2008;22:21-28 □ 종 설 □
21
책임저자:이석구, 서울시 강남구 일원동 50 삼성서울병원 외과, 135-710 Tel: 02-3410-3464, Fax: 02-3410-0040 E-mail: [email protected]
본 논문의 요지는 2008년 삼성서울병원 신장이식 1,000예 기념 심포지엄에서 발표되었음.
신장 이식 후의 Post-transplant Lymphoproliferative Disorder
1성균관대학교 의과대학 소아과학교실, 2서울대학교 의과대학 소아과학교실, 성균관대학교 의과대학 3내과학교실,
4외과학교실
백경훈1ㆍ강희경2ㆍ김원석3ㆍ유건희1ㆍ정두련3ㆍ이석구4
The Post-transplant Lymphoproliferative Disorder after Renal Transplantation
Kyung Hoon Paik, M.D.1, Hee Gyung Kang, M.D.2, Won Seog Kim, M.D.3, Keon Hee Yoo, M.D.1, Doo Ryeon Chung, M.D.3 and Suk-Koo Lee, M.D.4
Department of Pediatrics, 1Samsung Medical Center, Sungkyun- kwan University School of Medicine, 2Seoul National University Children’s Hospital, Departments of 3Medicine and 4Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
Post-transplant lymphoproliferative disorder (PTLD) is a B cell proliferative disorder that is associated with Eptstein-Bar (EBV). This is a heterogeneous group of conditions charac- terized by EBV-driven proliferation of B-lymphocytes in the face of impaired T-cell immune surveillance. While new treatment modalities are being tried with variable success, regular EBV surveillance and carefully monitored reduction of immunosuppression remain the mainstay of treatment.
This paper reviews the current knowledge of this increasingly common complications in renal transplant recipients. (J Korean Soc Transplant 2008;22:21-28)
Key Words: Post-transplant lymphoproliferative disorder, Epstein-Barr virus, Renal transplantation 중심 단어: 이식 후 림프증식성 질환, Epstein-Barr 바
이러스, 신장 이식
서 론
최근 고형 장기 이식의 증가와 강력한 면역 억제제의 사
용으로 인해 이식 후 림프증식성 질환(post-transplant lympho- proliferative disorder, PTLD)의 위험성에 대한 관심이 높아 지고 있다. PTLD는 여러 가지 다양한 종류의 림프증식성 질환을 통칭하나 보통 Epstein-Barr 바이러스(EBV)에 관련 된 이식 후 질환에 대해 사용된다. 기본적인 기전은 이식 후 면역억제에 의한 T-cell dysfunction이다.(1) EBV 특이 면 역 반응이 억제되어 체내에 있던 EBV가 재활성화되거나, 원발성 EBV 감염을 억제시키지 못하는 것이 주된 원인이 다.(1) 아직까지 본 질환의 병리기전과 임상 양상에 관해서 는 많은 연구가 필요한 상태이다.
본 론 1) 발생 빈도
신장 이식 후 1∼10%의 환자에서 발생한다.(2) 소아에서 는 1.2∼4.5%로 보고되고 있으며(3,4) 소아 이식환자에서 가장 흔한 종양성 질환이다.(5) 소아에서 성인보다 4배 정 도 많이 발생한다.(6) 위장관 이식 후 19%, 심장 이식 후 2∼
10%, 심장-폐 이식 후 5∼9%, 간 이식 후 2∼8%가 발생한 다.(2,6,7) 장기별로 발생 빈도가 다른 이유는 잘 모르지만, 기관 마다 림프 조직의 양이 다르고, 이식 후 면역 억제의 정도가 다른 것에 원인이 있을 것으로 생각되고 있다.(7)
2) 위험 인자
(1) EBV seronegative recipient status: 가장 중요한 위험 인자이다.(2,3,9-12) 소아에서 EBV-negative recipient 에서 25∼
50배 정도 PTLD 발생이 많다는 보고가 있다.(8) 이식 후 첫 1년간의 PTLD 발생의 위험도는 EBV negative recipient에서 positive recipient보다 20배 정도 높다.(14) 또한 EBV negative recipient에게 EBV positive donor의 신장을 이식했을 경우에 위험도는 더 증가한다.(14) 이식 받은 환자에서 이식 후에 원발성 EBV 질환이 발생했을 경우 증상이 더 심하고 이식 신의 손실이 있을 위험성이 크다는 보고도 있다.(9) (2) 면역억제제: PTLD는 면역 억제와 관련된 질환이다.
보다 강력한 면역억제제들이 개발됨에 따라 PTLD의 발생 빈도도 증가하고 있다.(3,6,7,10,11) 강력한 면역억제 상태에 서 PTLD는 때때로 치명적이 될 수 있다.(10,17) 면역 억제
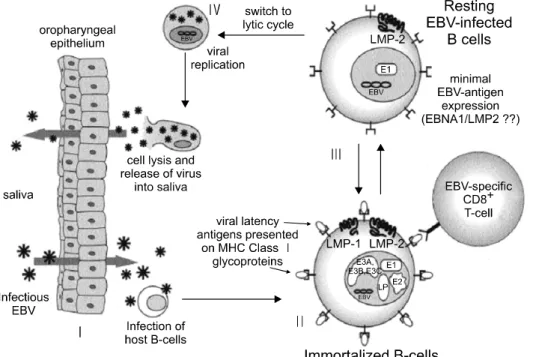
Fig. 1. Life cycle of EBV. (I) Infection of epithelium and entry into B cell compartment; (II) immor- talization of EBV-infec- ted B cells; (III) establi- shment of latency; (IV) entry into lytic cycle.(22) 에 의한 T-cell 기능의 감소로 인해 EBV에 의한 증식이 늘
어나게 된다.(12) 특히, OKT3 사용시 PTLD의 위험성이 증 가한다.(13) 이전의 연구에서 tacrolimus를 사용했을 경우에 cyclosporin보다 더 발생율이 높다는 보고가 있지만(18,19) 최근에 이들 약제에 대한 사용경험이 많아지고 치료 농도 를 철저히 조절해서 낮춤에 따라 차이가 없다는 보고도 있 다.(14) 또한, mycophenolate mofetil (MMF) 또는 tacrolimus+
MMF 병합 요법에서 발생이 더 증가하지는 않는다는 보고 도 있다.(15) 확실한 결론을 위해서는 보다 많은 기관의 전 향적인 연구가 필요한 상태이다.
(3) Simutaneous cytomegalovirus disease: 원발성 CMV 질 환 환자에서 이식 후 PTLD의 위험성이 4∼6배 정도 높 다.(2) CMV 질환이 EBV의 증식을 변화시키는 것이 원인으 로 생각된다.(16)
(4) 기타: 어린 나이에 이식할 경우, 남자, 백인, C형 간염 감염 등이 위험인자로 보고되고 있다.(3,14,17,18) 사이토카 인 유전자 다형성(Cytokine gene polymorphism)이 PTLD 와 관련이 있다는 연구도 있으며 interferon gamma 생산의 감소 가 간, 신장 이식에서 PTLD의 위험을 증가시킨다는 연구도 있다.(13)
3) 병태생리
EBV는 대부분의 사람들에서 감염을 일으키지만 건강한 사람에서는 병을 일으키지 않는다. 면역기능이 억제되어 있는 이식 환자에서는 EBV 증식과 EBV 특이 면역 반응 사 이에 불균형이 생겨서 EBV의 과증식이나 종양성 변화를 일으키는 경우가 생길 수 있다.
(1) 바이러스: EBV는 임파구성 또는 상피 세포 종양과
관련되어 있는 lymphotropic herpes virus 이다.(19) 대부분의 사람들이 EBV에 감염되어 있는데, 성인의 90% 이상에서 EBV 감염의 혈청학적 증거가 있다.(2) 처음 감염 시 바이러 스의 주요 envelope glycoprotein인 gp350이 B세포 표면의 CD21과 반응하여 세포 내로 들어가게 된다(Fig. 1).(2) 일단 숙주세포 내에 자리잡은 바이러스는 일생 동안 잠복해 있 게 된다. 적은 수의 B세포가 비증식성의 바이러스를 가지 고 있으면서 때때로 oropharyngeal epithelium에서 간헐적인 바이러스 증식이 일어나게 된다.(20) 이러한 잠복 상태에서 바이러스는 EBNA(Epstein-Barr nuclear antigen)와 LMP (latent membrane proteins)을 생산하여 B-cell에 의한 apoptosis로부 터 보호하게 한다(Fig. 1).(21) 건강한 사람에서는 cytotoxic T-cell(CD8+ T-cells)에 의해 EBV의 증식이 억제되어 있 다.(2)
(2) 병리기전: 면역억제 된 상태에서는 EBV specific cyto- toxic T-cell 기능의 저하로 바이러스가 증식하게 된다.(22) 이때 virus-carrying B-cell의 숫자가 증가하고 virus lytic cycle antigen의 항체가 증가하게 된다.(22) 결국 lytic repli- cation과 B세포의 형질 전환(transformation)이 일어난다. 면 역 억제 상태에서 EBV-transformed B-cell clone의 증식이 과 도하게 일어나게 되어(23,24) 과증식성 또는 종양성 PTLD 로 된다. 고형 장기 이식에서 비정상적 B세포는 보통 recipient origin이다.(8,29)
4) 분류
(1) WHO에서는 PTLD를 임상적, 조직학적 양상에 따라 early lesions, polymorphic PTLD, monomorphic PTLD로 나누 고 있다(Table 1).
Table 1. WHO classification of PTLD
Category Subtype
Early lesions Reactive plasmacytic hyperplasia Polymorphic PTLD Polyclonal
Monoclonal Monomorphic PTLD B-cell lymphomas
Diffuse large B-cell lymphoma Burkitt’s/Burkitt’s like lymphoma Plasma cell myeloma
T-cell lymphomas
Peripheral T-cell lymphoma Rare types(gamma/delta,
T/natural killer cell) Other types
Hodgkin’s disease-like Plasmacytoma-like
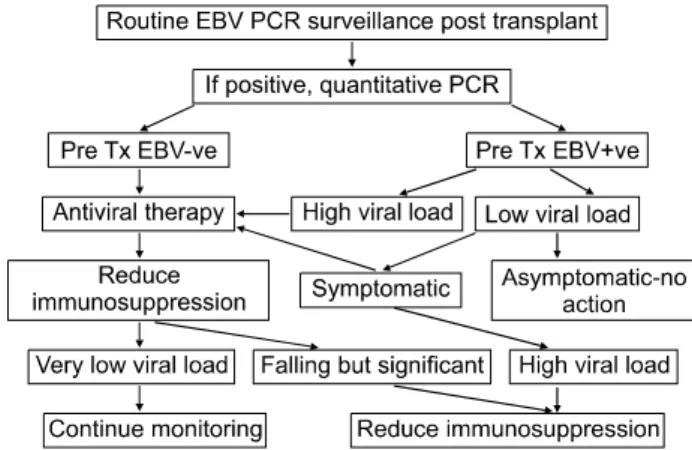
Fig. 2. Epstein-Barr virus (EBV) monitoring post transplant.(2)
Table 2. Clinical and pathologic spectrum of PTLD and its management(32)
Early disease (50%) Polymorphic (30%) Monoclonal (20%)
Clinical features Infectious mononucleosis-type Infectious mononucleosis-type illness Fever, weight loss, localizing
illness ±wt loss, localizing symptoms symptoms
Pathology Preserved architecture;atypical Intermediate High-grade lymphoma with confluent
cells infrequent transformed cells and marked atypia
Clonality Polyclonal Usually polyclonal Monoclonal
Treatment Reduce immunosuppression; Reduce immunosuppression; Reduce immunosuppression to acyclovir acyclovir; if poor response low-dose steroids only; combination
then treat as monoclonal PTLD treatment; surgery, chemotherapy, radiation therapy, immunotherapy, rituximab.
Prognosis Good Intermediate Poor
(2) EBV-negative PTLD: EBV-negative PTLD는 주로 late-onset PTLD에서 볼 수 있으며, 단순히 면역결핍된 환자 에서 우연히 생기는 lymphoma라고 할 수도 있다.(2) 또한, EBV와 연관되서 “hit and run” 가설이 제시되고 있는데, EBV가 pre-neoplastic cell injury를 유발하고, neoplastic cell division이 일어난 후에 여러 기전에 의해 제거된다는 가설 이다.(25)
5) 임상양상
이식 후 언제라도 다양한 위치에서 발병할 수 있다. 임파 선 비대가 있는 경우가 많으며 구토, 설사, 출혈 등이 있을 수 있다. 거부반응과의 감별이 중요하다.
초기 증상은 비특이적으로 발열, 쇠약감, 체중 감소 등이 있다.(12,30,31) 소아환자에서는 원발성 EBV 감염이 있는 경우 infectious mononucleosis가 가장 흔한 발병 양상으로(9)
발열, 편도와 아데노이드 비대, 경부 임파선 비대, 간비대 등이 흔한 증상이다(9,26). Infectious mononucleosis 와 과증 식성, 종양성 변화와 감별하기 위해서는 조직 검사가 필수 적이다.(7) 신장 이식 후 생기는 PTLD의 약 1/3에서 병변이 이식한 신장 자체에 생기는 것으로 보고 되고 있다.(27) 일반적으로 PTLD는 47%가 이식 후 6개월 이내에, 62%가 이식 후 1년 이내에, 90%가 이식 후 5년 이내에 생기는 것 으로 보고되고 있다.(28)
6) 진단
(1) Polymerase chain reaction: 혈장에서 EBV-DNA의 존 재는 높은 viral load를 의미하고 바이러스 증식이 지속되고 있음을 의미한다.(29,30) 거의 모든 연구에서 reactivation 질 환 보다 원발성 질환에서 viral load가 더 높음을 밝히고 있 다.(34,36-38) Viral load를 선별 검사로 이용하는 예는 Fig. 2 와 같다.(2)
(2) Radiology: 단순 방사선 촬영, 초음파 검사, CT, PET 등을 이용할 수 있다.
(3) Histology: PTLD의 최종 진단은 조직 검사이다. 조직에
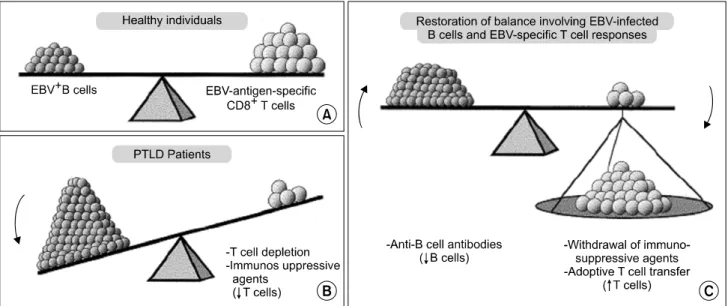
Fig. 3. Balance between EBV-infected B cells and EBV-specific T cells. (A) In healthy individuals; (B) in patients with PTLD; (C) patients in whom B cell numbers have been reduced or T cell responses have been augmented.(22)
서 EBV (EB-ER) in situ hybridization, immunostaining (LMP-1, EBNA-2) 등을 시행해서 진단할 수 있다.(31) 조직 검사에서 clonality (polyclonal or monoclonal)는 치료와 예후 결정에 중 요하다(Table 2). Monoclonal PTLD는 예후가 나쁘며 적극적 으로 치료해야 한다(Table 2).(32) PTLD는 급성 거부반응과 같이 있을 수 있는데, T-cell PTLD와 관련이 있다.(33) 이식 신 자체에 병변이 있을 경우 plasmacytoid infiltrates, immu- noblastic cells, nodular infiltrates, serpinginous necrosis, absence of neutrophils 등이 PTLD를 시사하는 소견이다.(31) (4) Markers of disease activity: 소변 monoclonal proteins (특히 IgM), 말초 혈액의 CD19+B세포, β2-microglobulin/
cystatin C ratio 등이 활성도를 평가하는데 이용될 수 있다는 연구들이 있다.(39,40)
7) 예방
EBV 감염이 없었던 수혜자, 강력한 면역 억제제 사용, 활동 형 CMV 질환 등이 PTLD의 주요 위험인자이다.(3,4,8,9,16, 34-36) 이들에서 EBV 감염 여부 감시, 항바이러스 투여 등 이 예방법으로 시도되어 왔다. 비감염자에 대한 EBV 백신 사용도 역시 효과가 있는 것으로 생각되고 있다.
(1) EBV surveillance: EBV에 의한 림프증식이 언제 종양 성으로 될 지 예측하기는 어렵다. 증상이 애매하거나 없는 경우도 많기 때문에 위험성이 높은 환자에서, 특히 이식 초 기에 정기적인 EBV 선별 검사가 필요하다.(9,26,37) 감염 초 기에 면역 억제를 줄임으로써 면역 체계를 회복 시켜서 EBV 증식을 억제할 수 있도록 하는 것이 중요하다.(9) (2) EBV vaccine: EBV 음성인 수혜자는 PTLD의 위험이 높아서 백신 접종의 대상이 될 수 있다.(2) EBV gp350 백신
투여 후 성공적으로 항체가 생성되고, 백신의 안정성이 보 고되고 있다.(2) 하지만 EBV 감염을 예방하기 위한 anti-gp 350 항체의 필요양은 아직 알려져 있지 않다. 적절한 백신 투여 양을 결정하기 위한 연구가 현재 진행 중에 있다.(2) (3) 항바이러스제: EBV-PTLD에 항바이러스제를 사용하 는 것에 대해서는 상반된 연구 결과들이 있다.(40,42) 현재 사용할 수 있는 약제는 aciclovir와 ganciclovir 등이 있다. 이 들 약제들은 EBV의 lytic-replicative cycle을 억제하지만, latent 또는 oncogenic virus에는 효과가 없다.(38-40) 이론적으로 이들 약 제에 의해 예방 효과를 기대하려면 이식 전부터 사용하여 일생 동안 사용해야 하지만 대부분의 기관에서는 가장 많은 면역억제를 하고 PTLD의 위험이 가장 높은 이식 초기(3∼6개월)에 예방 목적으로 사용하고 있다.
8) 치료
치료의 기본 원리는 면역 억제를 감소시키거나 T cell을 직 접 투여하여 환자의 면역성을 늘리거나, anti-B cell antibody를 투여하는 것이다(Fig. 3).(22) 조직 소견과 임상 양상에 따라 치료가 결정된다(Table 2).(2,32)
(1) 면역억제제 감량: 면역억제제 감량은 PTLD 치료에서 가장 먼저 고려된다. 아직 면역억제제 감량에 대한 표준 지 침은 나와 있지 않고 환자의 임상 상태와 종양 크기, clo- nality, 이식신의 기능에 따라 조절해야 한다. 보통 많이 쓰 이는 방법은 cyclosporine이나 tacrolimus 용량을 1/2 이하로 줄이고, azathioprine이나 MMF는 중지하면서 경구용 스테로 이드는 유지하는 방법이다.(13,41) 신장 이식 환자에서는 거 부 반응에 의해 생명이 위협받는 경우는 드물기 때문에 면 역억제제 용량을 적극적으로 감량시키는 것이 가능하다.
Fig. 4. Rituximab: three potential mechanisms of action include apoptosis, complement activation and antibody-dependent
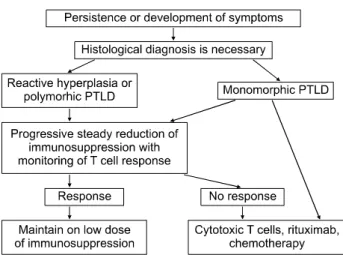
cell-mediated cytotoxicity.(41) Fig. 5. The management of PTLD using EBV PCR screening.(2) 보통 2∼4주가 지나야 반응이 있으며(42) 언제 다시 면역억
제제를 증가시켜야 하는지에 대해서는 아직 알려져 있지 않다. 면역억제제의 감량은 가장 중요하고 90% 이상의 증 례에서 사용되었다.(4) 면역억제제 감량 만으로 1/3-1/2의 환자에서 EBV에 의한 림프증식을 호전시켰다는 연구도 있 고, 완전히 치료했다는 연구도 있다.(17,26)
(2) Monitoring the host immune response to reduction of immunosuppression: 바이러스에 대한 반응에 특징적인 lymphocyte activation phenotype으로 PTLD의 관해를 유도할 수 있는 host immunity를 측정할 수 있다.(43) 이것을 통해 면역억제의 과도한 감량을 예방할 수 있다. EBV-transformed B-cell에 대한 CD8+ cytotoxic T-cell과 CD57+ cell, NK cell 이 host immunity에 주요한 역할을 한다.(2) 활동성 PTLD 시 기에 이들 세포 수는 감소되었다가 host immunity가 회복될 때 증가한다. CD 69+ T-cell 숫자는 활동성 PTLD시 증가한 다.(2) PTLD의 관해를 위해서는 지속적인 CD8+ T-cell의 증가가 필요하다.(44)
(3) Anti-CD 20 anitibodies: 면역억제제 감량에도 반응이 없는 환자에서 anti-CD20 monoclonal antibody(rituximab) 투 여가 좋은 성적을 보이고 있다.(45) Rituximab은 CD20을 표 현하는 B세포를 중화시켜서 EBV에 의한 림프증식의 lytic- replicatve phase를 억제한다(Fig. 4).(46) B-cell에 작용하는 주된 작용 기전은 apoptosis, complement activation, cell-mediated cytotoxicity 이다(Fig. 4).(41) Rituximab은 375 mg/m2의 용량 으로 일주일에 한번씩, 4회 정맥 주사하는 방법이 많이 쓰 이고 있다. 폐, 신장, 간, 심장 기능에 따른 용량 조절은 필요 하지 않다.(41) 처음 투여 시 발열, 오한, 두통 angioedema, 저혈압 등이 생길 수 있으므로 acetaminophen, 항히스타민 제 등으로 전처치 하는 것이 권장된다.(41) Rituximab은 정 상 B-cell에도 작용해서 B-cell depletion이 약 6개월간 지속 된다.(41) 하지만, rituximab 투여 후 2년간 관찰시 감염이 증가하지는 않는다는 연구가 있으며, 비교적 심각한 부작용이 없이 안전하게 사용되고 있다.(47) 마찬가지로, anti-CD21, anti-CD24 antibody의 사용도 시도되고 있고 각각 80%, 46%
의 관해율을 보고하고 있다.(47) 이들 치료의 부작용은 2차 감염, 종양용해증후군(tumor lysis syndrome), 면역글로불린 생성 장애 등이다.(48)
(4) Interferon alfa: 환자의 면역 시스템을 비특이적으로 강화시키는 효과가 있으나 CD8+ T-cell 활성화를 증가 시 킴으로 인해 거부반응을 유도할 위험이 있다.(2)
(5) Chemotherapy: 면역억제제 감량에도 효과가 없는 환 자에서 anthracycline-based chemotherapy (CHOP; cyclophs- phamide, adriamycin, viscristine, and prednisolone)가 좋은 효 과를 보였다는 연구가 있다.(49) 심한 PTLD(Burkitt lympho- ma-like disease 등) 에서는 chemotherapy가 일차 치료로 사용 되기도 한다.(41)
(6) 항바이러스제: ganciclovir 또는 acyclovir가 예방 및 치 료에 시도되어 왔다. 하지만, 항바이러스제가 단일 치료로 PTLD에 효과적이지는 않다. 이들 항바이러스제가 EBV genome을 가지고 있는 latent EBV-infected B-cell을 제거시 키지는 못한다.(41)
(7) Cytotoxic T-cells: 골수이식 후에 생기는 PTLD에서 공 여자의 EBV-specific cytotoxic T-lymphoctye를 투여해서 좋 은 효과를 보인 연구가 있다.(50) 고형장기 이식 후에 사용 하는 것에 대한 연구는 현재 진행 중에 있다.(51)
9) 예후
PTLD에서 나쁜 예후를 예측할 수 있는 인자는 monoclonal lesion, 다발성 병변, 후기 발생, 이식신 병변, 중 추신경 침범, 높은 LDH, 진단시 bad performance status 등이 다.(41)
결 론
신장 이식 후의 PTLD는 조직형에 따라 예후와 치료 방침 이 달라질 수 있다(Fig. 5). 이식 후 EBV PCR 검사를 정기적
으로 시행하면서 EBV 감염 상태를 감시하면서 적절한 시 기에 면역억제제의 용량을 조절하는 것이 치료 및 예방에 있어서 중요하다(Fig. 5).(2) 면역억제제 감량에도 효과가 없 을 경우 rituximab 이 비교적 안전하고 효과적인 치료법으로 최근에 많이 사용되고 있다(Fig. 5). 신장 이식 후의 PTLD의 치료 방침에 대해서는 앞으로 많은 환자를 대상으로 한 전 향적인 연구가 필요하다.
REFERENCES
1) Gottschalk S, Rooney CM, Heslop HE. Post-transplant lym- phoproliferative disorders. Annu Rev Med 2005;56:29-44.
2) Shroff R, Rees L. The post-transplant lymphoproliferative disorder-a literature review. Pediatr Nephrol 2004;19:369-77.
3) Dharnidharka VR, Sullivan EK, Stablein DM, Tejani AH, Harmon WE. Risk factors for posttransplant lymphoproli- ferative disorder (PTLD) in pediatric kidney transplantation: a report of the North American Pediatric Renal Transplant Cooperative Study (NAPRTCS). Transplantation 2001;71:
1065-8.
4) Funch DP, Brady J, Ko HH, Dreyer NA, Walker AM.
Methods and objectives of a large US multicenter case-control study of post-transplant lymphoproliferative disorder in renal transplant patients. Recent Results Cancer Res 2002;159:81-8.
5) Pinkerton CR, Hann I, Weston CL, Mapp T, Wotherspoon A, Hobson R, Kelly DA, Vergani D, Hadzic D, Rees L, Burke M, Alero Thomas J. Immunodeficiency-related lymphopro- liferative disorders: prospective data from the United Kingdom Children's Cancer Study Group Registry. Br J Haematol 2002;118:456-61.
6) Shapiro R, Nalesnik M, McCauley J, Fedorek S, Jordan ML, Scantlebury VP, Jain A, Vivas C, Ellis D, Lombardozzi-Lane S, Randhawa P, Johnston J, Hakala TR, Simmons RL, Fung JJ, Starzl TE. Posttransplant lymphoproliferative disorders in adult and pediatric renal transplant patients receiving tacrolimus-based immunosuppression. Transplantation 1999;68:1851-4.
7) Paya CV, Fung JJ, Nalesnik MA, Kieff E, Green M, Gores G, Habermann TM, Wiesner PH, Swinnen JL, Woodle ES, Bromberg JS. Epstein-Barr virus-induced posttransplant lym- phoproliferative disorders. ASTS/ASTP EBV-PTLD Task Force and The Mayo Clinic Organized International Consensus Development Meeting. Transplantation 1999;68:1517-25.
8) Boubenider S, Hiesse C, Goupy C, Kriaa F, Marchand S, Charpentier B. Incidence and consequences of post-transplan- tation lymphoproliferative disorders. J Nephrol 1997;10:136-45.
9) Shroff R, Trompeter R, Cubitt D, Thaker U, Rees L. Epstein- Barr virus monitoring in paediatric renal transplant recipients.
Pediatr Nephrol 2002;17:770-5.
10) Libertiny G, Watson CJ, Gray DW, Welsh KI, Morris PJ.
Rising incidence of post-transplant lymphoproliferative disease in kidney transplant recipients. Br J Surg 2001;88:1330-4.
11) Walker RC, Marshall WF, Strickler JG, Wiesner RH, Velosa JA, Habermann TM, McGregor CG, Paya CV. Pretran- splantation assessment of the risk of lymphoproliferative disorder. Clin Infect Dis 1995;20:1346-53.
12) Bakker NA, van Imhoff GW, Verschuuren EA, van Son WJ.
Presentation and early detection of post-transplant lympho- proliferative disorder after solid organ transplantation. Transpl Int 2007;20:207-18.
13) Tsao L, Hsi ED. The clinicopathologic spectrum of posttrans- plantation lymphoproliferative disorders. Arch Pathol Lab Med 2007;131:1209-18.
14) Shpilberg O, Wilson J, Whiteside TL, Herberman RB. Pre- transplant immunological profile and risk factor analysis of post-transplant lymphoproliferative disease development: the results of a nested matched case-control study. The University of Pittsburgh PTLD Study Group. Leuk Lymphoma 1999;
36:109-21.
15) Shapiro R, Scantlebury VP, Jordan ML, Vivas C, Ellis D, Lombardozzi-Lane S, Gilboa N, Gritsch HA, Irish W, McCauley J, Fung JJ, Hakala TR, Simmons RL, Starzl TE.
Pediatric renal transplantation under tacrolimus-based immu- nosuppression. Transplantation 1999;67:299-303.
16) Ho M, Jaffe R, Miller G, Breinig MK, Dummer JS, Makowka L, Atchison RW, Karrer F, Nalesnik MA, Starzl TE. The frequency of Epstein-Barr virus infection and associated lym- phoproliferative syndrome after transplantation and its mani- festations in children. Transplantation 1988;45:719-27.
17) Buda A, Caforio A, Calabrese F, Fagiuoli S, Pevere S, Livi U, Naccarato R, Burra P. Lymphoproliferative disorders in heart transplant recipients: role of hepatitis C virus (HCV) and Epstein-Barr virus (EBV) infection. Transpl Int 2000;13 Suppl 1:S402-5.
18) Manez R, Breinig MC, Linden P, Wilson J, Torre-Cisneros J, Kusne S, Dummer S, Ho M. Posttransplant lymphoproliferative disease in primary Epstein-Barr virus infection after liver transplantation: the role of cytomegalovirus disease. J Infect Dis 1997;176:1462-7.
19) Epstein MA, Achong BG, Barr YM. Virus Particles in Cultured Lymphoblasts from Burkitt's Lymphoma. Lancet 1964;1:702-3.
20) Sixbey JW, Nedrud JG, Raab-Traub N, Hanes RA, Pagano JS.
Epstein-Barr virus replication in oropharyngeal epithelial cells.
N Engl J Med 1984;310:1225-30.
21) Miyashita EM, Yang B, Lam KM, Crawford DH, Thorley- Lawson DA. A novel form of Epstein-Barr virus latency in normal B cells in vivo. Cell 1995;80:593-601.
22) Hsieh WS, Lemas MV, Ambinder RF. The biology of Epstein-Barr virus in post-transplant lymphoproliferative disease.
Transpl Infect Dis 1999;1:204-12.
23) Swinnen LJ, Costanzo-Nordin MR, Fisher SG, O'Sullivan EJ, Johnson MR, Heroux AL, Dizikes GJ, Pifarre R, Fisher RI.
Increased incidence of lymphoproliferative disorder after
immunosuppression with the monoclonal antibody OKT3 in cardiac-transplant recipients. N Engl J Med 1990;323:1723-8.
24) Tanner JE, Alfieri C. The Epstein-Barr virus and post-transplant lymphoproliferative disease: interplay of immunosuppression, EBV, and the immune system in disease pathogenesis. Transpl Infect Dis 2001;3:60-9.
25) Ambinder RF. Gammaherpesviruses and “Hit-and-Run” onco- genesis. Am J Pathol 2000;156:1-3.
26) Srivastava T, Zwick DL, Rothberg PG, Warady BA. Posttran- splant lymphoproliferative disorder in pediatric renal transplan- tation. Pediatr Nephrol 1999;13:748-54.
27) Cohen JI. Epstein-Barr virus lymphoproliferative disease asso- ciated with acquired immunodeficiency. Medicine (Baltimore) 1991;70:137-60.
28) Mihalov ML, Gattuso P, Abraham K, Holmes EW, Reddy V.
Incidence of post-transplant malignancy among 674 solid- organ-transplant recipients at a single center. Clin Transplant 1996;10:248-55.
29) Gartner BC, Fischinger J, Schafer H, Einsele H, Roemer K, Muller-Lantzsch N. Epstein-Barr viral load as a tool to diagnose and monitor post-transplant lymphoproliferative disease.
Recent Results Cancer Res 2002;159:49-54.
30) Haque T, Thomas JA, Parratt R, Hunt BJ, Yacoub MH, Crawford DH. A prospective study in heart and lung transplant recipients correlating persistent Epstein-Barr virus infection with clinical events. Transplantation 1997;64:1028-34.
31) Rowe M, Lear AL, Croom-Carter D, Davies AH, Rickinson AB. Three pathways of Epstein-Barr virus gene activation from EBNA1-positive latency in B lymphocytes. J Virol 1992;66:122-31.
32) Magee CC, Milford E. Clinical aspect of renal transplantation.
In: Brenner BM editor. The Kidney. 7th ed. Philadelphia, Saunders 2004. p.2838.
33) Lippman SM, Grogan TM, Carry P, Ogden DA, Miller TP.
Post-transplantation T cell lymphoblastic lymphoma. Am J Med 1987;82:814-6.
34) Basgoz N, Preiksaitis JK. Post-transplant lymphoproliferative disorder. Infect Dis Clin North Am 1995;9:901-23.
35) Herzig KA, Juffs HG, Norris D, Brown AM, Gill D, Hawley CM, Cobcroft R, Petrie JB, Marlton P, Thomson D, Campbell SB, Nicol DL, Johnson DW. A single-centre experience of post-renal transplant lymphoproliferative disorder. Transpl Int 2003;16:529-36.
36) Sokal EM, Antunes H, Beguin C, Bodeus M, Wallemacq P, de Ville de Goyet J, Reding R, Janssen M, Buts JP, Otte JB.
Early signs and risk factors for the increased incidence of Epstein-Barr virus-related posttransplant lymphoproliferative diseases in pediatric liver transplant recipients treated with tacrolimus. Transplantation 1997;64:1438-42.
37) Newell KA, Alonso EM, Whitington PF, Bruce DS, Millis JM, Piper JB, Woodle ES, Kelly SM, Koeppen H, Hart J, Rubin CM, Thistlethwaite JR Jr. Posttransplant lymphoproliferative
disease in pediatric liver transplantation. Interplay between primary Epstein-Barr virus infection and immunosuppression.
Transplantation 1996;62:370-5.
38) Andersson J, Skoldenberg B, Ernberg I, Britton S, Henle W, Andersson U. Acyclovir treatment in primary Epstein-Barr virus infection. A double-blind placebo-controlled study. Scand J Infect Dis Suppl 1985;47:107-15.
39) Darenkov IA, Marcarelli MA, Basadonna GP, Friedman AL, Lorber KM, Howe JG, Crouch J, Bia MJ, Kliger AS, Lorber MI. Reduced incidence of Epstein-Barr virus-associated posttransplant lymphoproliferative disorder using preemptive antiviral therapy. Transplantation 1997;64:848-52.
40) Yao QY, Ogan P, Rowe M, Wood M, Rickinson AB.
Epstein-Barr virus-infected B cells persist in the circulation of acyclovir-treated virus carriers. Int J Cancer 1989;43:67-71.
41) Svoboda J, Kotloff R, Tsai DE. Management of patients with post-transplant lymphoproliferative disorder: the role of rituximab. Transpl Int 2006;19:259-69.
42) Tsai DE, Hardy CL, Tomaszewski JE, Kotloff RM, Oltoff KM, Somer BG, Schuster SJ, Porter DL, Montone KT, Stadtmauer EA. Reduction in immunosuppression as initial therapy for posttransplant lymphoproliferative disorder: analysis of prognostic variables and long-term follow-up of 42 adult patients. Transplantation 2001;71:1076-88.
43) Haque T, Amlot PL, Helling N, Thomas JA, Sweny P, Rolles K, Burroughs AK, Prentice HG, Crawford DH. Reconstitution of EBV-specific T cell immunity in solid organ transplant recipients. J Immunol 1998;160:6204-9.
44) Porcu P, Eisenbeis CF, Pelletier RP, Davies EA, Baiocchi RA, Roychowdhury S, Vourganti S, Nuovo GJ, Marsh WL, Ferketich AK, Henry ML, Ferguson RM, Caligiuri MA.
Successful treatment of posttransplantation lymphoproliferative disorder (PTLD) following renal allografting is associated with sustained CD8(+) T-cell restoration. Blood 2002;100:2341-8.
45) Benkerrou M, Jais JP, Leblond V, Durandy A, Sutton L, Bordigoni P, Garnier JL, Le Bidois J, Le Deist F, Blanche S, Fischer A. Anti-B-cell monoclonal antibody treatment of severe posttransplant B-lymphoproliferative disorder: prognostic factors and long-term outcome. Blood 1998;92:3137-47.
46) Benkerrou M, Durandy A, Fischer A. Therapy for transplant- related lymphoproliferative diseases. Hematol Oncol Clin North Am 1993;7:467-75.
47) Hainsworth JD, Litchy S, Shaffer DW, Lackey VL, Grimaldi M, Greco FA. Maximizing therapeutic benefit of rituximab:
maintenance therapy versus re-treatment at progression in patients with indolent non-Hodgkin's lymphoma--a randomized phase II trial of the Minnie Pearl Cancer Research Network.
J Clin Oncol 2005;23:1088-95.
48) Cook RC, Connors JM, Gascoyne RD, Fradet G, Levy RD.
Treatment of post-transplant lymphoproliferative disease with rituximab monoclonal antibody after lung transplantation.
Lancet 1999;354:1698-9.
49) Swinnen LJ, Mullen GM, Carr TJ, Costanzo MR, Fisher RI.
Aggressive treatment for postcardiac transplant lymphoproli- feration. Blood 1995;86:3333-40.
50) Papadopoulos EB, Ladanyi M, Emanuel D, Mackinnon S, Boulad F, Carabasi MH, Castro-Malaspina H, Childs BH, Gillio AP, Small TN, Young JW, Kernan NA, O'Reilly RJ.
Infusions of donor leukocytes to treat Epstein-Barr virus-
associated lymphoproliferative disorders after allogeneic bone marrow transplantation. N Engl J Med 1994;330:1185-91.
51) Haque T, Wilkie GM, Taylor C, Amlot PL, Murad P, Iley A, Dombagoda D, Britton KM, Swerdlow AJ, Crawford DH.
Treatment of Epstein-Barr-virus-positive post-transplantation lymphoproliferative disease with partly HLA-matched allogeneic cytotoxic T cells. Lancet 2002;360:436-42.