Original Article
pISSN 2233-9019 · eISSN 2233-9116
Korean J Fam Pract. 2015;5(3, suppl. 2):641-646
KJFP
Korean Journal of Family PracticeOriginal Article
pISSN 2233-9019 · eISSN 2233-9116 Korean J Fam Pract. 2015;5(3, suppl. 2):PB-1
KJFP
Korean Journal of Family Practice서 론
위식도 역류질환( gastroesophageal reflux disease , GERD )이란 위 나 십이지장 내용물이 식도 내로 반복적으로 역류하여 여러 가지 임 상 증상을 나타내거나 식도의 조직 병리학적, 방사선학적, 내시경적 변화를 초래한 상태를 총칭하는 용어이다.
1)역류성 식도염은 GERD 의 아군( subgroup )으로 위식도 역류에 의한 내시경적 혹은 병리학 적 식도점막의 손상을 일으키며, 내시경 검사, 바륨식도조영술 등 여러 가지 다양한 검사를 통해 진단 할 수 있다.
2)서구에서의 유병률 은 10 ~ 20 % 정도로 비교적 높게 보고되는 질병이지만,
3)우리나라에 서는 과거 대부분의 보고가 10 % 이내로 서양에 비하여 낮은 편이었
다,
4, 5)하지만 최근에는 11 . 8 ~ 17 . 3 %로 증가되어 보고되고 있다.
6, 7)또한, 평균수명의 증가와 생활양식의 서구화 및 하부식도 괄약근 압 을 저하시키는 약제사용의 증가 등으로 추후 빈도가 더욱 증가할 것
으로 추정되나 역류성 식도염의 유병률에 관련된 전국 규모의 전향 연구는 아직 없는 실정이다.
고민감도 C -반응단백( high sensitivity C - reactive protein , hs - CRP )은 전형적인 급성단계의 반응물질로서 여러 종류의 염증반응 이나 조직 손상에서 증가하며 정상인에서는 매우 낮은 농도로 존재 한다.
8)hs - CRP 는 여러 염증성 사이토카인들에 반응하여 간에서 생 성되며, 혈청 지질 농도 및 죽상경화와 관련이 있고 심혈관 질환의 독립적인 예측인자로 이용할 수 있다. 9 , 10 ) 또한 hs - CRP 의 증가는 비록 정상 범위에 있더라도 대사증후군과 2 형 당뇨병의 중요한 전구 단계가 될 수 있다고 보고되었다.
11, 12)역류성 식도염이 식도점막의 손상이나 염증성 변화의 특징을 가 지고 있으므로 다양한 염증반응이나 조직 손상시 증가하는 hs - CRP 와도 연관되어 있을 것으로 생각되어 역류성 식도염의 중증도에 따 른 계량화된 hs - CRP 의 농도를 구체적으로 확인해보고자 본 연구에
역류성 식도염과 고민감도 C-반응단백과의 상관성
윤영보, 김은기
*, 박찬욱, 류보석, 박주화, 고준, 서해원
청주한국병원 가정의학과
The Correlation between Reflux Esophagitis and High sensitivity C-reactive protein
Young-Bo Yun, Eun-Ki Kim
*, Chan-Wook Park, Bo-Seok Ryu, Joo-Hwa Park, Jun Ko, Hae-Won Seo
Department of Family Medicine, Hankook hospital, Chungju, KoreaBackground: We studied the correlation between reflux esophagitis and high sensitivity C-reactive protein, one of the acute phase reactants.
Methods: This study was performed with the participation of 764 males and females who visited a health promotion center from 1 August to 31 October, 2013. We examined the participants’ questionnaires, body weight, body mass index, blood pressure, laboratory data, and upper gastrointestinal endoscopy. High sensitivity C-reactive protein was compared between the control group and the other group diagnosed with reflux esophagitis using upper gastrointestinal endoscopy. The endoscopic severity of reflux esophagitis was classified on the basis of the Los Angeles grading classification system.
Results: The comparison of high sensitivity C-reactive protein among participants revealed that it increased as the severity of reflux esophagitis increased (P<0.001). Quintile-based analysis of high-sensitivity C-reactive protein revealed that patients with a high level of high sensitivity C-reactive protein were more likely to have reflux esophagitis with high severity.
Compared to quintile 1, the odds ratios for quintile 2 and 3 were 0.83 and 3.11, respectively (95% confidence interval 0.45-1.51, 1.81-5.33).
Conclusion: This study showed quantitatively a significant positive correlation between high sensitivity C-reactive protein and the severity of reflux esophagitis.
Keywords: reflux esophagitis;upper gastrointestinal tract endoscopy;Los Angeles grading classification system;C-reactive protein
Received July 23, 2015 Revised July 23, 2015 Accepted September 8, 2015 Corresponding Author Eun-Ki Kim
Tel: +82-43-222-7000, Fax: +82-43-255-7007 E-mail: [email protected]
Copyright © 2015 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Young-Bo Yun, et al. The Correlation between Reflux Esophagitis and High sensitivity C-reactive protein
Korean Journal of Family Practice
KJFP
서는 역류성 식도염의 중증도에 따른 hs - CRP 의 농도와의 상관성 에 대해 알아보았다.
방 법
1. 연구대상
2013 년 8 월 1 일부터 2013 년 10 월 31 일까지 지방의 일개 종합병 원 건강검진센터 방문자 중에서 상부위장관 내시경 검사를 받은 18 세에서 81 세의 총 764 명을 대상으로 하였고, 그 중 남자 401 명, 여 성 363 명이었다. 급성 감염성 질환, 심혈관질환, 당뇨, 만성신부전, 고지혈증, 고혈압, 자가면역질환 등의 과거력이 있는 환자는 제외 하였다. 간질환, 비만(체질량 지수 30kg / m
2초과), 현재 흡연자, 수 술 받은 환자, 외상이 있는 환자, 염증상태를 의심할 수 있는 백혈 구수가 10 × 103 / μL 이상인 경우와 hs - CRP 가 10mg / dL 이상인 경우, statin 계열의 약제를 사용하는 경우들도 제외하였다.
2.연구방법
1) 설문 조사
연구 대상자들에게 먼저 설문조사를 시행하였다. 조사 내용은 현 병력, 과거 병력, 흡연력 등에 관한 것이었다.
2) 신체 계측 및 혈액검사
기본적인 신체검사와 검사실 검사를 위해 측정 전 최소 8 시간 이상 금식을 한 후, 다음날 오전에 채혈을 시행하였고, 검진용 가 운을 착용하고 신발을 벗은 상태에서 신체검사를 시행하였다. 체 중과 체질량지수는 X - SCAN PLUS II ( Zawon Medical , Daegu , Korea )를 이용하여 측정하였고, 혈압은 대상자가 최소 10 분 이상 안정을 하도록 한 후 앉은 자세에서 Standby baumanometer ( W . A . BAUM CO . INC ., Coriague , N . Y ., USA )를 이용하여 측정하 였다. 채혈한 혈액은 바로 검사실로 보내 검사를 실시하였다. 백 혈구수( WBC )는 ADVIA 2120i ( Siemens . Dublin , Ireland )를 이 용하여 측정하였고, 혈중 총콜레스테롤과 중성지방은 Toshiba TBA200FR ( Toshiba Co . Ltd ., Tokyo , Japan )를 이용하여 효소 비색법( enzymatic colorimetric method )으로 측정하였고, 저밀 도지단백( low - density lipoprotein , LDL ) 콜레스테롤, 고밀도 지단백( high - density lipoprotein , HDL ) 콜레스테롤은 Toshiba TBA200FR ( Toshiba Co . Ltd ., Tokyo , Japan )을 사용하여 직접측 정법으로 측정하였다. 공복혈당은 포도당 산화효소법( LX - 20 , Beckman Coulter , Fullerton , CA , USA )으로 측정하였다. hs - CRP 는 Toshiba TBA200FR ( Toshiba Co . Ltd ., Tokyo , Japan ) 장비 및 Denka CRP - LATEX Ⓡ X2 ( Denka Seiken Co . Ltd , Japan ) 시약
키트로 면역응집법을 이용하여 검사하였다.
3) 상부소화관 내시경 검사
역류성 식도염은 내시경에 숙련된 4 명의 가정의학과 전문의에 의해 내시경 Olympus Q160 ( Olympus Medical systems Corp ., Tokyo , Japan )으로 진단하였다. 역류성 식도염은 Los Angeles Grading Classification System ( LA - A , LA - B , LA - C , LA - D ) 으로 분류하였다.
13)또한, 뚜렷한 점막손상은 없으나 점막의 백색 혼탁으로 인해 식도 경계인 Z 선( Z - line ) 주위에 식도점막의 주행 ( palisading ) 혈관이 전혀 안보이거나 Z 선 불선명( blurring )이 확 실한 경우만을 점막의 미세변화( minimal change , MC )라고 하였 다.
14, 15)4) 통계분석
정상인에서의 hs - CRP 는 매우 낮은 수치이기 때문에 삼분위수 를 이용하여 그 차이를 분석하였고, 모든 데이터는 평균± 표준편 차 혹은 해당 값(%)으로 표시하였다. 역류성 식도염의 중증도와 hs - CRP 를 비교 시 두 군 간의 차이는 independent t - test 와 chi - square test , 세 군 이상의 차이는 one way ANOVA test 와 chi - squre test 로 통계적 유의성을 확인하였다. 그 결과 개별적으로 유의 하게 나온 변수들을 포함하여 ordinal logistic regression 을 실시하 여 역류성 식도염의 중증도와 hs - CRP 의 삼분위수 세 구간의 관련 성을 분석하였다. 통계 프로그램은 Window 용 SPSS ver . 13 . 0 ( SPSS Inc ., Chicago , IL , USA )을 사용하였고, 통계적 유의 수준은 P - value
<0 . 05 로 하였다.
결 과
1. 연구대상자의 일반적인 특징
연구 대상자는 총 764 명(남자 401 명, 여자 363 명)으로 평균 연
령은 42 . 9 ± 9 . 6 세이었으며, 상부위장관 내시경 소견 상 정상 621
명( 81 . 3 %), MC 16 명( 2 . 1 %), LA - A 및 LA - B 127 명( 16 . 7 %)이고
LA - C , LA - D 에 해당하는 대상자는 없었다. 평균 체중은 63 . 0 ±
10 . 4kg , 평균 체질량지수는 22 . 6 ± 2 . 6kg / m
2이었고, 평균 수축기
혈압과 이완기혈압은 각각 112 . 5 ± 11 . 3mmHg , 72 . 0 ± 8 . 6mmHg
이었다. 평균 백혈구 수치는 5 . 9 ± 1 . 4 × 103 / μL 이었으며 총콜레
스테롤과 HDL 콜레스테롤, LDL 콜레스테롤, 중성지방은 각각
189 . 4 ± 26 . 4mg / dL , 58 . 8 ± 14 . 1mg / dL , 114 . 6 ± 24 . 7mg / dL ,
91 . 5 ± 50 . 7mg / dL 이었다. 공복혈당은 94 . 1 ± 11 . 1mg / dL 이었으
며, hs - CRP 는 0 . 094 ± 0 . 147mg / dL 이었다( Table 1 ).
윤영보 외. 역류성 식도염과 고민감도 C-반응단백과의 상관성 Korean Journal of Family Practice
KJFP
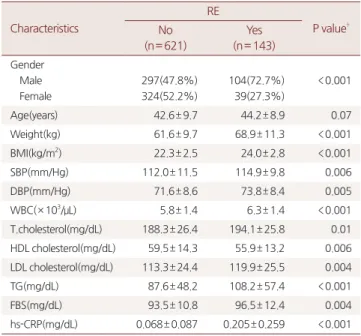
2. 역류성 식도염 유무에 따른 임상적, 혈액학적 특징
역류성 식도염이 없는 정상군 총 621 명 중 남성은 297 명( 47 . 8 %), 여성은 324 명( 52 . 2 %)이었으며, 역류성 식도염군 총 143 명 중 남 성은 104 명( 72 . 7 %), 여성은 39 명( 27 . 3 %)으로 역류성 식도염군에 서 남성의 비율이 더 높았다. 연령은 정상군에서 42 . 6 ± 9 . 7 세, 역 류성 식도염군에서 44 . 2 ± 8 . 9 세로 유의한 차이를 보이지 않았다.
HDL 콜레스테롤을 제외한 체중, 체질량지수, 혈압, 백혈구수, 총 콜레스테롤, LDL 콜레스테롤, 중성지방, 공복혈당은 정상군에서보 다 역류성 식도염군에서 더 높았으며 통계학적으로 유의한 차이를 보였다. hs - CRP 도 정상군과 역류성 식도염군에서 각각 0 . 068 ± 0 . 087mg / L , 0 . 205 ± 0 . 259mg / L 로 역류성 식도염군에서 더 높았 으며 통계학적으로 유의한 차이를 보였다( P
<0 . 001 )( Table 2 ).
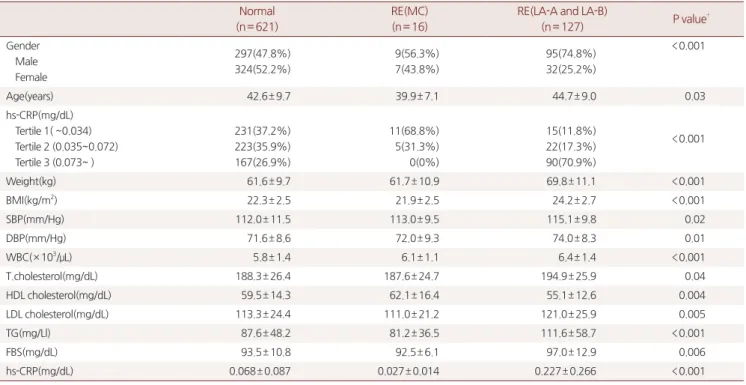
3. 역류성 식도염의 중증도와 hs-CRP와의 상관관계
역류성 식도염의 중증도에 따른 hs - CRP 를 비교하였을 때 MC 를 제외한 LA - A 및 LA - B 로 갈수록 hs - CRP 가 증가하였 다( P
<0 . 001 ). 연령, 체중, 체질량지수, 수축기혈압, 이완기혈 압, 백혈구수, 총콜레스테롤, LDL 콜레스테롤, 중성지방, 공복혈 당( P = 0 . 03 , P = 0 . 04 , P
<0 . 001 , P
<0 . 001 , P = 0 . 02 , P = 0 . 03 ,
P
<0 . 001 , P = 0 . 01 , P
<0 . 001 , P = 0 . 003 )도 MC 를 제외한 LA - A 및 LA - B 에서 증가하였다. 하지만 HDL 콜레스테롤은 MC 를 제외 한 LA - A 및 LA - B 에서 감소하였다( P = 0 . 004 )( Table 3 ).
역류성 식도염의 중증도에 따른 hs - CRP 의 삼분위수와 비교 시 개별적으로 유의하게 나온 변수들(성별, 연령, 체중, BMI , 수축 기혈압, 이완기혈압, 백혈구수, 총콜레스테롤, HDL 콜레스테롤, LDL 콜레스테롤, 중성지방, 공복혈당)을 포함하여 ordinal logistic regression 을 실시하였다. 그 결과 2 구간을 제외하고 3 구간에서 hs - CRP 가 높을수록 내시경적 중증도가 높은 그룹에 속할 확률이 높았 으며, hs - CRP 1 구간에 비해 2 , 3 구간의 교차비( odds ratio )가 각각 0 . 83 , 3 . 11 ( 95 % 신뢰구간 0 . 45 ~ 1 . 51 , 1 . 81 ~ 5 . 33 )이었다( Table 4 ).
고 찰
위식도역류질환은 임상에서 흔히 접하게 되며 이의 병태생리에 대한 이해와 진단 및 치료 방법이 발전함에 따라 서구에서는 다양한 진료지침이 개발, 개정되고 있으며,
16, 17)국내에서도 위식도역류질 환의 임상진료지침 개정안이 마련되었다.
18)내시경 검사는 역류성 식도염의 표준진단검사로 점막손상의 정도와 합병증, 바렛식도의
Table 1. The general characteristics of study subjects*Characteristics Total†(n= 764)
Gender Male Female
401(52.5%) 363(47.5%)
Age(years) 42.9± 9.6
Endoscopic findings Normal RE(MC) RE(LA-A and LA-B)
621(81.3%) 16(2.1%) 127(16.7%)
Weight(kg) 63.0± 10.4
BMI(kg/m2) 22.6± 2.6
SBP(mmHg) 112.5± 11.3
DBP(mmHg) 72.0± 8.6
WBC(× 103/μL) 5.9± 1.4
T.cholesterol(mg/dL) 189.4± 26.4
HDL cholesterol(mg/dL) 58.8± 14.1
LDL cholesterol(mg/dL) 114.6± 24.7
TG(mg/dL) 91.5± 50.7
FBS(mg/dL) 94.1± 11.1
hs-CRP(mg/dL) 0.094± 0.147
* Data are analyzed by Frequency and Descriptive analysis.
† Data are presented as Number(%) or mean±standard deviation.
Abbreviations: n, number; RE, reflux esophagitis; MC, minimal change; LA, Los Angeles classification; BMI, body mass index calculated as weight in kilograms divided by height in meters squared; SBP, systolic blood pressure; DBP, diastolic blood pressure; WBC, white blood cell; T.cholesterol, total cholesterol; HDL, high density lipoprotein; LDL, low density lipoprotein; TG, triglyceride; FBS, fasting blood sugar; hs-CRP, high sensitivity C-reactive protein.
Table 2. Clinical and laboratory characteristics of the subjects by RE*
Characteristics
RE
P value† No
(n= 621)
Yes (n= 143) Gender
Male Female
297(47.8%) 324(52.2%)
104(72.7%) 39(27.3%)
<0.001
Age(years) 42.6± 9.7 44.2± 8.9 0.07
Weight(kg) 61.6± 9.7 68.9± 11.3 <0.001
BMI(kg/m2) 22.3± 2.5 24.0± 2.8 <0.001
SBP(mm/Hg) 112.0± 11.5 114.9± 9.8 0.006
DBP(mm/Hg) 71.6± 8.6 73.8± 8.4 0.005
WBC(× 103/μL) 5.8± 1.4 6.3± 1.4 <0.001
T.cholesterol(mg/dL) 188.3± 26.4 194.1± 25.8 0.01 HDL cholesterol(mg/dL) 59.5± 14.3 55.9± 13.2 0.006 LDL cholesterol(mg/dL) 113.3± 24.4 119.9± 25.5 0.004
TG(mg/dL) 87.6± 48.2 108.2± 57.4 <0.001
FBS(mg/dL) 93.5± 10.8 96.5± 12.4 0.004
hs-CRP(mg/dL) 0.068± 0.087 0.205± 0.259 <0.001
* Data are presented as Number(%) or mean±standard deviation.
† P value are analyzed by chi-square test and independent t-test , and statistically significant P < 0.05 are shown.
Abbreviations: RE, reflux esophagitis; n, number; BMI, body mass index calculated as weight in kilograms divided by height in meters squared; SBP, systolic blood pressure; DBP, diastolic blood pressure; WBC, white blood cell;
T.cholesterol, total cholesterol; HDL, high density lipoprotein; LDL, low density lipoprotein; TG, triglyceride; FBS, fasting blood sugar; hs-CRP, high sensitivity C-reactive protein.
Young-Bo Yun, et al. The Correlation between Reflux Esophagitis and High sensitivity C-reactive protein
Korean Journal of Family Practice
KJFP
이형성을 알 수 있지만 진단 민감도가 낮은 단점이 있다.
19)hs - CRP 는 간에서 합성되고 IL - 6 , TNF - α 와 같은 사이토카인 에 의해서 조절되는 급성 반응성 물질로 그 정확한 기능은 알려져 있지는 않지만 조직인자( tissue factor )의 형성이나 보체를 활성화하 는데 관여하는 것으로 생각된다.
20)hs - CRP 는 체질량지수, 중성지 방, HDL 콜레스테롤, 총콜레스테롤, 혈압 등과 관련이 있다고 보 고되고 있다.
21-24)본 연구에서는 Roberts 등
25)의 연구에서 제시한 기준에 따라 hs -
CRP 의 정상수치 상한값을 10mg / dL 로 정하였다. 일반적으로 hs - CRP 10mg / dL 이상의 수치는 급성 감염이나 전신 염증의 가능성이 높으므로 hs - CRP 10mg / dL 이상의 수치는 연구 대상에서 제외하 였다.
본 연구에서는 역류성 식도염이 있는 환자들을 대상으로 hs - CRP 의 상승과 LA 분류를 이용하여 상부위장관 내시경으로 증명된 점막 손상 정도와의 상관성을 분석하였다. 본 연구에서 LA - C 및 LA - D 에 해당하는 대상자는 없었는데, 이는 건강검진 수검자들을 대상으로 하였기 때문인 것으로 생각된다.
본 연구에서 역류성 식도염의 중증도와 hs - CRP 간의 유의한 상 관관계가 있었다. Rifai 등
26)의 연구에서 hs - CRP 를 오분위수로 구 분하여 정상인에서도 오분위수의 단계가 증가 할수록 심혈관 질환 의 상대위험도가 증가하였음을 보고한바 있다. 따라서 건강검진 수 검자에서의 hs - CRP 는 매우 낮으므로 그 차이로 인한 임상적 의의 를 쉽게 발견하기 어려운 점으로 인해 오분위수로 구분하고자 하였 으나, 본 연구에서는 표본의 크기가 작아 이를 삼분위수로 나누었 으며 역류성 식도염 분류상 LA - A 와 LA - B 도 묶어서 분석하였으 며, hs - CRP 삼분위수 중 1 구간을 기준으로 2 구간, 3 구간에서의 역 류성 식도염의 중증도와의 교차비를 구하였다. 그 결과 역류성 식 도염의 중증도는 hs - CRP 삼분위수 중 3 구간에 속할 경우가 1 구간 에 비해 증가할 가능성이 3 . 11 배이었다. 물론 2 구간에서는 음의 상
Table 4. Risk of belonging to higher endoscopic severity group of reflux esophagitis according to hs-CRP
Tertile of hs-CRP
Level of hs-CRP
(mg/dL) OR* 95% CI
(Lower-Upper) P value†
1 ≦0.034) 1 NA‡ NA‡
2 0.035-0.072 0.83 0.45-1.51 0.53
3 ≥ 0.073 3.11 1.81-5.33 <0.001
* odds ratio adjusting for gender, age, weight, body mass index, systolic blood pressure, diastolic blood pressure, white blood cell, total cholesterol, high density lipoprotein cholesterol, low density lipoprotein cholesterol, triglyceride, fasting blood sugar.
† P value are analyzed by ordinal logistic regression and statistically significant P<0.05.
‡ NA not applicable.
Abbreviation: hs-CRP, high sensitivity C-reactive protein; OR, odds ratio; CI, confidence interval.
Table 3. Difference of variables among RE groups*
Normal (n= 621)
RE(MC) (n= 16)
RE(LA-A and LA-B)
(n= 127) P value†
Gender Male Female
297(47.8%) 324(52.2%)
9(56.3%) 7(43.8%)
95(74.8%) 32(25.2%)
<0.001
Age(years) 42.6± 9.7 39.9± 7.1 44.7± 9.0 0.03
hs-CRP(mg/dL) Tertile 1( ~0.034) Tertile 2 (0.035~0.072) Tertile 3 (0.073~ )
231(37.2%) 223(35.9%) 167(26.9%)
11(68.8%) 5(31.3%) 0(0%)
15(11.8%) 22(17.3%) 90(70.9%)
<0.001
Weight(kg) 61.6± 9.7 61.7± 10.9 69.8± 11.1 <0.001
BMI(kg/m2) 22.3± 2.5 21.9± 2.5 24.2± 2.7 <0.001
SBP(mm/Hg) 112.0± 11.5 113.0± 9.5 115.1± 9.8 0.02
DBP(mm/Hg) 71.6± 8.6 72.0± 9.3 74.0± 8.3 0.01
WBC(× 103/μL) 5.8± 1.4 6.1± 1.1 6.4± 1.4 <0.001
T.cholesterol(mg/dL) 188.3± 26.4 187.6± 24.7 194.9± 25.9 0.04
HDL cholesterol(mg/dL) 59.5± 14.3 62.1± 16.4 55.1± 12.6 0.004
LDL cholesterol(mg/dL) 113.3± 24.4 111.0± 21.2 121.0± 25.9 0.005
TG(mg/Ll) 87.6± 48.2 81.2± 36.5 111.6± 58.7 <0.001
FBS(mg/dL) 93.5± 10.8 92.5± 6.1 97.0± 12.9 0.006
hs-CRP(mg/dL) 0.068± 0.087 0.027± 0.014 0.227± 0.266 <0.001
* Data are presented as Number(%) or mean±standard deviation.
† P value are analyzed by chi-square test and one way ANOVA that used to evaluated differences in the 4 groups and statistically significant P < 0.05.
Abbreviations: RE, reflux esophagitis; MC, minimal change; LA, Los Angeles classification; n, number; BMI, body mass index calculated as weight in kilograms divided by height in meters squared; SBP, systolic blood pressure; DBP, diastolic blood pressure; WBC, white blood cell; T.cholesterol, total cholesterol; HDL, high density lipoprotein;
LDL, low density lipoprotein; TG, triglyceride; FBS, fasting blood sugar; hs-CRP, high sensitivity C-reactive protein.
윤영보 외. 역류성 식도염과 고민감도 C-반응단백과의 상관성 Korean Journal of Family Practice
KJFP
관관계를 보였다.
본 연구는 몇 가지 면에서 한계를 갖고 있다. 첫째, 건강검진센터 를 방문한 사람들을 대상으로 하여 표본의 크기가 작으며, 단면적 연구( cross sectional study )라는 한계가 있다. 둘째, 상부위장관 내 시경 검사는 숙련된 전문의에 의해 시행되었지만 1 명이 아니라 여 러 명이 시행하였으므로 검사자에 따라 역류성 식도염 진단율의 차 이가 있을 수 있으며, 다른 전문가들에 의해 그 결과를 검토하는 과 정은 없었다. 이번 연구에서 역류성 식도염 유병률은 LA 분류를 기 본으로 한 건강검진자 대상의 국내 연구의 역류성 식도염 유병률보 다는 약간 높은 수치를 보였다. 상부위장관 내시경 소견 상 LA - C , D 에 해당하는 역류성 식도염 대상자가 없어 전 인구집단에 대한 대 표성이 부족한 점도 들 수 있다. 셋째, 이번 연구에서 LA 분류에 포 함시켰던 미세변화에 대한 진단율이 전문가에 의해 따라 매우 다양
하며
27, 28)관찰자간의 일치율이 낮다는 점이며,
29)아직까지도 미세
변화에 대한 표준 정의가 아직 없으며 미세변화에 상응하는 조직학 적 변화의 증거나 역류치료에 대한 반응에 대한 보고가 많지 않다.
넷째, 흡연은 hs - CRP 를 증가 시키는 것으로 알려져 있어서 흡연 에 의한 영향력을 통제하기 위해 비흡연자만을 대상으로 분석을 하 였지만, 간접흡연에 노출되는 정도에 따라 hs - CRP 가 증가할 가능 성이 있으므로 결과 분석에 영향을 주었을 가능성을 배제하지 못한 다. 다섯째, 역류성 식도염의 발생에 영향을 미칠 수 있는 식생활이 나 음주 여부, 위산 분비, 내장 민감도, 헬리코박터 감염, 위의 내용 물 제거 기능, 인슐린, 렙틴, 에스트로겐, 성장인자 등 원인을 규명 하기 위한 다양한 조사를 하지는 못하였다. 여섯째, 단 한 번의 혈 액 채취를 통해 hs - CRP 를 측정하였으므로 각 개인의 hs - CRP 변 동에 대해 정확한 평가를 하기 힘들며, hs - CRP 가 저평가 되었을 가능성이 있다.
결론적으로 이러한 한계점에도 불구하고 아직까지 우리나라를 포함한 동양인을 대상으로 하여 역류성 식도염의 중증도에 따른 hs - CRP 의 상관성에 관한 연구가 없었기 때문에, 본 연구가 역류성 식도염의 중증도에 따른 계량화된 hs - CRP 의 농도를 제시했다는 점에서 의미가 있다고 할 수 있겠다.
요 약
연구배경: 본 연구에서는 염증과 조직 손상 시에 증가하는 급성 반 응물질인 고민감도 C -반응단백을 이용해 역류성 식도염과의 상관 성을 알아보고자 하였다.
방법: 지방의 일개 종합병원의 건강검진 수진자 남, 여 총 764 명을 대상으로 하여 설문지를 작성하고, 체중, 체질량지수, 혈압 측정과 혈액검사 및 상부위장관 내시경 검사를 시행하였다. 상부위장관 내
시경 검사 상 정상군과 역류성 식도염군으로 나누어 고민감도 C - 반응단백과의 상관성을 분석하였다. 역류성 식도염은 Los Angeles 분류를 이용하였다.
결과: 고민감도 C -반응단백은 상부위장관 내시경 검사상 정상군 ( 0 . 068 ± 0 . 087 )과 미세변화군( 0 . 027 ± 0 . 014 )에 비해 Los Angeles 분류 A 및 B ( 0 . 227 ± 0 . 266 )로 갈수록 증가하는 양상을 보였다 ( P
<0 . 001 ). 고민감도 C -반응단백을 삼분위수로 나누어서 분석한 결과, 2 구간을 제외하고 고민감도 C -반응단백이 증가할수록 역류 성 식도염의 중증도가 높은 그룹에 속할 확률이 높았다. 1 구간에 비 해 2 , 3 구간의 교차비( odds ratio )가 각각 0 . 83 , 3 . 11 ( 95 % 신뢰구간 0 . 45 ~ 1 . 51 , 1 . 81 ~ 5 . 33 )이었다.
결론: 역류성 식도염의 중증도가 높아질수록 고민감도 C -반응단백 이 증가하는 통계적으로 유의한 양의 상관관계가 있었으며, 본 연 구에서는 역류성 식도염의 중증도에 따른 계량화된 hs - CRP 의 농 도를 제시했다.
중심단어: 역류성 식도염,상부위장관 내시경, Los Angeles 분류,고 민감도 C -반응단백
REFERENCES
1. Fock KM, Talley NJ, Fass R, Goh KL, Katelaris P, Hunt R, et al.
Asia-Pacific consensus on the management of gastroesophageal reflux disease: update. J Gastroenterol Hepatol 2008;23:8-22.
2. Fass R, Ofman JJ. Gastroesophageal reflux disease-should we adopt a new conceptual framework? Am J Gastroenterol 2002;97(8):1901- 9.
3. Loffeld RJ, van der Putten AB. Rising incidence of reflux oesophagitis in patients undergoing upper gastrointestinal endoscopy. Digestion 2003;68(2-3):141-4.
4. Youn YH, Kang YW, Ahn SH, Park SK. Prevalence alteration of reflux esophagitis in recent years, Korean J Gastrointest Endosc 2001;23:144-8.
5. Jeon SG, Rhee PL, Shin MH, Hyun JG, Lee HY, Sohn CI, et al. The prevalence and risk factors of reflux esophagitis in routine check- up subjects. Korean J Gastroenterol 1998;32:701-8.
6. Yoo SS, Lee WH, Ha J, Choi SP, Kim HJ, Kim TH, et al. The prevalence of esophageal disorders in the subjects examined for health screening. Korean J Gastroenterol 2007;50:306-12.
7. Hwang JK, Kim J, Hong SG, Jung SJ, Joo MK, Lee BJ, et al. A prospective multicenter study on the prevalence and symptoms of erosive reflux esophagitis in secondary and tertiary hospitals in Korea. Korean J Gastroenterol 2009 ;53(5):283-91.
8. Ridker PM, Buring JE, Cook NR, Rifai N. C-reactive protein, the metabolic syndrome, and risk of incident cardiovascular events:
an 8-year follow-up of 14 719 initially healthy American women.
Circulation 2003;107(3):391-7.
Young-Bo Yun, et al. The Correlation between Reflux Esophagitis and High sensitivity C-reactive protein
Korean Journal of Family Practice
KJFP
9. Tracy RP, Lemaitre RN, Psaty BM, Ives DG, Evans RW, Cushman M, et al. Relationship of C-reactive protein to risk of cardiovascular disease in the elderly. Results from the Cardiovascular Health Study and the Rural Health Promotion Project. Arterioscler Thromb Vasc Biol 1997;17:1121-7.
10. Rohde LE, Hennekens CH, Ridker PM. Survey of C-reactive protein and cardiovascular risk factors in apparently healthy men.
Am J Cardiol 1999;84:1018-22.
11. Rutter MK, Meigs JB, Sulivan LM, D'Agostino RB Sr, Wilson PW. C-reactive protein, the metabolic syndrome, and prediction of cardivascular events in the Framingham Offspiring Study.
Circulation 2004;110:380-5.
12. Han TS, Sattar N, Williams K, Gonzalez-Villalpando C, Lean ME, Haffner SM. Prospective study of C-reactive protein in relation to the development of diabetes and metabolic syndrome in the Mexico City Diabetes Study. Diabetes Care 2002;25:2016-21.
13. Armstrong D, Bennett JR, Blum AL, Dent J, De Dombal FT, Galmiche JP, et al. The endoscopic assessment of esophagitis:
a progress report on observer agreement. Gastroenterology 1996;111(1):85-92.
14. Kusano M, Shirai N, Yamaguchi K, Hongo M, Chiba T, Kinoshita Y, et al. It is possible to classify non-erosive reflux disease(NERD) patients into endoscopically normal groups and minimal change groups by subjective symptoms and responsiveness to rabeprazole - a report from a study with Japanese patients. Dig Dis Sci 2008;53(12):3082-94.
15. Lee JH, Lee JS, Rhee PL, Chun HJ, Choi MG, Bak YT, et al. Interobserver Variation in the Endoscopic Diagnosis of Gastroesophageal Reflux Disease. Korean J Gastrointest Endosc 2006;33(4):197-203.
16. DeVault KR, Castell DO; American College of Gastroenterology.
Updated guidelines for the diagnosis and treatment of gastroesophageal reflux disease. Am J Gastroenterol 2005;100(1):190-200.
17. Hirano I, Richter JE; Practice Parameters Committee of the American College of Gastroenterology. ACG practice guidelines:
esophageal reflux testing. Am J Gastroenterol 2007;102(3):668-85.
18. Jung HK, Hong SJ, Jo YJ, Jeon SW, Cho YK, Lee KJ, et al. Updated guidelines 2012 for gastroesophageal reflux disease. Korean J Gastroenterol 2012 ;60(4):195-218.
19. Gasiorowska A, Fass R. The proton pump inhibitor (PPI) test in GERD: does it still have a role? J Clin Gastroenterol 2008;42(8):867-74.
20. Ridker PM, Rifai N, Rose L, Buring JE, Cook NR. Comparison of C-reasctive protein and low-density lipoprotein cholesterol levels in the prediction of first cardiovascular events. N Engl J Med 2002;347:1557-65.
21. Haverkate F, Thompson SG, Pyke SD, Gallimore JR, Pepys MB.
Production of C-reactive protein and risk of coronary events in stable and unstable angina. European Concerted Action on Thrombosis and Disabilities Angina Pectoris Study Group. Lancet 1997;349(9050):462-6.
22. Yudkin JS, Stehouwer CD, Emeis JJ, Coppack SW. C-reactive protein in healthy subjects: associations with obesity, insulin resistance, and endothelial dysfunction: a potential role for cytokines originating from adipose tissue? Arterioscler Thromb Vasc Biol 1999;19(4):972-8.
23. Koenig W, Sund M, Fröhlich M, Fischer HG, Löwel H, Döring A, et al. C-Reactive protein, a sensitive marker of inflammation, predicts future risk of coronary heart disease in initially healthy middle- aged men: results from the MONICA (Monitoring Trends and Determinants in Cardiovascular Disease) Augsburg Cohort Study, 1984 to 1992. Circulation 1999;99(2):237-42.
24. Mendall MA, Patel P, Ballam L, Strachan D, Northfield TC. C reactive protein and its relation to cardiovascular risk factors: a population based cross sectional study. BMJ 1996;312(7038):1061- 5.
25. Roberts WL, Moulton L, Law TC, Farrow G, Cooper-Anderson M, Savory J. Evaluation of nine automated high-sensitivity C-reactive protein methods; implications for clinical and epidemiological applications. Part 2. Clin Chem 2001;47:418-25.
26. Rifai N, Ridker PM. High sensitivity C-reactive protein:a novel and promising marker of coronary heart disease. Clin Chem 2001;47:403-11.
27. Nakamura T, Shirakawa K, Masuyama H, Sugaya H, Hiraishi H, Terano A. Minimal change oesophagitis: a disease with characteristic difference to erosive oesophagitis. Aliment Pharmacol Ther 2005;21(suppl 2):S19-26.
28. Kiesslich R, Kanzler S, Vieth M, Moehler M, Neidig J, Thanka Nadar BJ, et al. Minimal change esophagitis: prospective comparison of endoscopic and histological markers between patients with non- erosive reflux disease and normal controls using magnifying endoscopy. Dig Dis 2004;22(2):221-7.
29. Amano Y, Ishimura N, Furuta K, Okita K, Masaharu M, Azumi T, et al. Interobserver agreement on classifying endoscopic diagnoses of nonerosive esophagitis. Endoscopy 2006;38(10):1032-5.