262
책임저자: 박진영, 대구광역시 중구 삼덕 2가 50번지
700-721, 경북대학교병원 외과 Tel: 053-420-5612, Fax: 053-421-0510 E-mail: [email protected]
접수일:2008년 5월 1일, 게재승인일:2008년 6월 23일 본 논문의 요지는 2006년도 11월 서울에서 개최된 제58차 대한 외과학회 추계학술대회에서 구연되었음.
소아의 장중복증
경북대학교 의과대학 외과학교실
박수연ㆍ박진영
Intestinal Duplication in Childhood
Soo Yeun Park, M.D., Jin Young Park, M.D.
Department of Surgery, School of Medicine, Kyungpook National University, Daegu, Korea
Purpose: Intestinal duplication is a rare congenital anomaly that may be found anywhere from the mouth to the anus. The clinical presentation varies depending on the anatomic location or the size of the duplication, and the presence of the ectopic gastric tissue. The aim of this study was to analyze the clinical characteristics, the diagnostic and therapeutic methods, the location, the anatomic type and the associated anomalies of intestinal duplication.
Methods: We reviewed the medical record of eighteen patients with duplication of the alimentary tract and these patients had been treated at Kyungpook National University Hospital from July 1995 through October 2007.
Results: There were 9 boys and 9 girls. Their ages ranged from 3 days to 15 years. The most common symptom was abdominal pain. The duplicated segment acted as a leading point of intussusception in 3 cases. Two patients had melena. The duplications were cystic in fifteen cases and three others were tubular. In twelve cases, the lesions were located in the ileum; two other cases were located in the anal canal, one other was located in the in the transverse colon, another was located in the transverse and descending colon, one was located in the in the duodenum and one was located in the jejunum. Ultrasonography, computed tomography and barium enema were helpful as diagnostic tools. Three cases were diagnosed by prenatal ultrasonography. Associated anomalies were documented in four cases. All the patients underwent surgery. A duplicated lesion was lined with ectopic gastric mucosa in only one case. One patient still suffers from short bowel syndrome as a result of volvulus.
Conclusion: The early operative treatment of intestinal duplication is safe and effective to prevent complications.
In patients with intussusception, duplication should be considered as one of the causes of the leading point of intussusception. (J Korean Surg Soc 2008;75:262-267)
Key Words: Intestinal duplication, Childhood 중심 단어: 장중복증, 소아
서 론
소화관에 발생하는 장중복증은 드문 선천성 기형으로 혀 의 기저부에서부터 항문에 이르기까지 소화관의 어느 부위 에서나 발생할 수 있으나 주로 소장에 발생한다.(1-3) 대부 분 유아기에 증상이 나타나며 증상이 없는 경우도 있지만 병변의 위치와 크기, 이소성 위 점막의 유무에 따라 구토, 출혈, 복통, 복부 종괴 및 장 폐색 등 다양한 증상이 발생한
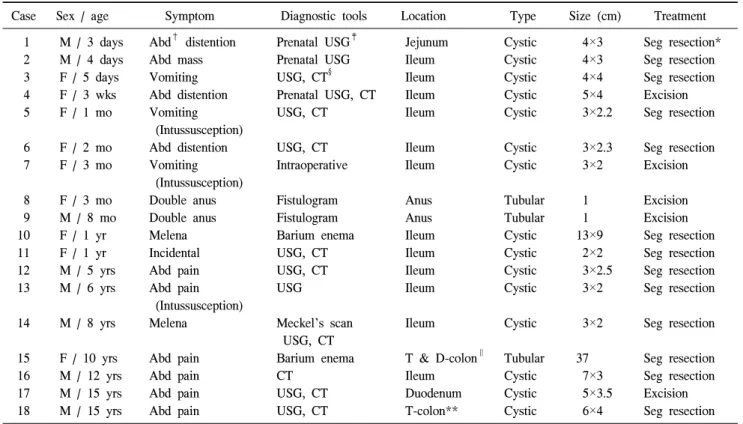
Table 1. Case summary
Case Sex / age Symptom Diagnostic tools Location Type Size (cm) Treatment
1 M / 3 days Abd† distention Prenatal USG‡ Jejunum Cystic 4×3 Seg resection*
2 M / 4 days Abd mass Prenatal USG Ileum Cystic 4×3 Seg resection
3 F / 5 days Vomiting USG, CT§ Ileum Cystic 4×4 Seg resection
4 F / 3 wks Abd distention Prenatal USG, CT Ileum Cystic 5×4 Excision
5 F / 1 mo Vomiting USG, CT Ileum Cystic 3×2.2 Seg resection
(Intussusception)
6 F / 2 mo Abd distention USG, CT Ileum Cystic 3×2.3 Seg resection
7 F / 3 mo Vomiting Intraoperative Ileum Cystic 3×2 Excision
(Intussusception)
8 F / 3 mo Double anus Fistulogram Anus Tubular 1 Excision
9 M / 8 mo Double anus Fistulogram Anus Tubular 1 Excision
10 F / 1 yr Melena Barium enema Ileum Cystic 13×9 Seg resection
11 F / 1 yr Incidental USG, CT Ileum Cystic 2×2 Seg resection
12 M / 5 yrs Abd pain USG, CT Ileum Cystic 3×2.5 Seg resection
13 M / 6 yrs Abd pain USG Ileum Cystic 3×2 Seg resection
(Intussusception)
14 M / 8 yrs Melena Meckel's scan Ileum Cystic 3×2 Seg resection
USG, CT
15 F / 10 yrs Abd pain Barium enema T & D-colon∥ Tubular 37 Seg resection
16 M / 12 yrs Abd pain CT Ileum Cystic 7×3 Seg resection
17 M / 15 yrs Abd pain USG, CT Duodenum Cystic 5×3.5 Excision
18 M / 15 yrs Abd pain USG, CT T-colon** Cystic 6×4 Seg resection
*Seg resection = segmental resection; †Abd = abdominal; ‡USG = ultrasonography; §CT = computed tomography; ∥D-colon = descending colon; **T-colon = transverse colon.
다. 성인에서 발견된 장중복증의 경우에는 드물지만 악성 변성이 보고되고 있어 진단 즉시 수술적 치료가 필요하 다.(4-6) 저자들은 소아에 발생한 장중복증의 임상양상, 진 단 및 치료 방법, 동반기형에 대해서 알아보고자 후향적 임 상고찰을 시행하였다.
방 법
1995년 7월부터 2007년 10월까지 경북대학교병원 소아외 과에 입원하여 장중복증으로 수술을 받은 18예의 환아의 의무기록을 바탕으로 성별, 수술 당시의 연령, 임상 양상, 진단 방법, 병변의 위치 및 크기, 해부학적 유형, 치료, 이소 성 조직의 유무, 동반기형에 관하여 조사 분석하였다.
결 과
1) 성별 및 수술 당시의 연령
성별은 남아에서 9예, 여아에서 9예가 발생하여 남녀의 성별 비는 동일하였다. 수술 당시의 연령은 생후 3일에서부
터 15세까지 다양하였으며, 1개월 미만이 4예, 1개월에서 1 세 미만의 영아기가 5예, 1세에서 5세까지가 2예, 5세 이상 이 7예였다(Table 1).
2) 임상양상
임상소견은 복통을 동반한 경우가 6예로 가장 많았으며, 구토가 3예, 복부팽만이 3예, 혈변이 2예, 외관상 항문의 개 구가 2개여서 진단된 경우가 2예, 복부 종괴 1예, 무증상이 1예 있었다. 3예에서는 장중첩증의 유도점으로 작용하였다.
3) 진단 방법
대부분에서 복부 초음파 검사와 전산화 단층촬영으로 진 단이 가능했었다(Fig. 1). 장중첩증을 유발했던 3예 중 1예 는 공기압 정복술을 시행한 후 재발하여 수술하는 도중에 발견이 되었으며, 나머지 2예는 공기압 정복술을 시행한 후 에 추적 복부 초음파 검사를 시행하는 도중에 발견되었다.
횡행결장에서부터 하행결장까지에 걸쳐서 발생한 관상형 장중복증(증례 15)과 회장에 발생한 구상형 장중복증 환아 중 1예(증례 10)에서는 대장 조영술에 의해 진단됐다(Fig.
Fig. 2. Barium study shows the ac- cumulation of contrast with- in the lesion. Operative find- ing shows a 13×9 cm sized round cystic lesion in the mesenteric side of the termi- nal ileum (Case 10).
Fig. 1. Abdominal ultrasonography and computed tomography show a round cystic mass in the left lower quadrant of the abdomen (Case 1).
Fig. 3. Duplication of transverse and descending colon. Operative finding shows a duplicated colon running parallel to the normal colon from transverse colon to descending colon (Case 15).
2). 임신 중 산전 초음파 검사상에서 복강 내 낭성종괴가 발견된 경우가 3예(증례 1, 2, 4) 있었으며, 처녀막 막힘증으 로 복부 초음파 검사를 시행하다가 우연히 발견된 경우(증 례 11)가 있었다. 혈변을 주소로 내원했던 2예에서는 맥켈 스캔을 시행하였으나 한 예에서만 양성으로 진단되었으며 (증례 14), 나머지 한 예는 맥켈 스캔에서 음성으로 나와 대 장 조영술을 추가로 시행하여 진단이 되었다(증례 10).
4) 수술 소견 및 방법
해부학적 유형은 구상형이 15예, 관상형이 3예였다. 병변 의 위치는 회장이 12예로 가장 많았고, 항문이 2예, 그리고 십이지장, 공장, 횡행결장 및 횡행결장에서부터 하행결장까 지에 걸쳐서 발생된 경우가 각각 1예씩이었다. 병변의 크기 는 구상형의 경우에 2×2 cm에서부터 13×9 cm까지 였으며, 횡행결장에서부터 하행결장까지에 걸쳐서 발생한 관상형 의 경우에는 길이가 37 cm였다(Fig. 3). 15예의 구상형 장중
복증 중 2예에서 인접한 정상 장관과 서로 교통되어 있었으 며, 3예의 관상형 장중복증 중 횡행결장에서부터 하행결장 까지에 걸쳐서 생긴 경우에서 근위부가 정상 장관과 서로 교통되어 있었으나 원위부는 맹단으로 막혀있어서 심하게 팽창되어 있었다. 수술 방법은 회장에 발생한 구상형 장중 복증 12예 중 2예에서 병변의 절제술을 시행하였으며, 10예 에서는 주위의 정상 장관을 포함한 절제술을 시행하였다.
항문에 발생된 2예와 십이지장 제2부위에 발생한 1예에서 절제술을 시행하였으며 횡행결장에서부터 하행결장까지에 걸쳐서 발생한 관상형 장중복증의 경우에는 GIA 봉합기를 이용하여 중격 절개술을 시도하였으나 점막에 궤양이 동반 되어 있어서 절제술을 시행하였다. 공장에 발생한 1예에서 는 수술 당시 장 염전에 의한 장 괴사로 소장의 대부분을 절제해 수술 후 단장 증후군이 발생하였다.
5) 이소성 조직 및 동반 기형
18예 중 혈변을 주소로 내원하여 맥켈 스캔으로 진단되 었던 회장의 구상형 장중복증 1예에서 술 후 조직 검사에서 이소성 위 점막조직이 발견되었다. 동반된 선천성 기형은 4예에서 처녀막 막힘증, 후두 연화증, 장 염전 및 Fallot 4징 이 각각 동반되었다.
고 찰
장 중복증은 드문 선천성 기형으로 1733년 Calder가 처음 으로 보고하였으며,(1) 국내에서는 Kim 등(7)이 처음으로 소아에서 발생한 장중복증 2예를 보고한 이후로 40예 정도 가 보고되어 있다.(1) 과거에는 enterogenous cyst, ileum du- plex, giant diverticula, unusual Meckel's diverticulum으로 혼 동되어 불리어지다가 Gross 등(8)이 duplication이라는 용어 를 제안하였다. 장중복증은 첫째, 잘 발달된 평활근에 의해 서 덮여 있어야 하고, 둘째, 위장관의 점막이 있어야 하며, 셋째, 정상적인 위장관에 인접해 있어야 한다.(9)
장중복증의 원인은 아직까지 정확하게 알려져 있지 않은 실정이나 여러 가지 가설이 제기되고 있다. Fetal gut diver- ticula가 잔존해서 장중복증이 생긴다는 diverticular theo- ry,(10) solid stage의 primitive gut에서 발생되는 recanalization 의 결함으로 장중복증이 발생한다는 aberrant luminal recan- alization theory,(11) partial twining,(12) split notochord theo- ry,(13) 태아의 발생과정 중에 초래된 혈류장애 및 저산소증 (2,14) 등이 있다.
성별은 Kim과 Jung(1)은 남아에서 약간 더 호발한다고 보 고하였고, Iyer와 Mahour(15)는 여아에서 호발한다고 보고 하였으나 저자들의 경우는 남아 9예, 여아 9예로 남녀의 성 별 비는 동일하였다.
증상의 발현 시기는 신생아에서부터 5세 이전의 유아기 에 이르기까지 다양하며 증상이 없는 경우에는 성인에서도 발견된다. 주로 1세 이전에 증상이 나타난다고 보고되고 있 으나(1,15,16) 본 연구에서는 1세 이전에 증상이 생긴 경우 는 50%이며, 39%가 5세 이후의 학령기에 증상이 나타났다.
임상양상은 장중복증의 형태학적 유형과 위치, 크기, 이 소성 위 점막의 유무에 따라서 다양하다. 증상이 없이 복부 촉진상에서 유동성의 복부 종괴가 만져지는 경우도 있으 며, 분비물의 축적으로 병변이 팽창되어 동통이 유발되기 도 하고, 인접한 장관을 압박해서 장 폐색을 일으킬 수도 있다.(15) 저자들의 경우 가장 흔한 증상은 복통으로 6예 (33%)에서 발생하였으며, 이 중 3예는 장중복증에 의해 초 래된 장중첩증에 의한 복통이었다. 향후 장중첩증으로 공 기압 정복술을 시행한 경우에는 복부 초음파 검사를 시행 하여 장중첩증의 원인의 하나로서 동반된 장중복증의 유무 를 확인해야 하겠다.
진단은 저자들의 경우처럼 산전 초음파 검사로 진단이 되는 경우도 있으나, 수술 전에 정확하게 진단하기는 어렵 고 수술 중에 우연히 발견되는 경우도 흔하다. 대개 복부 초음파 검사와 전산화 단층 촬영으로 진단할 수 있다. Royle 와 Doig(17)는 병변 내의 이소성 위 점막으로 인해 인접한 정상적인 장점막에 궤양이 초래되어 출혈이나 천공이 발생 하였다고 보고하였으며, Ildstad 등(18)은 30%에서, Stringer 등(19)은 29%에서 맥켈 스캔상 이소성 위 점막 조직이 발견 되어 맥켈 스캔이 진단에 도움이 된다고 하였으나, 위 음성 결과가 발생할 수도 있다고 보고되었다.(19) 저자들의 경우 혈변을 주소로 내원한 1예(5%)에서만 맥켈 스캔으로 진단 이 되었으며 수술 후 조직검사에서 이소성 위 점막이 발견 된 경우는 드물었다. 대장에 발생한 장중복증의 경우는 주 로 교통성 관상형 장중복증의 형태가 많아서 대장 조영술 이 유용하다.(20)
형태학적 유형은 구상형과 관상형으로 나누어지는데, 구 상형의 빈도가 훨씬 높으며(2) 저자들의 경우에도 15예 (83%)에서 구상형이었다. 구상형의 경우에는 인접한 정상 장관과의 교통이 없이 완전히 분리된 경우가 많으며, 관상 형의 경우에는 병변의 근위부, 원위부 혹은 양측이 정상 장 관과 교통이 있는 경우가 많으며, 단지 병변의 근위부와 교
통이 있는 경우에는 중복된 장이 분비물로 심하게 팽창하 여 장 폐색 심지어는 천공이 발생할 수도 있다.(15) 병변의 부위별 빈도는 회장에서 가장 많이 발생하며, 다 음으로 식도, 공장, 위 등의 순으로 발생되는데,(19) 저자들 의 경우에도 회장에서 발생된 경우가 12예(67%)로 가장 많 았다. 십이지장에 장중복증이 발생하는 경우는 매우 드물 며, 십이지장에 발생하는 장중복증은 주로 십이지장의 제 1 및 2 분절에 발생하여 십이지장 폐색, 췌장염 및 담도 폐 색을 야기하며 해부학적 위치 때문에 치료에 대해서 의견 이 분분하다.(21-23) 완전히 절제해 내는 것이 좋지만 불가 능한 경우에는 인접한 정상 십이지장이나 공장의 Roux-en Y loop 내로 내배액법을 이용한 조대술(marsupialization)을 시행할 수도 있다.(24) 이 경우에 담도계의 손상여부를 알 아보기 위해서 담도조영술이 반드시 필요하다. 저자들의 경우에는 복통을 주소로 내원한 15세 남아가 복부 전산화 단층 촬영에서 십이지장 장중복증이 의심되어 개복술을 시 행하였다. 십이지장 제2분절의 항장간막 부위에 위치한 5×3.5 cm의 구상형 장중복증이 발견되었으나, 인접한 정상 십이지장과의 연결이 없어서 쉽게 절제해 낼 수 있었다.
감별 진단해야 할 병변은 장간막 혹은 대망 낭종, 낭성 임파선종이 있으며, 이 경우에는 조직학적으로 내강이 점 막보다는 상피세포로 덮여 있다.(15)
장중복증은 합병증 및 악성 변성을 예방하기 위해서 진 단 즉시 조기에 수술적 절제가 필요하다.(19) 수술의 범위 는 환아의 증상을 없애고 재발을 방지하는 선에서 근치적 으로 절제를 시행해야 하며, 정상 장관의 광범위한 절제를 피하기 위해 공유된 혈관을 보존해야 한다.(25) 인접한 정 상 장관과 분리가 되어 있는 장중복증의 경우에는 쉽게 절 제해 낼 수도 있지만, 인접한 정상 장관과 혈류를 공유하는 경우에는 병변 자체만 단독으로 절제해 내기가 힘들어 인 접한 정상 장관과 함께 병변을 절제해야 한다. 저자들의 경 우에도 13예(72%)에서 인접한 정상 장관을 포함하여 병변 을 절재해 냈다. 길이가 긴 관상형 중복증이나 크기가 큰 구상형 중복증의 경우는 광범위한 절제가 단장 증후군을 야기할 수 있어 절제보다는 점막 발거술을 이용하기도 한 다.(18,26) 대장에 생긴 긴 관상형 장중복증의 경우에 병변 의 원위부에 있는 common wall을 일부 절제해 정상적인 장 과 연결해 주는 내배액법을 사용하여 치료하기도 한다. 최 근에는 복강경을 이용하여 장중복증을 절제한 경우도 보고 되었다.(27)
동반기형은 Stringer 등(19)은 장중복증 환아의 48%, Galvez
등(28)은 54%로 흔한 것으로 보고가 되었으나, Kim 등(2)은 외국과 비교해서 국내문헌에서 동반된 기형의 증례가 적은 것으로 보고하였으며 동반기형에 대한 철저한 검사가 필요 하다고 주장하였다. 저자들의 경우에도 단지 4예(22%)에서 각각 처녀막 막힘증, 후두 연화증, 장 염전 및 Fallot 4징이 동반되었다.
결 론
장중복증은 5세 이상의 연령에서 가장 많이 진단이 되었 으며, 남녀의 성별 비는 동일하였다. 위치는 회장에 가장 호 발하였으며, 형태학적 유형은 대부분이 구상형이었다. 증상 은 복통이 가장 많았으며, 장중첩증의 유도점으로 작용한 경우도 3예가 있어서 장중첩증 환아에서 공기압 정복술 후 에 복부 초음파 검사를 시행해야 하겠으며, 복통을 호소하 는 환아에서 장중복증을 감별진단 해야 하겠다. 수술 후 이 소성 위 점막조직이 발견된 경우는 1예로 드물며, 인접한 정상 장관과 혈관을 공유하고 있어서 병변의 단순절제는 어렵고 13예(72%)에서 인접한 정상 장관을 포함해서 절제 를 시행하였다. 단지 4예에서 동반기형이 발견되었으며 동 반기형에 대한 철저한 검사가 필요하다고 생각한다.
REFERENCES
1) Kim TW, Jung PM. A clinical study of intestinal duplication.
J Kor Assoc Pediatr Surg 2004;10:9-16.
2) Kim DY, Kim SC, Kim IK. Gastrointestinal duplications in childhood. J Kor Assoc Pediatr Surg 2001;7:26-30.
3) Lee SH, Kim KH, Jung SE, Lee SC, Park KW, Kim WK.
Clinical characteristics and management of congenital in- testinal duplication. J Korean Surg Soc 2001;61:530-6.
4) Orr MM, Edwards AJ. Neoplastic change in duplications of the alimentary tract. Br J Surg 1975;62:269-74.
5) Hickey WF, Corson JM. Squamous cell carcinoma arising in a duplication of the colon: case report and literature review of squamous cell carcinoma of the colon and of malignancy complicating colonic duplication. Cancer 1981;47:602-9.
6) Kim HS, Hong SH, Park HS, Lee ES, Kang IW. Adenocarci- noma arising in an ileal duplication cyst with peritoneal seed- ing: a case report. J Korean Radiol Soc 2001;44:599-602.
7) Kim HK, Woo ZH, Sohn JH. A report of 2 cases of duplica- tion of the alimentary tract. J Korean Surg Soc 1971;13:456-9.
8) Gross RE, Holcomb GW Jr, Farber S. Duplications of the ali- mentary tract. Pediatrics 1952;9:448-68.
9) Yamauchi Y, Hoshino S, Yamashita Y, Funamoto S, Ishida
K, Shirakusa T. Successful resection of an infected duodenal duplication cyst after percutaneous cyst drainage: report of a case. Surg Today 2005;35:586-9.
10) Lewis FT, Thyng FW. The regular occurrence of intestinal di- verticula in embryos of the pig, rabbit and man. Am J Anat 1908;7:505-19.
11) Bremer JL. Diverticula and duplications of the intestinal tract.
Arch Pathol 1944;38:132-40.
12) Wrenn EL Jr, Hollabaugh RS. Alimentary tract duplications. In:
Ashcraft KW, editor. Pediatric Surgery. 3rd ed. Philadelphia:
W.B. Saunders; 2000. p.527-39.
13) Bentley JF, Smith JR. Developmental posterior enteric rem- nants and spinal malformations: the split notochord syndrome.
Arch Dis Child 1960;35:76-86.
14) Bishop HC, Koop CE. Surgical management of duplications of the alimentary tract. Am J Surg 1964;107:434-42.
15) Iyer CP, Mahour GH. Duplications of the alimentary tract in infants and children. J Pediatr Surg 1995;30:1267-70.
16) Choi SO, Park WH, Kim SP. Enteric duplications in children.
J Korean Med Sci 1993;8:482-7.
17) Royle SG, Doig CM. Perforation of the jejunum secondary to a duplication cyst lined with ectopic gastric mucosa. J Pediatr Surg 1988;23:1025-6.
18) Ildstad ST, Tollerud DJ, Weiss RG, Ryan DP, McGowan MA, Martin LW. Duplications of the alimentary tract. Clinical char- acteristics, preferred treatment, and associated malformations.
Ann Surg 1988;208:184-9.
19) Stringer MD, Spitz L, Abel R, Kely E, Drake DP, Agrawal M, et al. Management of alimentary tract duplication in children. Br J Surg 1995;82:74-8.
20) Rathi V, Singh S, Bhargava SK, Kaur N, Seth N. Diagnosis of tubular colonic duplication by barium follow-through study.
Aus Radiol 2005;49:157-9.
21) Jo YC, Joo KR, Kim DH, Park JH, Suh JH, Kim YM, et al.
Duodenal duplication cyst manifested by acute pancreatitis and obstructive jaundice in an elderly man. J Korean Med Sci 2004;19:604-7.
22) Mattioli G, Buffa P, Pesce F, Barabino A, Ganduglia P, Fratino G, et al. Pancreatitis caused by duodenal duplication.
J Pediatr Surg 1999;34:645-8.
23) Sezgin O, Altiparmak E, Yilmaz U, Saritas U, Sahin B.
Endoscopic management of a duodenal duplication cyst asso- ciated with biliary obstruction in an adult. J Clin Gastroenterol 2001;32:353-5.
24) Holcomb GW III, Gheissari A, O'Neill JA Jr, Shorter NA, Bishop HC. Surgical management of alimentary tract dupli- cations. Ann Surg 1989;209:167-74.
25) Pinter AB, Schubert W, Szemledy F, Gobel P, Schafer J, Kustos G. Alimentary tract duplications in infants and children. Eur J Pediatr Surg 1992;2:8-12.
26) La Quaglia MP, Feins N, Eraklis A, Hendren WH. Rectal duplications. J Pediatr Surg 1990;25:980-4.
27) Schalamon J, Schleef J, Hollwarth ME. Experience with gas- trointestinal duplications in childhood. Langenbeck's Arch Surg 2000;385:402-5.
28) Galvez Y, Skaba R, Kalousova J, Rouskova B, Hribal Z, Snajdauf J. Alimentary tract duplications in children: high in- cidence of associated anomalies. Eur J Pediatr Surg 2004;
14:79-84.