Korean Journal of HBP Surgery
□ 증 례 □ Vol. 8, No. 3, September, 2004
195 BACKGROUND
Gastrointestinal stromal tumors (GISTs) may arise about anywhere in the tubular gastrointestinal tract, from the esophagus to the rectum. In addition, it has been discovered
in recent years that identical lesions may also occur in extra-gastrointestinal locations, principally the mesentery, om- entum and retroperioneum.1,2 The demonstration of CD 117 (KIT) expression in these lesions has helped validate their existence, particularly as they have been found in exceptional sites such as the gallbladder or bladder.3,4 However, only a few GISTs of the gallbladder have been described;5 therefore, we wish to contribute to the medical literature a rather unique case study having a rare location for malignant extra GIST, that of the gallbladder.
CASE PRESENTATION
A 68-year-old male patient was admitted to the department of surgery complaining of a right upper quadrant abdominal mass for 3 months. On admission, the patient was well nou- rished, and the physical examination showed that he had a nontender mass, 10 ×8 cm, that occupied the entire right upper quadrant. Laboratory findings were a hemoglobin level of 14.2 g/dl (normal: 13∼18 g/dl), white blood cell count of 6,700/mm3 (normal: 4,800∼10,800/mm3), and the liver blood tests were normal.
Contrast enhanced computed tomography revealed a severely distended gallbladder with an intraluminal enhancing polypoid portion (Fig. 1).
Upon laparotomy, a markedly enlarged gallbladder was observed. It was adhered to the omentum and neighboring transverse colon and it contained a sized 1.8 cm sized stone.
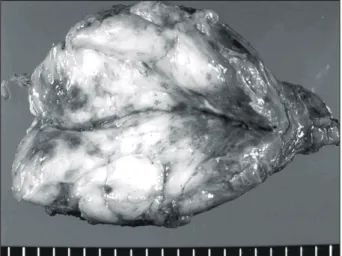
On gross examination, a firm, polypoid, 10×6 cm tumor protruded from the lumen of the gallbladder. On cross section, the tumor was fleshy yellow with patchy areas of hemorrhage and necrosis (Fig. 2). The wall of the gallbladder appeared unremarkable. Histologically, spindle to round shaped tumor cells were arranged in long and short fascicles. The nuclei of the tumor cells were hyperchromatic with inconspicuous nucleoli, and the cytoplasm appeared eosinophilic or vacuolated (Fig. 3). Myxoid hypocellular areas were interspersed with dense cellular areas, and extensive necrosis was noted. There
담낭에서 발생한 악성 Gastrointestinal Stromal Tumor
전북대학교 의과대학 외과학교실, 1병리학교실 및 2내과학교실
김찬영․장규윤1․김인희2․조백환
Malignant Extragastrointestinal Stromal Tumor of the Gallbladder
Chan Young Kim, M.D, Kyu Yun Jang, M.D1, In Hee Kim, M.D2 and Baik Hwan Cho, M.D.
Departments of Surgery, 1Pathology, and 2Internal Medicine, Chonbuk National University College of Medicine, Chonju, Korea The demonstration of CD 117 (KIT) expression in extragastro- intestinal lesions has helped to validate extra-gastrointestinal stromal tumors. We report here on an exceedingly rare case of a malignant extragastrointestinal stromal tumor of the gallb- ladder. A 68-year-old male patient presented with a palpable and nontender mass occupying the entire right upper quad- rant of his abdomen. The patient underwent open cholecys- tectomy. On gross examination, a firm, polypoid, 10×6 cm tumor protruded from the lumen of the gallbladder. Histo- logically, there were 88 mitotic figures per 10 high-power fields. The tumor cells were immunoreactive for CD 117, vimentin and CD 34. Immunostaining for CD 117 showed a dot-like staining pattern in about 20% of the tumor cell. The present case was an exceedingly rare entity occurring in the gallbladder, Currently, the patient is under follow-up for 6 months with no abnormal findings such as recurrence.
(Korean J HBP Surg 2004;8:195-197)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Key Words: Gastrointestinal Neoplasm
Gallbladder
중심 단어: 담낭암, 간질종양
책임저자:조백환, 전북 전주시 덕진구 금암동 634-18 ꂕ 561-712, 전북대학교 의과대학 외과학교실 Tel: 063-250-1570 Fax: 063-271-6197 E-mail: [email protected]
196 한국간담췌외과학회지:제 8 권 제 3 호 2004
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
were 88 mitotic figures per 10 high-power fields, and atypical mitosis was noted. The tumor had invaded the proper muscle layers, but not serosa of the gallbladder.
The tumor cells were immunoreactive for CD 117, vimentin and CD 34. Immunostaining for CD117 showed a dot-like staining pattern in about 20% of tumor cells (Fig. 4). Immunos- taining for desmin showed focal positivity. There was negative staining for cytokeratin, S-100 protein, smooth muscle actin and myoglobin. There were no CD 117-positive cells in the uninvolved gallbladder wall.
DISCUSSION
The discovery of gain-of-function mutations in the KIT proto-oncogene of GIST by Hirota and colleagues6 in 1998 was crucially importance in terms of the genesis and classification of these tumors. At present, the expression of KIT protein has emerged as the tumors' most important defining feature, and it is probably the gold standard for diagnosing GISTs.7,8 For that reason, the demonstration of KIT expression in extra- gastrointestinal lesions has helped validate their existence, and particularly when finding these tumors in exceptional sites such as the gallbladder or bladder.3,4
Fig. 1. Abdomen CT scan. Contrast enhanced computed tomography reveals the severely distended gallbladder with the intralu- minal, enhancing polypoid portion.
Fig. 2. Section of fresh gross specimen. The tumor filled the lumen of the gallbladder. The cut surface is fleshy and yellow with patch areas of hemorrhage and necrosis.
Fig. 4. Immunohistochemical staining tumor cells show dot-like cytoplasmic reactivity for CD 117 (×400).
Fig. 3. Histologic finding (H&E, ×400). Spindle shaped tumor cells with nuclear pleomorphism and mitotic features.
김찬영:담낭에서 발생한 악성 Gastrointestinal Stromal Tumor: 증례 보고 197 ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Usually, most GISTs show unequivocal diffuse, strong
cytoplasmic positive immunostaining for CD 117 (KIT). But occasional, there are cases showing only the dot-like staining pattern in as few as 5% to 20% of the tumor cells.8 Our case likewise showed the dot-like immunostaining pattern for CD 117 in about 20% of tumor cells.
Aside from the consistent positivity for CD 117, 60% to 70%, 30% to 40%, 5%, and 1% to 2% of GISTs show immuno- reactivity for CD 34, smooth muscle actin, S-100 protein and desmin, respectively.8 But the immunophenotype of true CD 117-positive GISTs varies to some degree with their location.
The previously reported malignant stromal tumor of the gallbladder showed immunoreactivity for CD 117 and vimentin, but cytokeratin, desmin, and myoglobin were negative.9 Our case displayed immunoreactivity for CD 117, vimentin, CD 34, and desmin.
Histologically, our case should be distinguished from primary or metastatic undifferentiated carcinoma, sarcomatoid carcinoma, leiomyosarcoma, rhabdomyosarcoma, and metastatic melanoma.
However, these tumors can excluded by the immunohisto- chemical findings. Undifferentiated carcinoma or sarcomatoid carcinomas show immunoreactivity for cytokeratin. A leiomyo- sarcoma would express smooth muscle actin and desmin, and likewise a rhabdomyosarcoma would express desmin and myoglobin. Moreover, these tumors are all negative for CD 117 immunostaining. Some malignant melanomas can express CD 117, but the S-100 protein and HMB-45 immunostaining would be positive.9
To distinguish between benign and malignant GISTs, many parameters have been proposed, but tumor size and the mitotic rate have been widely used as histologic criteria. Fletcher et al. have recently proposed criteria to separate benign from malignant tumors by tumor size and the mitotic count.5 By this definition, the tumor larger than 10 cm or having more than 10 mitosis per 50 high power fields belong to the high risk category. In this respect our case belongs to the high risk category. Moreover our case showed extensive necrosis, high cellularity and nuclear pleomorphism. Therefore, it was predicted that the prognosis for our patient would be poor.
Complete excision has been accepted as the only and efficacious treatment regimen for nonmetastatic GISTs. However, with the recent discovery that the gain-of-function mutation of the c-kit proto-oncogene is an etiologic factor for GIST, many
studies have reported that imatinib mesylate inhibiting kit receptor tyrosine kinase is an efficacious agent for patients with malignant, metastatic and/or unresectable GIST. Currently, imatinib mesylate is widely used as neoadjuvant or adjuvant therapy.9
In conclusion, our present case was an exceedingly rare entity occurring in the gallbladder, and it was characterized by a right upper quadrant abdominal mass that was palpable and nontender, and the patient underwent cholecystectomy. The present case will be under follow-up to monitor the future clinical outcome.
REFERENCES
1) Miettinen M, Sobin LH, Sarlomo-Rikala M. Immunohisto- chemical spectrum of GISTs at different sites and their differential diagnosis with a reference to CD 117 (KIT). Mod Pathol 2000;13:1134-1142.
2) Reith JD, Goldblum JR, Lyles RH, Weiss SW. Extra- gastrointestinal (soft tissue) stromal tumors: an analysis of 48 cases with emphasis on histologic predictors of outcome. Mod Pathol 2000;13:577-585.
3) Ortiz-Hidalgo C, de Leon Bojorge B, Albores-Saavedra J.
Stromal tumor of the gallbladder with phenotype of interstitial cells of Cajal. A previously unrecognized neoplasm. Am J Surg Pathol 2000;24:1420-1423.
4) Lasota J, Carlson JA, Miettinen M. Spindle cell tumor of urinary bladder serosa with phenotypic and genotypic features of gastrointestinal stromal tumor. Arch Pathol Lab Med 2000;124:894-897.
5) Mendoza-Marin M, Hoang MP, Albores-Saavedra J. Malignant stromal tumor of the gallbladder with interstitial cells of Cajal phenotype. Arch Pathol Lab Med 2002;126:481-483.
6) Hirota S, Isozaki K, Moriyama Y, et al. Gain-of-function muta- tions of c-kit in human gastrointestinal stromal tumors. Science 1998;279:577-580.
7) Miettinen M, Lasota J. Gastrointestinal stromal tumors-definition, clinical, histological, immunohistochemical, and molecular genetic features and differential diagnosis. Virchows Arch 2001;438:1-12.
8) Fletcher CD, Berman JJ, Corless C, et al. Diagnosis of gastro- intestinal stromal tumors: a consensus approach. Hum Pathol 2002;33:459-465.
9) Dernatteo RP, Hinrich MC, El-Rifai WM, Demetri G. Clinical management of gastrointestinal tumor: before and after STI- 571. Hum Pathol 2002;33:466-477.