 이외의 골 대사 질환이나 갑상선 질환으 로 치료 중인 경우, 최근 12개월 이내에 전신적인 스 테로이드 치료를 받은 병력이 있는 경우, 유방암이 나 자궁내막암과 같이 여성 호르몬과 관련한 암이 있는 경우, 최근 5년 이내에 유방암이나 자궁내막암 과 같이 여성호르몬과 관련 있는 암 이외의 암을 진 단받은 경우, 간이나 신기능에 장애가 있는 경우, 여 성호르몬을 병용투약 받은 경우를 제외하였으며 총 연구 대상자는 18명이었다.
Teriparatide로 변경 전에 사용한 골흡수 억제제의 종류와 칼슘 및 비타민 D의 병용투여 여부는 제한 하지 않았다.
2. 연구 방법
연구 대상자의 병록 기록을 통해 병력, 약물 복용 력, teriparatide 투여 시작 시기와 지속 여부 및 치료 종결 시기를 비롯하여 신체 계측치, 골밀도, 골교체 표지자, 그리고 혈액검사결과를 확인하였다.
신장과 체중은 가벼운 옷을 입은 상태에서 각각 자동 신체 계측기(모델명: DS-102, 제작사: ㈜동산제 닉스, Korea)와 생체 전기저항 분석법(Bioelectrical impedance analysis, BIA)을 이용한 체성분 분석기(모 델명: InBody 3.0, 제작사: Biospace, Korea)를 사용하 여 측정되었고, 체중(kg)을 신장(m)의 제곱으로 나누 어 체질량지수(Body mass index, BMI, kg/m2)를 계산 하였다. 체지방률은 체성분 분석기를 통해 얻어졌다.
골밀도는 teriparatide 치료 시작 전과 치료 1년 후
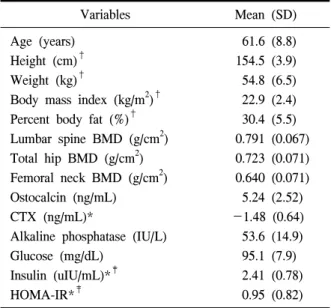
Variables Mean (SD) Age (years)
Height (cm)† Weight (kg)†
Body mass index (kg/m2)† Percent body fat (%)† Lumbar spine BMD (g/cm2) Total hip BMD (g/cm2) Femoral neck BMD (g/cm2) Ostocalcin (ng/mL) CTX (ng/mL)*
Alkaline phosphatase (IU/L) Glucose (mg/dL)
Insulin (uIU/mL)*‡ HOMA-IR*‡
61.6 (8.8) 154.5 (3.9) 54.8 (6.5) 22.9 (2.4) 30.4 (5.5) 0.791 (0.067) 0.723 (0.071) 0.640 (0.071) 5.24 (2.52)
-1.48 (0.64) 53.6 (14.9) 95.1 (7.9) 2.41 (0.78) 0.95 (0.82)
†n=15, ‡n=11. *Variables were transformed logarith- mically to normalize the distribution before analysis.
Abbreviations: SD, standard deviation; BMD, bone mine- ral density; CTX, C-telopeptide of collagen cross-links;
HOMA-IR, homeostasis model assessment of insulin re- sistance.
Table 1. Baseline characteristics of the subjects (n=18) 에 이중에너지 방사선 흡수법(dual-energy X-ray ab-
sorptiometry, DXA)을 이용한 QDR 4500 (Hologic Inc., USA)으로 요추 L2-L4와 대퇴골에서 측정하였다.
골교체 표지자로 골형성 표지자인 osteocalcin, alkaline phosphatase와 골흡수 표지자인 C-telopeptide of collagen cross-links (CTX)를 혈액검사결과를 통해 얻었다.
연구 대상자는 매일 teriparatide 20μg을 자가로 피 하 주사하였다.
골다공증은 세계보건기구(World health organiza- tion, WHO)의 견해에 따라 대퇴골 전체, 대퇴골 경 부 혹은 요추 중 한 곳이라도 T-score가 -2.5 이하인 경우로16, 폐경은 마지막 생리 후 1년 이상 무월경이 지속되는 경우로 정의하였다17.
3. 통계 분석
연구 대상자의 teriparatide 투여 전 일반적 특성은 평균과 표준 편차로 나타내었다.
Teriparatide 투여 전과 투여 1년 후의 요추 및 대 퇴골의 골밀도 변화와 골교체 표지자의 변화를 비교 하기 위해서 대응 표본 T-검정(paired T-test)을 사용 하였으며, P-value 0.05 미만을 통계적으로 유의하다 고 간주하였다.
모든 통계분석은 SPSS (Statistical Program for Social Science) version 12.0을 사용하여 시행하였고, CTX, insulin, HOMA-IR은 정규성을 이루지 않아 자 연 log로 치환한 후 분석하였다.
결 과
1. 연구 대상자의 일반적 특성
연구 대상자의 teriparatide 투여 전 일반적 특성은 Table 1과 같다.
이들은 모두 골다공증이 있는 폐경 여성으로 평균 연령은 61.6±8.8세였고, 평균 체질량 지수는 22.9±
2.4 kg/m2, 평균 체지방률은 30.4±5.5%였다.
요추의 평균 골밀도는 0.791±0.067 g/cm2였고, 대 퇴골 전체와 경부의 평균 골밀도는 각각 0.723±
0.071 g/cm2, 0.640±0.071 g/cm2였다.
골교체 표지자의 평균은 osteocalcin의 경우 5.24±
2.52 ng/mL, CTX는 -1.48±0.64 ng/mL, alkaline phos- phatase 53.6±14.9 IU/L였다.
2. 골밀도의 변화
연구 대상자의 teriparatide 투여 1년 후 요추와 대 퇴골 골밀도 변화를 투여 전과 비교하였다.
Teriparatide 투여 1년 후 요추의 골밀도는 평균 0.035 g/cm2 (4.4%, P<0.01) 증가하였고, 대퇴골 경부 골밀도는 평균 0.062 g/cm2 (9.7%, P<0.05) 감소하였 다(Fig. 1).
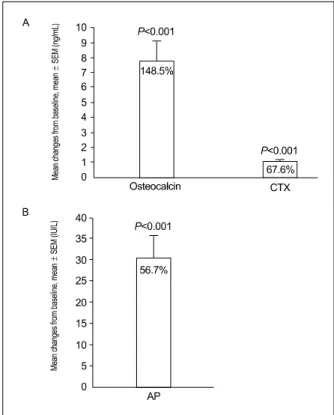
3. 골교체 표지자의 변화
Teriparatide 투여 1년 후 골교체 표지자인 osteocal- cin, alkaline phosphatase 및 CTX는 투여 전과 비교 시 모두 통계적으로 유의하게 증가하였는데, osteo- calcin은 평균 7.78 ng/mL (148.5%, P<0.001), CTX는 1.00 ng/mL (67.6%, P<0.001), 그리고 alkaline phos- phatase는 30.39 IU/L (56.7%, P<0.001) 증가하였다 (Fig. 2).
Fig. 1. Mean BMD changes from baseline after one- year of teriparitide treatment at lumbar spine, total hip, and femoral neck (mean±SEM).
Percent changes from mean baseline bone mineral density were shown within each bar.
Abbreviations: BMD. Bone mineral density;
SEM, standard error of the mean P-value<0.05 by paired T-test.
Fig. 2. Mean bone turnover markers changes from baseline after one-year of teriparitide treatment (mean±SEM): a, osteocalcin and CTX; b, AP.
Percent changes from mean baseline bone turnover marker were shown within each bar.
*Variables were transformed logarithmically to normalize the distribution before analysis.
Abbreviations: BMD, Bone mineral density;
SEM, standard error of the mean; CTX, C- telopeptide of collagen cross-links; AP, alkaline phosphatase P-value<0.05 by paired T-test.
고 찰
본 연구에서는 골다공증이 있는 폐경 여성 가운데 골흡수 억제제로 1년 이상 치료받은 사람을 대상으 로 1년 동안 teriparatide 치료 후 골밀도 및 골교체 표지자의 변화를 살펴보았다. 그 결과 요추의 골밀 도는 teripatide 투여 1년 후 유의하게 증가하였다 (4.4%, P<0.01). Teriparatide 투여 후 요추의 골밀도 가 증가하는 것은 이전의 다른 연구에서도 관찰된 바가 있고 이것은 teriparatide 투여 전 골흡수 억제제 의 치료여부나 반응여부와 상관이 없었다7,14,18. 그리 고 EUROPOS 연구13나 Gallagher 등의 연구19에서는 teriparatide 투여 전 골흡수 억제제 치료를 받지 않았 던 군이 골흡수 억제제 치료를 받은 군에 비해 teri- paratide에 대한 반응이 더 좋았음을 보여주고 있는 데, 앞으로 한국인의 경우에서도 골흡수 억제제 치 료 과거력이 이들 연구에서와 같이 동일한 결과를 보이는지, 아니라면 어떤 차이가 있는지에 대한 연 구가 시행되어야 할 것이다.
본 연구에서 대퇴골 골밀도의 경우 teriparatide 치
료 1년 후 대퇴골 경부에서는 감소하였고(-9.7%, P<0.05), 대퇴골 전체는 의미 있는 변화가 없었다 (-1.9%, P=0.071). 그러나 EUROPOS 연구에서는 이 전에 골흡수 억제제로 치료를 받았던 군에서 teri- paratide 치료 6개월 째 대퇴골 골밀도가 감소하다가 (이전 골흡수 억제제 치료에 부적절한 반응을 보인 군에서는 의미 있게 감소함), 치료 1년 째 이전 골흡 수 억제제 치료에 부적절한 반응을 보인 군은 치료 전과 비슷한 수준으로 회복되고 적절한 반응을 보인 군에서는 증가하기 시작하여 18개월부터는 모든 군 에서 유의하게 증가하는 것을 볼 수 있었다13,14. 본 연구에서는 이전의 골흡수 억제제 치료에 대한 반응
여부를 구별하여 살펴보지 않았고 1년 후의 대퇴골 전체 골밀도 감소는 통계적으로 유의하지 않았으며 대퇴골 경부 골밀도는 대퇴골 전체에 비해 측정 오 차가 크기 때문에 본 연구의 대퇴골 골밀도 결과를 한국인에게 일반화시켜 적용하는 것은 무리가 있겠 다. 앞으로 이런 점을 보완한 장기간의 연구를 통해 본 연구에서의 teriparatide 치료에 대한 대퇴골 골밀 도 변화가 국외의 연구결과와 다른 것이 인종적 차 이에 의한 것인지, 아니면 연구 대상자가 적고 세분 화되지 못한 본 연구의 제한점에 의한 것이지 살펴 볼 필요가 있을 것이다.
이전에 골흡수 억제제로 치료를 받았던 환자에서 teriparatide 치료 시 대퇴골 골밀도가 치료 초기에 일 시적으로 감소하는 것에 대한 논의는 앞으로도 계속 되어야 할 문제이다. 골흡수 억제제로 치료를 받았 던 환자에서 teriparatide 치료 시 대퇴골 골밀도가 일 시적으로 감소하는 것을 처음 보고한 사람은 Ettin- ger와 그의 동료들이었다18. EUROPOS의 1년 연구에 서도 이전에 골흡수 억제제 치료를 받지 않은 군은 teriparatide 치료 6개월 후부터 대퇴골 골밀도의 유의 한 증가를 보인 반면, 이전에 골흡수 억제제 치료를 받았던 군은 6개월째 감소하다가 이 후 증가하는 경 향을 보이고 있었다13. 이전의 연구들에 의하면 teri- paratide에 의한 골밀도 변화는 피질골보다 해면골이 많은 골격계에서 더 많음을 알 수 있다9,18,20,21. 요추 는 해면골이 풍부한 뼈인 반면 대퇴골은 피질골이 풍부한 뼈이다. 따라서 피질골이 풍부한 대퇴골에서 teriparatide에 대한 반응이 늦게 나타났을 것이라고 생각해 볼 수 있을 것이다. 그리고 또 다른 연구들에 서 teriparatide가 피질골에서 신생의 골기질을 골막 에 침착시키고 골 내의 낡은 골기질을 흡수시킬 때, 이전에 골흡수 억제제 치료로 인해 골교체가 억제되 어있는 경우에는 고도의 미네랄화가 되어있는 골에 서의 골흡수를 먼저 일으키고 이후 미네랄화가 덜 되어있는 뼈에서 골형성을 유도한다는 것을 유추해 볼 수 있다22-25. 이러한 이유들로 인해 teriparatide 치 료 시 대퇴골 골밀도가 일시적으로 감소할 것이라는 것이 현재까지 임상에서 받아들여지고 있는 가설이 다.
골형성 표지자인 osteocalcin과 alkaline phosphatase,
골흡수 표지자인 CTX는 이전의 다른 연구6,7,18에서 와 마찬가지로 본 연구에서도 teriparatide 치료 1년 후에 의미 있는 증가를 보였다(P<0.00l for all). Ste- ven Boonen 등은 EUROPOS 연구에서14 이전에 치료 받았던 골흡수 억제제의 종류와 골흡수 억제제를 끊 고 teriparatide 치료를 시작하기까지의 기간에 따라 골형성 표지자의 수치가 다르게 나타났지만 이러한 차이가 골밀도 변화와 일치하지 않기 때문에 이러한 결과에 대한 임상적 의미는 아직 명확하지 않다고 말하고 있다. 따라서 앞으로 골형성 표지자의 임상 적 의의에 대한 연구는 계속되어야 할 것이다.
본 연구의 제한점은 첫째 연구 대상자의 수가 적 다는 것이다. 이는 Teriparatide가 국내에 소개된 지 몇 해 안되고 아직 국내에서는 비급여로 처방되는 고가의 약제이기 때문에 실제로 teriparatide 치료를 받는 사람이 적은데다가 1년 이상 지속적인 치료를 받는 경우도 많지 않기 때문이라고 할 수 있겠다. 두 번째로 본 연구는 공개적 연구였으며 대조군이 없었 다. 또한 후향적 연구로서 연구 대상자의 폐경기간, 칼슘과 비타민 D 복용 여부 등을 모든 대상자에서 다 알 수 없었다. 그리고 teriparatide 투여 전의 골흡 수 억제제 투여기간을 1년 이상으로 제한했지만 모 든 대상자가 그 기간이 동일하지 않았다는 점이다.
본 연구를 통해 한국의 골다공증이 있는 폐경 여성 에게 1년 동안 teriparatide를 투여했을 때 국외의 다 른 연구에서처럼 요추의 골밀도가 증가함을 알 수 있었다. 대퇴골 경부의 경우는 국외 연구와 달리 teriparatide 치료 1년이 되어도 골밀도의 감소가 지속 되었음을 알 수 있었다. 본 연구는 국내에서 teri- paratide의 골밀도 및 골교체 표지자에 미치는 영향 을 살펴 본 최초의 연구라는 점에서 의의가 있겠고, 앞으로 더 많은 대상자로 장기간의 체계적인 전향적 연구가 시행되어야 할 것이다.
참 고 문 헌
1. NIH Consensus Development Panel on Osteoporo- sis Prevention, Diagnosis and Therapy. Osteoporo- sis Prevention, Diagnosis, and Therapy. JAMA 2001;285:785-95.
2. Ethel S, Paul D, Elizabeth B, Kenneth G, Lois E, Thomas A, et al. Identification and fracture outcomes of undiagnosed low bone mineral density in postmenopausal women: results from the Natio- nal Osteoporosis Risk Assessment. JAMA 2001;
286:2815-26.
3. 김영일, 박재후, 이종수, 김진우, 양승오, 전대준 등. 울산지역에서 주폐경기(Perimenopause) 여성 의 골다공증 유병률과 연관인자. 대한내과학회 지 2002;62:11-24.
4. Epstein S. Update of current therapeutic options for the treatment of postmenopausal osteoporosis. Clin Ther 2006;28:151-73.
5. Cosman F. Anabolic therapy for osteoporosis:
parathyroid hormone. Curr Osteoporos Rep 2005;
3:143-9.
6. Ma YL, Zeng Q, Donley DW, Ste-Marie LG, Gallagher JC, Dalsky GP, et al. Teriparatide increases bone formation in modeling and remo- deling osteons and enhances IGF-II immunoreacti- vity in postmenopausal women with osteoporosis. J Bone Miner Res 2006;21:855-64.
7. McClung MR, San Martin J, Miller PD, Civitelli R, Bandeira F, Omizo M, et al. Opposite bone remodeling effects of teriparatide and alendronate in increasing bone mass. Arch Intern Med 2005;
165:1762-8.
8. Jiang Y, Zhao JJ, Mitlak BH, Jiang Y, Zhao JJ, Mitlak BH, et al. Recombinant human parathyroid hormone (1-34) [teriparatide] improves both cortical and cancellous bone structure. J Bone Miner Res 2003;18:1932-41.
9. Neer RM, Arnaud CD, Zanchetta JR, Prince R, Gaich GA, Reginster JY, et al. Effect of parathyroid hormone (1-34) on fractures and bone mineral density in postmenopausal women with osteoporosis. N Engl J Med 2001;344:1434-41.
10. Keaveny TM, Donley DW, Hoffmann PF, Mitlak BH, Glass EV, San Martin JA. The effects of teriparatide and alendronate on vertebral strength as
assessed by finite element modeling of QCTscans in women with osteoporosis. J Bone Miner Res 2007;22:149-57.
11. Hodsman AB, Bauer DC, Dempster DW, Dian L, Hanley DA, Harris ST, et al. Parathyroid hormone and teriparatide for the treatment of osteoporosis: a review of the evidence and suggested guidelines for its use. Endocr Rev 2005;26:688-703.
12. Girotra M, Rubin MR, Bilezikian JP. The use of parathyroid hormone in the treatment of osteo- porosis. Rev Endocr Metab Disord 2006;7:113-21.
13. Helmut M, Maurice A, Maria ES, Barbara OP, Gunnar S, Fernando M, et al. Bone density after teriparatide in patients with or without prior antiresorptive treatment: one-year results from the EUROFORS study. Curr Med Res Opin 2008;24:
3117-128.
14. Steven B, Fernando M, Barbara OP, Maria ES, Clare B, Emment VG, et al. Effects of previous antiresorptive therapy on the bone mineral density response to two years of teriparatide treatment in postmenopausal women with osteoporosis. J Clin Endocrinol Metab 2008;93:852-60.
15. Obermayer-Pietsch BM, Marin F, McCloskey EV, Hadji P, Farrerons J, Boonen S, et al. Effects of two years of daily teriparatide treatment on bone mineral density in postmenopausal women with severe osteoporosis with and without prior anti- resorptive treatment. J Bone Miner Res 2008;23;
1591-600.
16. World Health Organization. Assessment of fracture risk and its application to screening for postmeno- pausal osteoporosis:report of a WHO study group.
World Health Organ Tech Rep Ser 1994;843:1-129.
17. JoAnn EM, Shari SB. The Menopause Transition and Postmenopausal Hormone Therapy. In:
Anthony SF, Eugene B, Dennis LK, Stephen LH, Dan LL, J. Larry Jameson, et al. Harrison's prin- ciple of internal medicine. 17th ed. New York:
McGrae-Hill companies; 2008 p. 2334-9.
18. Ettinger B, San Martin J, Crans G, Pavo I. Diffe- rential effects of teriparatide on BMD after treat- ment with raloxifene or alendronate. J Bone Miner Res 2004;19:745-51.
19. Gallagher JC, Rosen CJ, Chen P, Misurski DA, Marcus R. Response rate of bone mineral density to teriparatide in postmenopausal women with osteo- porosis. Bone 2006;39:1268-75.
20. Black DM, Greenspan SL, Ensrud KE, Palermo L, McGowan JA, Lang TF, et al. The effects of parathyroid hormone and alendronate alone or in combination in postmenopausal osteoporosis. N Engl J Med 2003;349:1207-15.
21. Black DM, Bilezikian JP, Ensrud KE, Greenspan SL, Palermo L, Hue T, et al. One year of alendro- nate after one year of parathyroid hormone (1-84) for osteoporosis. N Engl J Med 2005;353:555-65.
22. Lindsay R, Zhou H, Cosman F, Nieves J, Dempster
DW, Hodsman AB. Effects of a once-month treat- ment with PTH (1-34) on bone formation on can- cellous, endocortical, and periosteal surfaces of the human ilium. J Bone Miner Res 2007;22:495-502.
23. Parfitt AM. Parathyroid hormone and periosteal bone expansion. J Bone Miner Res 2002;17:1741-3.
24. Sato M, Westmore M, Ma YL, Schmidt A, Zeng QQ, Glass EV, et al. Teriparatide [PTH (1-34)]
strengthens the proximal femur of ovariectomized nonhuman primates despite increasing porosity. J Bone Miner Res 2004;19:623-9.
25. Burr DB, Hirano T, Turner CH, Hotchkiss C, Brommage R, Hock JM. Intermittently administered human parathyroid hormone (1-34) treatment in- creases intracortical bone turnover and porosity without reducing bone strength in humerus of ova- riectomized cynomolgus monkeys. J Bone Miner Res 2001;16:157-65.
■ 국문초록 ■
목적: 재조합 부갑상선 호르몬인 teriparatide는 골형성을 유도하고 척추 및 비척추 골절을 감소시킨 다. 본 연구에서는 골다공증이 있는 한국 폐경 여성을 대상으로 1년의 teriparatide 치료 시 오는 골밀도 와 골교체 표지자 변화를 평가하였다.
방법: 골다공증이 있는 폐경 여성이 등록되었고, 이들은 1년 동안 매일 자가로 teriparatide 20μg을 피 하주사했다. 요추와 대퇴골 골밀도 및 골교체 표지자인 osteocalcin, C-telopeptide of collagen cross-links (CTX), alkaline phosphatase는 teriparatide 치료 전과 1년 후 측정되었다.
결과: 요추 골밀도는 teriparatide 치료 1년 후 유의하게 증가하였다(4.4%, P<0.01). 그러나 대퇴골 경 부의 골밀도는 치료 시작 전보다 감소하였다(-9.7%, P<0.05). 골교체 표지자인 osteocalcin (148.5%), CTX (67.6%), alkaline phosphatase (56.7%)는 1년 후 모두 유의하게 증가하였다(P<0.001 for all).
결론: 골다공증이 있는 한국 폐경 여성에서 1년의 teriparatide 치료는 요추 골밀도와 골교체 표지자를 유의하게 증가시켰다. 앞으로 많은 사람을 대상으로 한 장기간의 체계화된 전향적 연구가 시행되어야 할 것이다.
중심단어: 골다공증, Teriparatide, 골밀도, 골교체 표지자, 폐경 여성