Case Report
원고 접수일 2011년 8월 5일, 원고 수정일 2011년 9월 26일, 게재 확정일 2011년 10월 4일
책임저자 배정호
(139-707) 서울시 노원구 상계 7동 761-1, 인제대학교 의과대학 상계백병원 구강악 안면외과학교실
Tel: 02-950-1161, Fax: 02-950-1164, E-mail: [email protected]
RECEIVED August 5, 2011, REVISED September 26, 2011, ACCEPTED October 4, 2011
Correspondence to Jung-Ho Bae
Department of Oral and Maxillofacial Surgery, Sanggye Paik Hospital, Inje University College of Medicine
761-1, Sanggye 7-dong, Nowon-gu, Seoul 139-707, Korea
Tel: 82-2-950-1161, Fax: 82-2-950-1164, E-mail: [email protected]
CC This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
교근 내로 전이된 신세포암의 치험례
박군찬ㆍ윤규호ㆍ박관수ㆍ정정권ㆍ배정호ㆍ박재안ㆍ민성창ㆍ신재명1ㆍ백지선1ㆍ김현정2
인제대학교 의과대학 상계백병원 구강안악면외과학교실, 1일산백병원 구강악안면외과학교실, 2상계백병원 진단병리과학교실
Abstract
Intramasseteric Metastasis of Renal Cell Carcinoma: Case Report
Gun-Chan Park, Kyu-Ho Yoon, Kwan-Soo Park, Jeong-Kwon Cheong, Jung-Ho Bae, Jae-An Park, Sung-Chang Min, Jae-Myung Sin
1, Jee-Sun Baik
1, Hyun-Jung Kim
2Department of Oral and Maxillofacial Surgery, Sanggye Paik Hospital,
1Ilsan Paik Hospital,
2
Department of Pathology, Sanggye Paik Hospital, Inje University College of Medicine
Renal cell carcinoma (RCC) is the most frequent urological malignant tumor in adults and it occurs mostly between the fifth and the sixth decades of life. The male-female ratio is 3:1 and it is more common in smokers. It accounts for approximately 3% of adult malignancies; 90∼95% of neoplasms of the kidney. The classic triad of presenting symptoms of RCC is hematuria, back pain and a mass in the flank. More than 50% of RCCs show metastasis to breast, lung and regional lymph nodes, and 15% present in the orofacialmaxillary region. This case is about a 66 year-old man who was treated for painless swelling in the left masseteric area. The mass was surgically excised and sent for biopsy. It was diagnosed as RCC and two weeks later nephronectomy of the left kidney was performed. Metastasis to other organs was detected and the patient received radiation therapy. In this case we were able to find the primary lesion by the metastatic lesion.
Key words: Renal cell carcinoma, Metastasis, Masseteric muscle
서 론
신세포암은 신세뇨관 표피 세포에서 유래하는 악성 종양으로 성인에서 나타나는 신장 악성 종양에서 가장 높은 빈도(약 80%) 를 나타내는 종양으로 전체 성인 악성 종양의 약 3%를 차지한다.
모든 연령대에 발생할 수 있으나, 50, 60대에서 호발한다. 발생 성비는 남성 대 여성 3:1의 비로 남성에서 더 잘 나타나며, 흡연과
도 연관이 있는 것으로 알려져 있다. 임상적 주증상은 혈뇨, 배통, 옆구리 종물 등이며, 비특이 증상으로 비교적 많은 환자에서 도한 (night sweat), 열병(fever), 쇠약(weakness), 체중감소(weight loss), 간비장비대(hepatosplenomegaly) 등이 나타날 수 있다[1,2].
신세포암은 조직병리학적 소견으로 풍부한 소혈관을 포함하는
clear cell이 관찰되며, 면역화학적 소견으로 Vimentin, CD10,
Pancytokeratin 등에 양성 반응을 보인다. 신세포암은 폐, 골,
Fig. 1. (A) This case is about a 66
years old man who was treated for painless swelling on left masseteric area. (B) Pre-operative computed to- mography view: relatively well-de- fined heterogenous enhancing lobu- lated contour mass (2.8×2.5×2.6 cm) in left masster muscle (R/O heman- giopericytoma or R/O other mesen- chymal origin tumor).Fig. 2. (A) Peri-operative photo: sur-
gical excision, well encapsulated mass. (B) Peri-operative photo: fro- zen biopsy was done at 5 margins (negative response). (C) Gross find- ing, "intramasseteric muscular mass"is a well circumscribed nodular mass (3×2.8×2.8 cm) (Left) The cut surface of the mass is gray yellow- ish to brown without hemorrhage and necrosis (Right). (D) The micro- scopic finding well delineated from skeletal muscle fibers. The tumor cells are surrounded by sinusoid vessel (arrow) and composed of round epithelial cells (▶) with clear cytoplasms (H&E, ×100).
간 등으로 주로 전이되며, 두경부 영역으로의 전이는 매우 드문 것으로 알려져 있다[3,4].
신세포암은 서서히 성장하는 종양임에도 불구하고, 타 종양에 비해서 더욱 괴사적이고, 침습적이며, 광범위한 전이 등을 보이는 데, 신세포암 주변에 맥관 구조를 포함하는 경우가 많기 때문인 것으로 알려져 있다[5].
이번 증례는 저작근(본 증례의 경우 좌측 교근) 내의 종물이 먼저 발견되어, 종양 제거 및 조직, 면역학적 검사 결과 신세포암 으로 진단된 후, 신장 원발 병소를 발견했다는 점에서 매우 드물기 때문에 문헌 고찰과 함께 보고하는 바이다. 신세포암의 교근 내로 전이에 관한 증례보고는 단 1증례 보고되었을 뿐이다[2].
증례보고
66세 전신 질환이 없는 남성 환자가 좌측 교근 영역에서 약 3개월 전부터 인지된 종창을 주소로 본과에 내원하였다. 임상적 관찰에서는 약 3∼4 cm의 크기를 갖는 무통성의 비가동성 종물이 촉진되었다(Fig. 1A). 혈관조영제를 이용한 computed tomog- raphy (CT) 촬영 결과 좌측 교근 내에 약 2.8×2.5×2.6 cm 크기의 소엽화된 외형(lobulated contour)을 갖는 종괴가 주변과 다르게 강화된 상을 보이며, 종괴 주변에 있는 혈관 과잉이 관찰되 고 하악골과 경부근막은 손상받지 않았고, 양측 악하선에는 이상 소견이 관찰되지 않는 것 등이 관찰되었다. 이를 근거로 혈관주위 세포종(Hemangiopericytoma)으로 잠정 진단하였다(Fig. 1B).
초기 진단된 종물에 대한 확진을 위해 전신마취하에 동결 조직 생검(frozen biopsy)을 동반한 외과적 절제를 시행하였다(Fig.
2A). 외과적 수술 중 시행했던 다섯 부위의 종양 경계부 동결
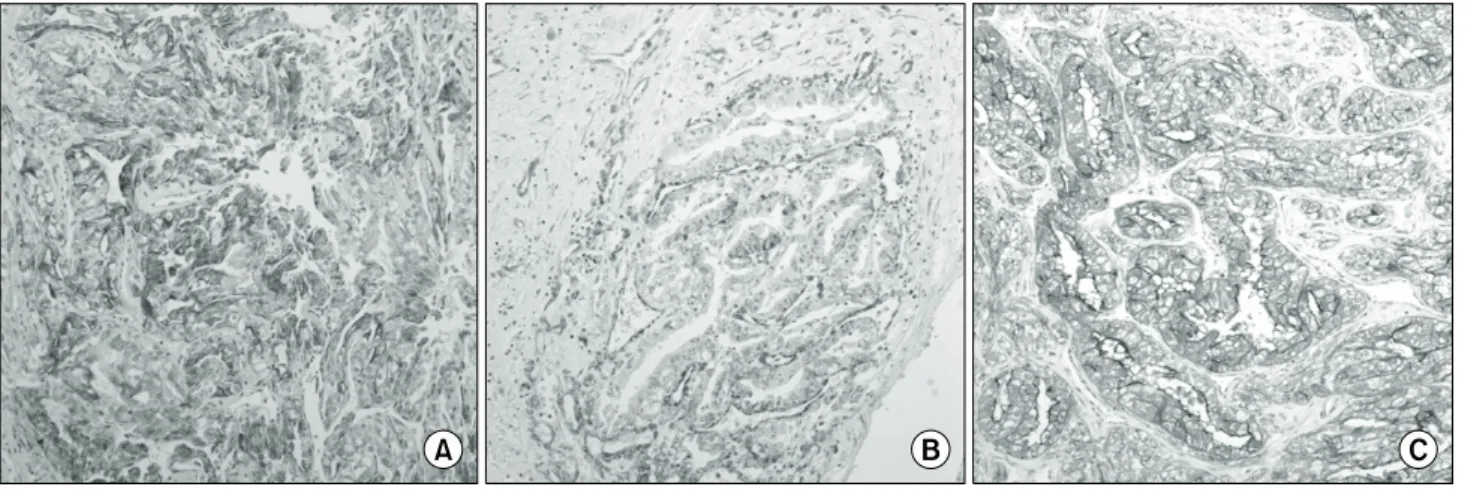
Fig. 3. The immunohistochemical stainings of the tumor cells result as follows: coexpression of pancytokeratin (A) & Vimentin (B),
and diffuse and strongly positive in CD10 (C) (H&E, ×100).Fig. 4. (A) Abdominal CT view: lobulating, exophytic heterogenous mass with wall-enhancement and delayed-washout (6.1×4.7 cm)
in mid portion of Lt. kidney. (B) Gross finding: "left radical nephrectomy specimen" consist of a kidney (12×8×4.5 cm), pro×imal ureter (7 cm in length 1.2 cm in greatest circumference), adrenal gland (4×5×2 cm), and peri-renal fat tissue (17×11×2.5 cm) and weighing totally 318 g. A lobulated firm mass (6.5×6×3 cm) is present at upper pole. The cut surface of the mass is golden yellowish with multifocal hemorrhage and necrosis. (C) The microscopic finding, kidney tumor sharply demarcated from intact renal cortex. The pattern and tumor cells are arranged in sinusoidal composed of clear cells similar to masseteric mass (H&E, ×100).조직 생검(frozen biopsy) 결과는 음성으로 나타났다(Fig. 2B).
외과적 절제술 결과 잘 피막화된 3 cm 크기의 종물(Fig. 2C)이 채취되었으며, 조직 병리적 소견에서는 골격근 섬유와 잘 구분되 며 동양 혈관(sinusoidal vessel)으로 둘러싸인 clear cell로 구성 된 종양 세포들이 관찰되었다(Fig. 2D). 또한 면역화학적 검사 결과에서는 Vimentin, CD10, Pancytokeratin 등에 양성을 보였 다(Fig. 3). 이러한 임상적, 조직학적, 면역학적 검사를 종합하여 신세포암의 전이 병소로 확정 진단할 수 있었다. 이후 원발 병소의 발견을 위하여 복부 및 흉부 CT를 촬영하였다(Fig. 4A). 이에 인지되지 않은 신장의 원발 병소를 발견하였고, 간과 폐 등의 다발성 전이 의심 병소 또한 발견할 수 있었다.
추가적인 진단과 처치를 위하여 비뇨기과로 전과하여 근치적 신장 절제술을 받았으며(Fig. 4B), 폐 전이에 대해 8주 동안 5-flu- orouracil, interferon-α과 interleukin-2을 이용한 면역요법을
시행하였다. 이후 폐 전산화 단층 촬영 결과 종양의 성장이 관찰되 어 Sunitinib malate (Sutene)을 이용한 경구 표적 항암 요법을 시행하였다.
환자는 임상적 검사 및 전산화 단층 촬영에 의한 주기적인 관찰을 시행 받았고, 관찰 중에 두경부 영역의 병소 및 전이는 관찰되지 않았다(Fig. 5). 하지만, 환자는 두경부 영역과는 관계 없이 폐 및 간에 발생한 다발성 전이병소로 신세포암의 교근 내 전이로 확진 후 13개월 뒤 사망하였다.
고 찰
신세포암은 신장 세뇨관의 표피에서 기원하는 종양으로 확실한
원인은 아직 밝혀지지 않았다. 다만, 환경 및 유전적 요인에 의한
것으로 추정되며, 흡연과 연관성이 높은 것으로 알려져 있다[2].
Fig. 5. (A) Post-oprative photo: no
palpable mass (7 months later). (B) Post-operative computed tomography view: no recurrence (7 months later).신세포암은 원발 병소의 임상적 증상 없이 전이되는 경우가 많아 전이 병소부의 임상적 증상이 발현된 경우라면 종양의 광범위한 전이를 암시한다. 주 전이는 폐에서 76%, 골에서 42%, 간에서 41%로 나타난다[5,6]. 신세포암은 특징적인 임상 증상 없이 서서 히 성장하는 특징을 갖는데 종양이 성장함에 따라 혈뇨 및 옆구리 통증 등이 나타날 수 있다. 전신 전이가 있는 경우 기침, 호흡곤란, 통증 등의 증상이 나타날 수 있다. 신세포암은 종양 주변에 매우 많은 맥관 구조를 포함하고 있기 때문에 다른 종양에 비해서 더욱 괴사적이고, 침습적이며, 광범위한 전이를 보일 수 있다[5,7].
악성 종양의 두경부 영역으로의 전이 경로는 동맥, 정맥, 림프 순환을 통하는 것으로 판단된다. 현재까지 가장 받아들여지는 이론은 종양 세포가 풍부한 신장의 국소 혈관망을 침투하여 전신 순환을 통해 전파되어, 흉골 내부나 복압이 증가했을 때 폐의 여과를 우회하여 역류함에 의해 전이된다는 이론이다. 만약, 폐의 병소와 관련이 없다고 판단된다면, 가능한 전이 경로는 Batson's 정맥총 또는 흉관이 있다. 특히, Batson's 정맥총은 두개골에서 천골까지 뻗어 있고, 판막이 없어 종양세포가 퍼지는 것에 덜 저항하는 것으로 여겨져 두경부 영역으로의 전이 경로로 받아들여 질 수 있다[8].
신세포암은 조직학적인 소견에서 clear cell 특징적으로 나타난 다. 이에 clear cell이 관찰되는 다른 종양인 선방세포암(acinic cell carcinoma), 점액표피양암종(mucoepidermoid carcino- ma), 원발성명세포함(primary clear cell carcinoma) 등과 감별 진단이 필요하다. 두경부 영역 전이 병소 감별진단을 위한 현미경 적 관찰에서 신세포암은 풍부한 맥관 구조로 둘러싼 증식된 신생 clear cell의 배열이 관찰되나 유사한 영역에서 발생한 타액선 종양에서는 이러한 구조가 관찰되지 않는다. 특히, 점액표피양암 종(mucoepidermoid carcinoma)에서 mucicarmin에 양성을 보이는 세포가 관찰되는 특징이 있어 신세포암과 쉽게 감별 진단
할 수 있다[5,9]. 다른 종양들과의 감별진단을 위하여 peri- odic-acid-Schiff 염색, 녹말 당화 효소와 같은 Enzyme test 및 CD10, Pancytokeratin, Vimentin과 같은 면역화학적 분석 등이 이용될 수 있다. 특히, Pancytokeratin, Vimentin의 동시 양성 반응은 다른 carcinoma에서는 잘 나타나지 않는 반응으로 신장 암 진단 표지자가 될 수 있다[7].
이번 증례에서는 조직학적인 관찰에서 신세포암에서 특징적인 소견인 clear cell이 나타났으며, 면역화학적 검사에서 CD10에 대해 강한 양성 반응을 보였고, Pancytokeratin 및 Vimentin에 동시 양성 반응을 나타내어 신세포암의 전이 병소로 확진할 수 있었다.
신세포암의 치료에는 외과적 절제, 방사선치료, 면역화학적 치료, 호르몬 치료 등이 이용될 수 있다. 하지만 장기간 생존율에 유의한 증가와 관련하여 이용 가능한 치료법은 없는 것으로 알려 져 있다. 신장 절제술 또한 환자의 전신 상태에 대한 호전을 보일 뿐 생존율을 높여주지는 못하는 것으로 보고되고 있다. 최근 의 연구에 따르면 전이의 수, 위치, 나타난 시기, 신장 절제술과 전이 병소의 절제술 등이 치료 예후를 결정하는 데 중요한 요소로 간주된다[10,11].
본 증례의 경우 본과에서 교근 영역에 종물에 대한 절제술, 비뇨기과에서 신장 절제술, 폐의 전이에 대해 면역요법제 (5-fluoronracil, interferon-α)를 이용한 치료를 시행하였으며, 경구 표적 항암 요법 Sunitinib malate (Sutene) 등의 치료가 시행되었다.
Böttiger[11]는 원거리 전이를 보이는 경우의 2년 생존율이
25%로 매우 불량한 예후를 나타냈으며, 특히 erythrocyte sed-
imentation rate의 수치가 30 이상일 경우 가장 불량한 예후를
보임을 밝혔다. 이러한 낮은 생존율을 이유로 빠른 진단과 세심한
치료를 주장하였다[12].
신세포암의 아류형(subtype)은 clear cell, papillary, chro- mophobe, collecting duct, unclassified 등으로 분류할 수 있 다. 이러한 아류형(subtype)은 예후와 연관되는데, clear cell type의 경우 전체 70%를 차지하며 5년 생존율이 약 60%이며, papillary type은 전체 15∼20%를 차지하며 5년 생존율이 80∼
90%를 나타낸다. Chromophobe type은 10%를 차지하며 5년 생존율이 90%이며, collecting duct type은 1% 이하이며 5년 생존율이 5% 미만이다[13]. 또한 최근 신세포암 예후에 관한 연구 에서 신장 절제술을 시행한 신세포암 환자에 대한 생존율과 유의 한 연관을 갖는 요소가 종양 stage, size (5 cm 이상), nuclear grade, necrosis임을 밝히고 이를 점수화한 stage size nuclear grade, necrosis (SSIGN) score를 이용하고 있다[14]. SSIGN의 값이 2인 환자의 5년 생존율은 평균 94.8%인 반면에 SSIGN 값이 8인 환자의 5년 생존율은 23.6%로 측정된다[14]. Subtype 분류와 SSIGN 점수를 토대로 임상가는 환자 예후 관리를 보다 쉽게 할 수 있고, 환자의 계층화를 통해 보조 치료를 효과적으로 시행할 수 있게 되었다. 또한 연관 요소에 대한 연구가 적절한 술 후 환자 생존 프로그램 개발에도 유용하게 사용될 수 있다[14,15].
본 증례와 같이 두경부 영역의 종양이 신세포암의 전이 병소로 진단되는 경우는 매우 드문 경우이다. 두경부 영역에 발생한 종양 은 대부분 신생종이며 전이에 의한 종양은 약 1%로 매우 드물고, 종양의 특성상 증상 발현 없이 발생하여 서서히 자라는 경우가 많기 때문에 진단이 매우 어려울 수 있다[15]. 그러므로 임상가는 두경부 영역에서 종양이 발견된 경우 감별 진단을 위하여 반드시 조직 병리 검사 및 면역화학적 검사를 통한 진단을 시행해야만 한다. 특히, 신세포암과 같이 예후가 불량한 악성 종양의 경우 빠른 진단을 통한 적절한 처치가 환자의 삶의 질을 향상시킬 수 있기 때문에 더욱 감별 진단에 유의하여야 한다.
References