서 론
2015년 통계청 사망원인 통계에 따르면 우리나라의 순환기계통 질환에 의한 사망은 인구 10만 명당 116.9명으로 전체 사망원인의 21% 가량 차지하고 있다.1) 대사증후군은 복부 비만, 높은 혈압, 고혈 당, 이상지질혈증 등 여러 대사 이상의 집합체로서 제 2형 당뇨병과
심혈관계 질환을 예측할 수 있는 주요 위험인자이다.2,3) 국민건강영 양조사 자료에 따르면 20세 이상 성인에서 대사증후군의 유병률은 증가하는 양상을 보이고 있다.4)
C-반응성 단백(C-reactive protein, CRP)은 급성기 반응성 단백질 중 하나로 신체의 전반적인 염증반응 정도를 나타내는 지표이며 심 혈관계 염증 반응 및 혈전의 형성에도 직접적인 관련이 있는 것으로
Received July 21, 2017 Revised October 24, 2017 Accepted October 26, 2017
Corresponding author Jin A Park Tel: +82-2-901-3114, Fax: +82-2-901-3174 E-mail: [email protected]
ORCID: http://orcid.org/0000-0001-6982-9309
Copyright © 2018 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons At- tribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Original Article
https://doi.org/10.21215/kjfp.2018.8.5.684 eISSN 2233-9116
Korean J Fam Pract. 2018;8(5):684-689
Korean Journal of Family Practice
KJFP
성인에서 High-Sensitivity C-Reactive Protein과
대사증후군과의 연관성: 2015년 국민건강영양조사를 활용
김성겸, 박진아*, 함상근, 신민우, 유은혜, 손용호
한일병원 가정의학과
The Relation of High-Sensitivity C-Reactive Protein with Metabolic Syndrome in Korean Adults:
Based on the Korean Health and Nutrition Examination Survey, 2015
Sung Kyum Kim, Jin A Park*, Sang Keun Ham, Min Woo Shin, Eun Hye Yu, Yong Ho Sohn Department of Family Medicine, Hanil General Hospital, Seoul, Korea
Background: Metabolic syndrome is a group of multiple metabolic disorders that increase the risk of cardiovascular diseases and type 2 diabetes.
C-reactive protein (CRP) level is a marker of systemic inflammation, and its correlation with coronary arterial disease has recently been highlighted.
The purpose of this study was to determine the relationship between metabolic syndrome and CRP level, as well as between each metabolic syndrome component and CRP level.
Methods: On the basis of the data from the Sixth Korea National Health and Nutrition Examination Survey conducted in 2015, 3,705 people were selected. They were grouped according to general and lifestyle characteristics such as age, sex, alcohol drinking, and smoking status. The correlation of high-sensitivity (hs-CRP) level according to these variables was analyzed statistically. The correlation between each component of the metabolic syndrome and hs-CRP level was examined using one-way analysis of variance. Finally, the association of hs-CRP level with metabolic syndrome was examined using logistic regression analysis.
Results: hs-CRP level correlated with male sex, age, high-risk drinking, and smoking status. Overall, high hs-CRP level correlated with the high incidence rate of metabolic syndrome. The metabolic syndrome components such as waist circumference, triglyceride level, high-density lipoprotein cholesterol level, blood pressure, and blood glucose level showed statistically significant correlations with hs-CRP level.
Conclusion: Each metabolic syndrome component showed a significant difference according to hs-CRP level. The group with metabolic syndrome had a high hs-CRP level as a whole. This study showed that high hs-CRP levels were also associated with the prevalence of metabolic syndrome.
Keywords: Korea National Health and Nutrition Examination Survey; Metabolic Syndrome; High-Sensitivity C-Reactive Protein; Korean Adult
김성겸 외. 성인에서 hs-CRP와 대사증후군과의 연관성 Korean Journal of Family Practice
KJFP
알려져 있다.5) 기존의 연구는 CRP 농도와 심혈관 질환 사이의 유의 한 상관관계를 보여주고 있다.6-8) CRP는 정상인에서는 매우 낮은 농 도로 존재하며 그 농도를 고감도 분석을 이용하여 측정하는 고감도 C-반응성 단백(high-sensitivity CRP, hs-CRP)은 건강한 성인에서 심 혈관 질환 관련 위험성을 예측 할 수 있는 인자로 사용되고 있다.9)
국민건강영양조사는 국가를 대표하는 신뢰성을 갖춘 통계 자료 로 여러 연구 및 보건정책의 기초자료로 활용되고 있다. 제6기 3차년 도(2015년) 혈액검사에서 hs-CRP가 처음으로 측정된 바 본 연구는 2015년 자료를 이용하여 분석함으로써 대사증후군과 hs-CRP와의 관계를 알아보고자 하였다.
방 법
1. 연구 대상
본 연구를 위해 국민건강영양조사 제6기 3차(2015년) 원시자료를 활용하였다. 전체 대상자 7,380명에서 만 19세 이상 80세 미만 성인 5,945명 중 주요 변인에 결측값이 존재하는 1,347명과 악성 종양, 자 가면역질환 유병자, 염증 상태를 의심할 수 있는 백혈구 10,000/µL 이 상, hs-CRP 10 mg/dL 이상 중 한 개 조건이라도 해당되는 893명을 제 외하여 최종 3,705명을 연구 대상자로 선정하였다.
2. 연구 변수 선정과 정의
국민건강영양조사 제6기 3차 원시자료에 기입된 허리둘레, 중성 지방(triglyceride, TG), 고밀도지단백 콜레스테롤(high-density lipo- protein [HDL] cholesterol), 수축기 혈압, 이완기 혈압, 공복혈당, hs- CRP 수치 및 성별, 연령, 음주, 흡연 변수 등의 일반적 특성 및 생활습 관 관련 변수를 활용하였다.
흡연은 현재 흡연군, 과거 흡연군, 비흡연군으로 분류 하였고 음주 는 금주군, 적정 음주군, 고위험 음주군(평균 음주량이 7잔[여자5 잔]) 이상이고, 주 2회 이상 음주)으로 분류하였다.
대사증후군은 2012년 대한비만학회의 비만치료지침과 National Cholesterol Education Program, Adult Treatment Panel III (NCEP ATP III) 진단 기준에 따라 다음 5가지 항목 중 3가지 이상에 해당하는 경 우를 대사증후군이라 정의하였다.10,11)
1) 허리둘레(남 ≥90 cm, 여 ≥85 cm) 2) TG (≥150 mg/dL)
3) HDL 콜레스테롤(남 <40 mg/dL, 여 <50 mg/dL) 4) 혈압(수축기 ≥130 mmHg 또는 이완기 ≥85 mmHg) 5) 공복혈당(≥100 mg/dL)
정상인에서 hs-CRP는 보통 매우 낮은 수치로 측정되기 때문에 사
분위수로 나누어 분석하였고 0.30 mg/dL 이하인 경우 ‘하(1사분위)’
집단으로, 0.30 mg/dL을 초과하고 0.50 mg/dL 이하인 경우는 ‘중하(2 사분위)’ 집단으로, 0.50 mg/dL을 초과하고 0.90 mg/dL 이하인 경우 는 ‘중상(3사분위)’ 집단으로, 0.90 mg/dL을 초과하는 경우는 ‘상(4사 분위)’ 집단으로 분류하였다.
3. 통계 분석
본 연구에서는 단순임의표본설계가 아닌 2단계 층화집락표본설 계를 이용하여 추출된 국민건강영양조사 원시자료를 활용하였기 때문에 복합표본 분석을 실시하였다. 층화, 집락 변수를 적용하고 설 문·검진조사 가중치를 적용하여 복합표본 설계를 하였다.
연구 대상자의 hs-CRP 수준에 따라 일반적 특성과 대사증후군 해당 비율을 확인하기 위해 카이제곱 검정(chi-square test)을 이용하 였고 hs-CRP 수준별로 대사증후군 관련 수치의 평균을 비교하기 위 해 일원배치 분산분석(one-way ANOVA analysis)을 이용하였다. 대사 증후군 진단 기준 항목 각각의 해당 여부에 따라 hs-CRP 수치의 평 균을 비교하기 위해 독립표본 t-검정(independent t-test)을 이용하였 고 hs-CRP 수준이 대사증후군 발생 가능성에 미치는 영향을 검증 하기 위해 로지스틱 회귀분석(logistic regression analysis)을 이용하였 다.
모든 분석은 IBM SPSS statistics ver. 22.0 (IBM Co., Armonk, NY, USA)을 이용하였으며, 통계적 유의성 수준은 P<0.05로 정의하였다.
결 과
1. hs-CRP군에 따른 일반적 특성과 대사증후군 비율
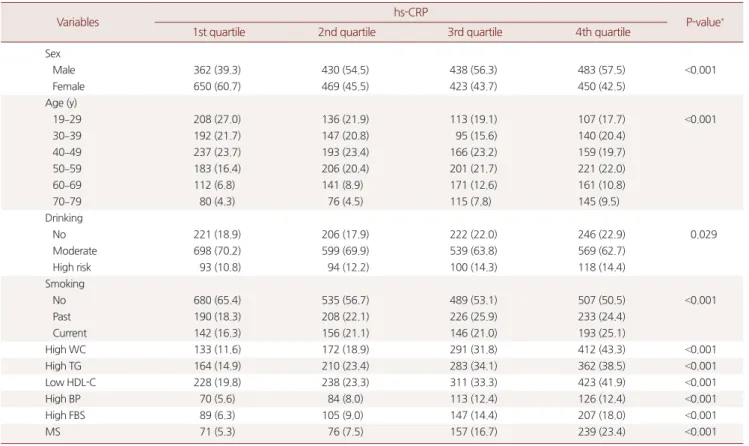
hs-CRP 수준에 따라 일반적 특성과 대사증후군 비율에 유의한 차이를 보이는지 검증하기 위해 카이제곱 검정을 이용하였다. 성별 항목에서는 hs-CRP가 높아질수록 남성의 비율이 높아지고 여성의 비율이 낮아지는 것으로 나타났다. 연령은 50대 이상에서 hs-CRP가 높아질수록 비율이 점차 증가하는 경향을 보였다. 음주는 hs-CRP가 제 3사분위군 이상으로 높은 군일수록 비음주와 고위험 음주의 비 율이 높게 나타났으며, 적정 음주 비율은 낮아지는 경향을 보였다.
흡연은 hs-CRP가 높은 군일수록 현재 흡연의 비율이 높아지는 경향 을 보였고 비흡연의 비율은 낮아지는 경향을 보였다. 대사증후군 항 목에서는 hs-CRP가 높은 군일수록 대사증후군 비율이 높아지는 양 상을 보였다(Table 1).
2. hs-CRP군에 따른 대사증후군 진단 기준 항목의 평균 비교 hs-CRP 군별로 대사증후군 진단 기준 항목을 비교하기 위해 일원
Original Article
Korean Journal of Family Practice
Sung Kyum Kim, et al. The Relation of hs-CRP with Metabolic Syndrome in Korean Adults
Korean Journal of Family Practice
KJFP
배치 분산분석(one-way ANOVA analysis)을 이용하였으며 hs-CRP가 높은 군일수록 허리둘레, TG, 혈압, 공복혈당은 높아지며 HDL 콜레 스테롤은 낮아지는 등 모든 대사증후군 진단 기준 항목의 평균이 hs-CRP 수준에 따라 유의한 차이를 보였다(Table 2).
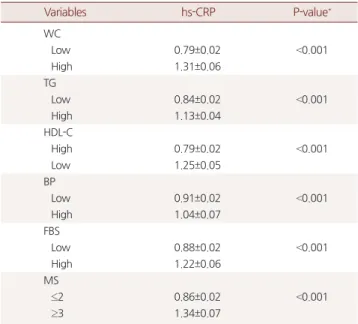
3. 대사증후군 진단 기준 항목 해당 여부에 따른 hs-CRP 평균 비교
대사증후군 진단 기준 항목의 해당 여부에 따라 hs-CRP 수치의 평균을 비교하기 위해 독립표본 t-검정(independent t-test)을 이용하 였으며 허리둘레, TG, HDL 콜레스테롤, 혈압, 공복혈당이 대사증후 군 진단 기준에 해당하는 경우 hs-CRP 평균이 전반적으로 높은 것 Table 2. Metabolic syndrome component according to hs-CRP
Variables hs-CRP
P-value*
1st quartile 2nd quartile 3rd quartile 4th quartile
WC 76.86±0.36 80.22±0.41 83.72±0.36 86.95±0.43 <0.001
TG 103.06±2.85 128.27±5.06 151.89±5.59 159.64±5.68 <0.001
HDL-C 56.70±0.48 53.01±0.50 49.75±0.47 47.19±0.50 <0.001
SBP 111.43±0.56 114.95±0.58 118.11±0.64 119.25±0.57 <0.001
DBP 72.65±0.39 75.04±0.46 76.60±0.43 76.43±0.41 <0.001
FBS 93.67±0.47 96.10±0.59 99.85±0.94 102.08±1.02 <0.001
Values are presented as mean±standard deviation.
hs-CRP, high-sensitivity C-reactive protein; WC, waist circumference; TG, triglyceride; HDL-C, high density lipoprotein-cholesterol; BP, blood pressure; FBS, fasting blood glucose.
*Calculated by one-way ANOVA.
Table 1. Subject characteristics by hs-CRP
Variables hs-CRP
P-value*
1st quartile 2nd quartile 3rd quartile 4th quartile
Sex
Male 362 (39.3) 430 (54.5) 438 (56.3) 483 (57.5) <0.001
Female 650 (60.7) 469 (45.5) 423 (43.7) 450 (42.5)
Age (y)
19–29 208 (27.0) 136 (21.9) 113 (19.1) 107 (17.7) <0.001
30–39 192 (21.7) 147 (20.8) 95 (15.6) 140 (20.4)
40–49 237 (23.7) 193 (23.4) 166 (23.2) 159 (19.7)
50–59 183 (16.4) 206 (20.4) 201 (21.7) 221 (22.0)
60–69 112 (6.8) 141 (8.9) 171 (12.6) 161 (10.8)
70–79 80 (4.3) 76 (4.5) 115 (7.8) 145 (9.5)
Drinking
No 221 (18.9) 206 (17.9) 222 (22.0) 246 (22.9) 0.029
Moderate 698 (70.2) 599 (69.9) 539 (63.8) 569 (62.7)
High risk 93 (10.8) 94 (12.2) 100 (14.3) 118 (14.4)
Smoking
No 680 (65.4) 535 (56.7) 489 (53.1) 507 (50.5) <0.001
Past 190 (18.3) 208 (22.1) 226 (25.9) 233 (24.4)
Current 142 (16.3) 156 (21.1) 146 (21.0) 193 (25.1)
High WC 133 (11.6) 172 (18.9) 291 (31.8) 412 (43.3) <0.001
High TG 164 (14.9) 210 (23.4) 283 (34.1) 362 (38.5) <0.001
Low HDL-C 228 (19.8) 238 (23.3) 311 (33.3) 423 (41.9) <0.001
High BP 70 (5.6) 84 (8.0) 113 (12.4) 126 (12.4) <0.001
High FBS 89 (6.3) 105 (9.0) 147 (14.4) 207 (18.0) <0.001
MS 71 (5.3) 76 (7.5) 157 (16.7) 239 (23.4) <0.001
Values are presented as number (%).
hs-CRP, high-sensitivity C-reactive protein; WC, waist circumference; TG, triglyceride; HDL-C, high density lipoprotein-cholesterol; BP, blood pressure; FBS, fasting blood glucose; MS, metabolic syndrome.
*Calculated by chi-square test.
김성겸 외. 성인에서 hs-CRP와 대사증후군과의 연관성 Korean Journal of Family Practice
KJFP
으로 나타났다(Table 3).
4. hs-CRP 군에 따른 대사증후군 및 진단 기준 항목의 교차비 hs-CRP 수치에 따라 대사증후군 및 진단 기준 항목의 교차비를 파악하기 위해 성별과 연령, 그리고 생활 습관 관련 변수인 음주, 흡 연의 영향력을 보정하여 로지스틱 회귀분석을 실시하였다.
hs-CRP 수치에 따른 교차비는(제 1사분위 대비 제 4사분위) 복부 둘레 4.99배(P<0.001), TG 2.88배(P<0.001), 낮은 HDL 콜레스테롤 2.98 배(P<0.001), 고혈압 1.93배(P<0.001), 고혈당 2.33배(P<0.001), 대사증후 군 4.41배(P<0.001)로 높게 나타나 hs-CRP 수치가 높아질수록 대사 증후군 가능성이 높아지는 것으로 확인되었다(Table 4).
고 찰
대사증후군과 CRP는 심혈관계 질환과 관련이 있음이 여러 연구 에서 밝혀졌다. West Scotland Coronary Prevention Study와 Framing- ham Offspring Study 등의 역학 연구에서 대사증후군과 CRP가 심혈 관계 질환 이환율과 사망률의 증가와 관련이 있음이 확인되었었 다.12,13)
또한, Mirhafez 등14)과 Kazemi-Bajestani 등15)의 연구는 hs-CRP와 대사증후군 모든 요인들과 연관성이 있다고 보고하였고 Bustos 등16) 의 연구에서는 남성의 경우 TG, 복부비만 항목들만, 여성의 경우 복 부비만 항목만 제한적으로 CRP와 관련이 있다고 발표한 바 있다. 또 Vidyasagar 등17)의 연구에서는 복부비만, 고혈당 항목만이 CRP와 관 련이 있었다,
국내에서는 Kim 등18)과 Jung등19)의 연구에서 CRP와 대사증후군 의 모든 진단 기준 항목들과 관련이 있다고 보고하였고, Park 등20)의 연구에서 CRP는 여성에서만 대사증후군의 진단 기준 항목들과 연 관성이 있고 남성에서는 유의한 상관 관계가 없다고 보고하였다.
본 연구에서는 hs-CRP가 대사증후군의 모든 진단 기준 항목들과 관련성이 높게 나타났다. 또한, hs-CRP 수치에 따라 대사증후군 및 진단 기준 항목의 교차비를 파악하기 위해 성별과 연령, 음주, 흡연 을 보정한 로지스틱 회귀분석에서 hs-CRP 수치가 높아질수록 대사 증후군 가능성도 높아지는 것으로 확인되었다. 특히 복부비만이 대 사증후군의 병태생리의 중요 요인으로 알려져 있는 것처럼 허리둘 레의 교차비가 가장 높은 것으로 나타났다. 흡연과의 연관성은 hs- CRP가 높아질수록 현재 흡연의 비율이 높아지는 경향을 보였고 비 흡연의 비율은 낮아지는 경향을 보여 흡연과 hs-CRP의 양의 상관관 계가 확인되었다. 음주의 경우 hs-CRP가 상승 할수록 적정 음주 비 율은 낮아지는 경향을 보였으나 명확한 연관성을 확인하기는 어려 웠다.
Table 4. Odds ratios of hs-CRP on metabolic syndrome
Variables hs-CRP
P-value*
1st quartile 2nd quartile 3rd quartile 4th quartile
WC 1.00 1.63 (1.20–2.23) 3.03 (2.20–4.17) 4.99 (3.62–6.88) <0.001
TG 1.00 1.51 (1.11–2.07) 2.41 (1.77–3.28) 2.88 (2.24–3.71) <0.001
HDL-C 1.00 1.29 (1.00–1.67) 2.02 (1.59–2.58) 2.98 (2.35–3.78) <0.001
BP 1.00 1.30 (0.87–1.95) 1.97 (1.33–2.90) 1.93 (1.33–2.82) <0.001
FBS 1.00 1.25 (0.87–1.79) 1.81 (1.31–2.51) 2.33 (1.68–3.22) <0.001
MS 1.00 1.32 (0.86–2.01) 2.92 (2.06–4.14) 4.41 (3.02–6.45) <0.001
Values are presented as odds ratio (95% confidence interval). Odds ratios are adjusted for sex, age, drinking, smoking.
hs-CRP, high-sensitivity C-reactive protein; WC, waist circumference; TG, triglyceride; HDL-C, high density lipoprotein-cholesterol; BP, blood pressure; FBS, fasting blood glucose; MS, metabolic syndrome.
*Obtained by logistic regression analysis.
Table 3. Mean of hs-CRP according to metabolic syndrome
Variables hs-CRP P-value*
WC
Low 0.79±0.02 <0.001
High 1.31±0.06
TG
Low 0.84±0.02 <0.001
High 1.13±0.04
HDL-C
High 0.79±0.02 <0.001
Low 1.25±0.05
BP
Low 0.91±0.02 <0.001
High 1.04±0.07
FBS
Low 0.88±0.02 <0.001
High 1.22±0.06
MS
≤2 0.86±0.02 <0.001
≥3 1.34±0.07
Values are presented as mean±standard deviation.
hs-CRP, high-sensitivity C-reactive protein; WC, waist circumference; TG, triglyc- eride; HDL-C, high density lipoprotein-cholesterol; BP, blood pressure; FBS, fast- ing blood glucose; MS, metabolic syndrome.
*Calculated by t-test.
Sung Kyum Kim, et al. The Relation of hs-CRP with Metabolic Syndrome in Korean Adults
Korean Journal of Family Practice
KJFP
본 연구는 단면연구라는 점에서 한계를 가지며 hs-CRP 수치에 영 향을 줄 수 있는 약물투약 및 고혈압, 당뇨, 이상지질혈증 치료 여부 와 신체활동 정도는 고려하지 못했다는 제한점이 있다. 또 대사증후 군의 유병률은 12.8%로 국내 타 연구4)에 비해 낮은 수치를 보였는데 진단기준 적용 시 투약 여부는 고려하지 않았기 때문으로 판단된다.
이번 연구는 우리나라 인구를 대표하는 통계조사를 분석하였다 는 장점을 가지며, 대사증후군과 hs-CRP의 연관성을 다시 한번 확인 하였다는 점에서 의미를 찾을 수 있다. 심혈관계 질환이 증가하는 현 실에서 대사증후군과 같은 전통적인 심혈관계 위험인자 보완을 위 해 위험도 평가의 일환으로 hs-CRP 선별검사의 유용성에 대한 연구 가 필요할 것으로 생각된다.
요 약
연구배경:
대사증후군은 심혈관 질환 및 제 2형 당뇨병의 위험을 증 가시키는 여러 가지 대사 이상 질환의 집합체이다. hs-CRP는 전신 염 증의 표지자이며 심혈관계 질환과의 관련성이 최근 강조되었다. 본 연구는 대사증후군과 hs-CRP의 관계를 규명함으로써 hs-CRP의 임 상적 의미에 대해 알아 보고자 하였다.방법:
본 연구는 국민건강영양조사 제6기 3차(2015년) 원시자료를 활용하여 만 19세 이상 80세 미만의 성인 3,705명을 대상으로 하였 다. hs-CRP는 사분위수로 나누어 분류 하였고 hs-CRP 수준에 따라 일반적 특성과 대사증후군 진단 기준 항목의 해당 비율을 확인하기 위해 카이제곱 검정을 이용하였다. hs-CRP 수준 별로 대사증후군 진단 기준 항목의 평균을 비교하기 위해 일원배치 분산분석을 이용 하였으며, 대사증후군 진단 기준 항목 해당 여부에 따른 hs-CRP 수 치의 평균을 비교하기 위해 독립표본 t-검정을 이용하였다. 그리고 hs-CRP 수준이 대사증후군 발생 가능성에 미치는 영향을 검증하기 위해 로지스틱 회귀분석을 이용하였다.결과:
hs-CRP이 높은 군일수록 적정 음주 비율은 낮아지고 남성, 50 대 이상, 현재 흡연, 대사증후군 비율이 높아지는 경향을 보였다. 대 사증후군의 진단 기준 항목인 허리 둘레(P<0.001), TG (P<0.001), HDL 콜레스테롤(P<0.001), 수축기 혈압(P<0.001), 이완기 혈압(P<0.001), 공 복혈당(P<0.001)이 hs-CRP와 관련이 있었다. 성별과 연령, 음주, 흡연 을 보정한 hs-CRP 수치에 따른 교차비는 (제 1사분위 대비 제 4사분 위) 복부둘레 4.99배(P<0.001), TG 2.88배(P<0.001), 낮은 HDL 콜레스 테롤 2.98배(P<0.001), 고혈압 1.93배(P<0.001), 고혈당 2.33배(P<0.001), 대사증후군 4.41배(P<0.001)로 높게 나타나 hs-CRP 수치가 높아질수 록 대사증후군 가능성이 높아지는 것으로 확인되었다.결론:
모든 대사증후군 진단 기준 항목이 hs-CRP 수준에 따라 유의한 차이를 보였으며 대사증후군에 해당되는 경우 hs-CRP 평균이 높 고 hs-CRP가 높은 군일수록 유의하게 대사증후군 비율이 높은 것 으로 나타났다.
중심단어:
국민건강영양조사; 대사증후군; 고감도 C-반응성 단백;한국 성인
REFERENCES
1. The Statistics Korea. Cause of death statistics in 2015. Daejeon: Statistics Korea; 2015.
2. Isomaa B, Almgren P, Tuomi T, Forsén B, Lahti K, Nissén M, et al. Cardiovas- cular morbidity and mortality associated with the metalobic syndrome. Di- abetes Care 2001; 24; 683-9.
3. Lakka H, Laaksonen DE, Lakka TA, Niskanen LK, Kumpusalo E, Tuomileh- to J, et al. The metabolic syndrome and total and cardiovascular disease mortality in middle-aged men. JAMA 2001; 288: 2709-16.
4. Lim S, Shin H, Song JH, Kwak SH, Kang SM, Won Yoon J, et al. Increasing prevalence of metabolic syndrome in Korea: the Korean national health and nutrition examination survey for 1998-2007. Diabetes Care 2011; 34: 1323- 8.
5. Haverkate F, Thompson SG, Pyke SD, Gallimore JR, Pepys MB. Production of C-reactive protein and risk of coronary eventsin stable and unstable an- gina: European concerted action on thrombosis and disabilities angina pec- toris study group. Lancet 1997; 349: 462-6.
6. Koenig W, Sund M, Fröhlich M, Fischer HG, Löwel H, Döring A, et al. C- Reactiveprotein, a sensitive marker of inflammation, predicts future risk of coronary heart disease in initially healthy middle-aged men: results from the MONICA (monitoring trends and determinants in cardiovascular dis- ease) Augsburg Cohort study, 1984 to 1992. Circulation 1999; 99: 237-42.
7. Rohde LE, Hennekens CH, Ridker PM. Survey of C-reactive protein and cardiovascular risk factors in apparently healthy men. Am J Cardiol 1999;
84: 1018-22.
8. Ridker PM, Buring JE, Cook NR, Rifai N. C-reactive protein, the metabolic syndrome, and risk of incident cardiovascular events: an 8-year follow-up of 14 719 initially healthy American women. Circulation 2003; 107: 391-7.
9. Ridker PM. High-sensitivity C-reactive protein: potential adjunct for global risk assessment in the primary prevention of cardiovascular disease. Circu- lation 2001; 103: 1813-8.
10. National Cholesterol Education Program (NCEP) Expert Panel on Detec- tion, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third report of the national cholesterol education program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III) final report.
Circulation 2002; 106: 3143-421.
11. Lee SY, Park HS, Kim DJ, Han JH, Kim SM, Cho GJ, et al. Appropriate waist circumference cutoff points for central obesity in Korean adults. Diabetes Res Clin Pract 2007; 75: 72-80.
12. Sattar N, Gaw A, Scherbakova O, Ford I, O’Reilly DS, Haffner SM, et al. Met- abolic syndrome with and without C-reactive protein as a predictor of coro- nary heart disease and diabetes in the West of Scotland coronary prevention
김성겸 외. 성인에서 hs-CRP와 대사증후군과의 연관성 Korean Journal of Family Practice
KJFP
study. Circulation 2003; 108: 414-9.
13. Rutter MK, Meigs JB, Sullivan LM, D’Agostino RB Sr, Wilson PW. C-reactive protein, the metabolic syndrome, and prediction of cardiovascular events in the Framingham Offspring study. Circulation 2004; 110: 380-5.
14. Mirhafez SR, Ebrahimi M, Saberi Karimian M, Avan A, Tayefi M, Heidari- Bakavoli A, et al. Serum high-sensitivity C-reactive protein as a biomarker in patients with metabolic syndrome: evidence-based study with 7284 sub- jects. Eur J Clin Nutr 2016; 70: 1298-304.
15. Kazemi-Bajestani SM, Tayefi M, Ebrahimi M, Heidari-Bakavoli AR, Moohebati M, Parizadeh SM, et al. The prevalence of metabolic syndrome increases with serum high sensitivity C-reactive protein concentration in individuals without a history of cardiovascular disease: a report from a large Persian cohort. Ann Clin Biochem 2017; 54: 644-8.
16. Bustos P, Rosas B, Román P, Villagrán J, Amigo H. [Association of C reactive
protein levels with metabolic syndrome in adults: a population-based study]. Rev Med Chil 2016; 144: 1239-46. Spanish.
17. Vidyasagar S, UK Razak A, Prashanth CK, Varma DM, Bairy KL. Highly sensitive C-reactive protein in metabolic syndrome. JIACM 2013; 14: 230-4 18. Kim YJ, Hwang SB, Kim SY, Hwang IH. The association between C-reactive
protein and features of the metabolic syndrome. Korean J Fam Med 2003;
24: 456-60.
19. Jung SB, Song YA, Chung DH, Choi BG, Oh JE, Cho CY, et al. The associa- tion between metabolic syndrome and high-sensitivity C-reactive protein.
Korean J Fam Pract 2016; 6: 367-70.
20. Park JS, Kim YJ, Lee JG, Kim YJ, Lee SY, Min HG. The role of C-reactive pro- teinas a inflammation-related factor in metabolic syndrome. Korean J Fam Med 2009; 30: 449-56.