156
서 론
위장관의 중복 낭종은 태생기 때 기관 형성의 이상으로 발생하는 선천성 기형으로 혀의 기저부에서부터 항문까지 의 장관 내 어디에서나 발생할 수 있다. 가장 흔한 호발 부 위는 회장 말단부위이며 그 외 십이지장, 공장, 위 등에서 고루 발생한다.(1) 식도 중복 낭종의 경우 위장관 중복 낭종 의 약 10% 에 해당하며 주로 식도의 하부 1/3 부분에서 발 생한다.(2,3) 식도 중복 낭종은 1711년 Blasius에 의해 처음 으로 보고되었고, 1931년 Sauerbruch가 첫 수술을 시행한 이 래 현재까지 여러 예가 보고되고 있으며, 평활근종(leiomyo- ma)을 제외하면 그 다음으로 흔한 식도의 양성 질환으로 일련의 부검에서 8,200 부검 예마다 1예(6/49,196)의 발생률 을 보인다.(3) 식도 중복 낭종의 경우 거의 대부분의 경우에 완전히 흉곽 내에 위치하거나 부분적으로 흉곽과 복강에 공히 존재하게 되는데,(4) 횡격막하 복부식도에 발생하여 복강 내에 국한되어 발견된 경우는 지금까지 매우 드물게 (4-9) 보고되고 있으며 소아에서의 보고 예는 Rathaus (9)의 5세 여아의 경우가 유일한 듯 더욱 드물어 보인다. 저자들은 최근 2개월 간의 간헐적인 심와부 동통과 오심, 구토를 주소 로 내원한 10세 11개월 된 남자 환아에서 선천성 횡격막하 식도 중복 낭종을 진단하고 수술적 치료로 증상이 소실된 예를 경험하였기에 문헌 고찰과 함께 보고하는 바이다.
증 례
환아는 10년 11개월 된 남아로 내원 전 약 2개월 동안 간 헐적인 심와부 통증과 오심, 구토를 호소하였다. 과거력에 서 5세와 7세 때 각각 서혜부 탈장 및 충수염으로 수술 받은 적이 있었으나 과거 다른 선천성 질환을 앓은 병력은 없었 다. 이학적 검사에서 경미한 오목 가슴 부위 압통이 관찰되 었으며 다른 특이 소견은 없었다. 혈액 검사를 포함한 기본 임상 검사에서도 특이 소견은 없었다.
위 내시경 소견: 소만 식도-위 경계 부위에 정상 점막으 로 덮여 있는 점막 하 종양의 소견을 보였다(Fig. 1).
방사선학적 소견
상부 위장관 조영술; 식도-위 경계에 가까운 원위부 식도
소아에서 발생한 횡격막하 식도 중복 낭종
인제대학교 의과대학 상계백병원 외과학교실 양 근 호․김 홍 주
Subdiaphragmatic Esophageal Duplication Cyst in a Child
Keun-Ho Yang, M.D. and Hong-Joo Kim, M.D.
An enteric duplication cyst is an unusual, benign congenital lesion of uncertain etiology. Duplications may be located anywhere along the alimentary tract from the mouth to the anus. Esophageal duplication cysts account for 10∼15% of all duplications, and combined autopsy series have estimated an incidence of 1 in 8,200. They can occur in any position related to the esophagus, but are most common in the lower third arising from the embryonic foregut, and are represented by a common spectrum of derivatives, such as bronchogenic cysts and ciliated hepatic foregut cysts. Many cases of esophageal duplication cysts have been reported, nearly all of which were either completely or partially within the thoracic cavity. However, reports of complete intra-abdominal cysts, so called subdiaphragmatic esophageal duplication cysts, are rare, especially in children. Herein, we report such a case that occurred in a 10-year-old boy, where a duplication cyst arose from the lower esophagus, remaining entirely confined within the abdomen of a child. The boy presented with a 2 month history of intermittent epigastric pain, nausea and vomiting. After surgical excision, the symptoms disappeared, with the diagnosis confirmed by histologic examination and fitting to the pathological criteria. (J Korean Surg Soc 2006;71:156-160)
Key Words: Esophagus, Duplication cyst, Subdiaphragmatic 중심 단어: 식도, 중복 낭종, 횡격막하
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Department of Surgery, Sanggye Paik Hospital, Inje Uni- versity College of Medicine, Seoul, Korea
책임저자:김홍주, 서울시 노원구 상계7동 761-1
ꂕ 137-707, 인제대학교 의과대학 상계백병원 외과 Tel: 02-950-1017, Fax: 02-933-9389
E-mail: [email protected]
접수일:2005년 12월 1일, 게재승인일:2006년 2월 17일 본 논문은 2002년 대한소아외과학회 춘계학술대회에서 구연되었음.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
우측으로 외부 압박(extrinsic compression) 소견이 보였다.
낭종과의 교통(communication)은 없으며 위 점막 또한 정상 소견을 보였다(Fig. 2).
복부 초음파 및 복부 단층 촬영; 위-식도 경계에 연하여 식도의 우측으로 약 4×3.5 cm 정도의 낭종이 관찰되었다 (Fig. 3).
수술 소견: 식도-위 경계 약 1.5 cm 전상방, 우측으로 4×3
cm 크기의 낭성 종물이 발견되었고 주위 조직과의 유착은 없었다. 단순 절제가 가능하였으며 식도 근육의 박리가 필 요하였으나 낭종과 식도 점막과의 교통은 없었고 점막 손 상 없이 장막의 일차 봉합을 시행하였다(Fig. 4).
조직학적 소견
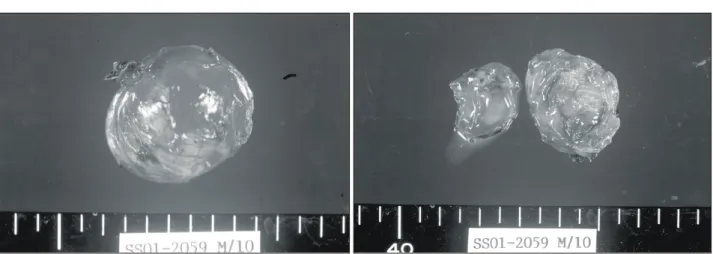
육안적 소견; 크기 4×3×2.5 cm, 무게 13.5 g의 원형 낭성 종물로 절단면상 단방성 낭종(unilocular cyst)이었고 우유빛 의 걸죽한 점액으로 채워져 있었다(Fig. 5).
현미경적 소견; 장막과 두층의 평활근으로 싸여져 있으 면서 상피는 위중층 섬모성 원주상피(pseudostratified cilia- ted columnar epithelium)로 구성되어 있었다(Fig. 6).
술 후 경과: 합병증 없이 수술 후 9일째 퇴원하였으며 만 5년이 경과한 현재 심와부 통증이나 그 외 여하의 위장관 증상 없이 경과 관찰 중이다.
Fig. 1. Normal gastric mucosa covering up the mass located in gastroesophageal junction. It looks like a submucosal tumor.
Fig. 2. Esophagogram shows extrinsic compression of distal esophagus with no evidence of barium leakage.
Fig. 3. Single cystic mass is noted at the medial side of distal esophagus in abdominal CT scan.
Fig. 4. The mass is identified in operative field, anteromedial side of intraabdominal esophagus near gastroesophageal junc- tion.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
고 찰
식도 중복 낭종은 1711년 Blasius에 의해 처음 기술되었 다.(4) 이는 비교적 흔치 않은 질환으로 모든 식도 종괴의 0.5∼2.5%를 차지하며 그럼에도 불구하고 식도 종괴의 대 부분을 차지하는 평활근종(leiomyoma)을 제외하면 그 다음 으로 흔한 양성 질환이다.(10,11) 식도 중복 낭종의 발생 원 인에 대해서는 1933년 Keith(12)가 선천적인 발생이상에 대 한 가설을 제기한 바 있으며 이후 1942년 Bremer(13)와 1973년 Kirwan(14)에 의해 거듭 주장되어 현재 가장 유력하 게 받아들여지고 있다. 이에 따르면 정상 전장(foregut) 발달 과정의 상피는 섬모성 원주 세포(ciliated columnar cell)로서 임신 4주경 이 상피세포들이 두꺼워지면서 관강(lumen)을 폐색시키게 되고 이들 세포의 분비물에 의하여 임신 6주경 폐색된 관강에 액포(vaculoe)가 생겨나게 된다. 이러한 액포
들의 융합과정을 통하여 새로운 관강이 형성되어 정상 식 도를 만들게 되는데 어떤 이유에 의해서 액포의 융합장애 가 발생한 경우 남아있게 되는 액포는 장관의 발생과정 중 에 식도의 측벽 내에서 낭종을 형성하게 된다.
전장 낭종(foregut cyst)은 발생학적인 기원과 현미경하에 서의 특징, 그리고 해부학적 위치에 따라 분류될 수 있다.
원시 전장(primitive foregut)에서 기원하는 낭종에는 식도 중 복 낭종, 기관지 낭종, 섬모성 간 전장 낭종(ciliated hepatic foregut cyst, CHFC), 위 낭종(gastric cyst) 등이 있을 수 있으 며 식도 중복 낭종으로 명명되기 위해서는 다음과 같은 세 가지 조직학적 진단 기준에 모두 합당해야 한다.(3) 1) 낭종 과 식도벽 사이의 연속성(continuity)의 존재, 2) 두층의 평활 근에 의해 둘러싸여 있는지 여부, 3) 상피세포는 4주 된 태 아의 상피세포, 즉 원주상피세포나 위중층 원주상피세포로 덮여있는지 여부(섬모성이거나 아닐 수도 있다) 등이다.
기관지 낭종의 경우도 위와 유사하나 낭종벽의 연골 조 Fig. 5. Gross specimen of 4×3×2.5 cm sized round cystic mass.
Fig. 6. In microscopic examination, pseudostratified ciliated columnar epithelium is confirmed. Gastric mucosa, cartilage, or bronchial glands are not founded in any other specimen section (H&E stain, ×100, ×40).
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 직이나 기관지선(bronchial gland)을 관찰함으로써 감별이
가능하고 위 낭종(gastric cyst)의 경우는 상피가 위 점막 (gastric mucosa)으로 덮여있으면서 위선(gastric gland)을 포 함하게 된다. 섬모성 간 전장 낭종(CHFC)은 태아의 상피세 포를 가진 간 실질의 낭종 병변일 경우 진단된다.(15,16) 본 증례의 검체는 장막과 두층의 평활근으로 싸여 있으 면서 상피는 위중층 섬모성 원주상피(pseudostratified ciliated columnar epithelium)로 구성되어 있음을 확인할 수 있었고 위점막(gastric mucosa)이나 연골조직, 기관지선(bronchial gland) 등이 관찰되지 않아 식도 중복 낭종 확진에 합당하다 고 판단하였다.
식도 중복 낭종의 증상은 소아의 경우 기관지 압박에 의 한 호흡곤란 증상이 주로 나타나며 성인의 경우 대부분 증 상이 없이 지내다가 우연히 발견되나 연하장애나 심와부 통증을 동반하기도 한다. 대부분의 식도 중복 낭종이 식도 하부 1/3에서 주로 발생한다는 점에서 상기의 증상 발현 양 상과 연관이 있으며 본 증례의 경우는 횡격막하 복부 식도 에 국한되어 발생한 경우로 식도-위 경계부위의 외부압박 에 의한 연하장애와 심와부 통증을 호소하였다.
식도 중복 낭종은 흉부 방사선 사진이나 상부 위장관 조 영술 등에 의해 종종 우연히 발견된다. 컴퓨터 복부 단순 촬영이나 복부 초음파에서 식도벽에 연하여 균질의 저음영 낭종의 소견을 보이며, 중복 낭종 또는 전장관(foregut) 기원 의 다른 선천성 낭종의 가능성을 감별해야 한다. 최근에는 내시경적 초음파 검사의 이용으로 낭종과 식도 사이의 근 육층의 연속성(continuity)을 관찰함으로써 수술 전 중복 낭 종의 감별진단에 도움을 받기도 한다.(17)
지금까지 여러 예의 식도 중복 낭종이 문헌을 통해 보고 되고 있으나 완전히 흉곽 내에 위치하게 되는 경우가 대부 분이다. 일부 흉곽 내의 식도 중복 낭종이 복강 내로 연장된 경우가 있으나(18-21) 본 증례와 같이 횡격막하 복부식도에 발생하여 복강 내에 국한되어 발견된 경우는 매우 드물게 보고되고 있는 듯하며,(4-9) 소아에서의 발생 예는 더욱 드 물어 보인다.
의증의 확진은 조직병리 결과에 의해서만 가능하며 또한 증상의 소실과 천공, 출혈, 감염, 악성변화(22) 등의 발생 가 능한 합병증을 예방하기 위해서도 낭종의 수술적 제거가 적절한 치료방법으로 추천된다. 수술적 제거 후의 단기 성 적은 매우 좋으나 장기적으로는 64%의 환자에게서 위-식도 역류에 의한 증상이 나타나는 것으로 보고되고 있으며 93%
에서 원위부 식도의 해부학적 이상이 관찰된다고 한다.(23) 이에 대한 원인은 명확하진 않지만 식도 근육층의 낭종을 제거하는 과정에서 하부 식도 괄약근의 장력이 감소하여 발생하는 것으로 생각한다. 본 증례의 경우 5년여 간의 추 적관찰한 결과 현재까지 역류성 식도염의 증상을 포함한 다른 위장관 증상은 나타나지 않았으며 앞으로 증상이 발 생하게 되면 위내시경 및 상부 위장관 조영술을 이용하여
식도-위 경계부위의 해부학적 평가를 수행할 계획이다.
REFERENCES
1) Choi SO, Park WH, Kim SP. Enteric duplications in child- ren. J Korean Med Sci 1993;8;482-7.
2) Anderson M, Silverman W, Shields TW. Duplications of the alimentary tract. Arch Surg 1962;85;110-24.
3) Arbona JL, Fazzi JGF, Mayoral J. Congenital esophageal cysts:
case report and review of the literature. Am J Gastroenterol 1984;79:177-82.
4) Ruffin WK, Hansen DE. An esophageal duplication cyst pre- senting as an abdominal mass. Am J Gastroenterol 1989;
84:571-3.
5) Suzuki T, Atari E, Okudaira M, Yosida M, Hiki Y, Kakita A. A case report of abdominal congenital esophageal cyst in adult. Jpn J Gastroenterol 1992;89:2700-4.
6) Harvell JD, Macho JR, Klein HZ. Isolated intra-abdominal esophageal cyst: case report and review of the literature. Am J Surg Pathol 1996;20:476-9.
7) Karahasanoglu T, Ozbal A, Alcicek S, Goksel S, Altun M.
Giant intra-abdominal esophageal duplication cyst. Endoscopy 1997;29:54-5.
8) Henry J, Paul NF. Isolated intraabdominal esophageal cyst.
AJR 1998;170:389-90.
9) Rathaus V, Freinberg MS. Subdiaphragmatic esophageal dup- lication cyst in a child. J Clin Ultrasound 2000;28;264.
10) Whitaker JA, Deffenbaugh LD, Cooke AR. Esophageal dup- lication cyst. Am J Gastroenterol 1980;73:329-32.
11) Anderson HA, Pluth JR. Benign tumors, cyst, and duplica- tions of the esophagus. In: Payne WS, Olsen AM, editors. The esophagus. 1st ed. Philadelphia: Lea and Febiger; 1974.
p.225-37.
12) Keith A. Human embriology and morphology. 5th ed. Balti- more: William Wood & Company; 1933.
13) Bremer JL. Diverticula and duplication of the intestinal tract.
Arch Pathol 1942;38:132-40.
14) Kirwan WO, Walbaum PR, McCormac RJM. Cystic intra- thoracic derivatives of the foregut and their complications.
Thorax 1973;28:424-8.
15) Wheeler DA, Edmondson HA. Ciliated hepatic foregut cyst.
Am J Surg Pathol 1984;8:467-70.
16) Vick DJ, Goodman ZD, Deavers MT, Cain J, Ishak KG.
Ciliated hepatic foregut cyst: a study of six cases and review of the literature. Am J Surg Pathol 1999;23:671-7.
17) Bhutani MS, Hoffmann BJ, Reed C. Endosonographic dia- gnosis of an esophageal duplication cyst. Endoscopy 1996;
28:396-7.
18) Bishop HC, Koop CE. Surgical management of duplications of the alimentary tract. Am J Surg 1964;107:434-42.
19) Grossfield JL, O'Neill JA, Clatworthy W. Enteric duplica- tions in infancy and childhood; 18 year review. Ann Surg
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 1970;172:83-9.
20) Shepherd MP. Thoracic, thoraco-abdominal, and abdominal duplications. Thorax 1965;20:82-6.
21) Pokorny WJ, Goldstein IR. Enteric thoracoabdominal duplications in children. J Thorac Cardiovasc Surg 1984;87:
821-4.
22) Tapia RH, White VA. Squamous cell carcinoma arising in a duplication cyst of the esophagus. Am J Gastroenterol 1986;
81:325-9.
23) Salo JA, Ala-Kulju KV. Congenital esophageal cysts in adul- ts. Ann Thorac Surg 1987;44:135-8.