161
서 론
GIST (gastrointestinal stromal tumor)는 식도, 위, 소장, 대 장, 직장에 생기는 비상피성 종양으로, 이전에는 평활근에 서 기원하는 평활근종, 평활근육종 등과 혼용되어 불려졌 으나 최근 Miettinen 등(1)은 GIST가 CD34에 양성반응을 보 이며 염색체 14번 장완의 손실과 c-kit 돌연변이에 의해 평 활근육종과 구분된다고 발표하여 현재 연구가 많이 진행되 고 있다.
GIST는 전체 위장관 종양의 약 1%를 차지하는 매우 드문 질환으로 대부분 위와 소장에 발생하는 하는 반면 대장과 직장에서의 발생은 드물며(2) 호발연령은 50대에서 60대이 며 40세 이전에는 매우 드물게 보고되고 있다.
저자들은 12세 소아에서 직장에 생긴 GIST 1예를 경험하 여 문헌고찰과 더불어 보고하는 바이다.
증 례
12세 남자 환자가 내원 10일 전부터 시작된 항문출혈을 주소로 개인병원에 내원하여 시행한 대장내시경 검사에서 직장내 종괴가 의심되어 본원으로 전원되었다. 출생력을 포함한 과거력과 가족력에 특이 소견이 없었으며 내원 당 일 신체 검사상 생명지수는 정상 소견이었다. 이학적 검사 상 복부는 정상이었고 직장수지검사에서 항문연으로부터 5 cm 상방 좌측 측면에 표면이 부드러운 점막으로 덮인 종 괴의 변연이 만져졌으며 출혈 양상을 띠었다. 검사실 소견상 말초 혈액 검사에서 혈색소 9.7 g/dL, 헤마토크리트 29.4%로 경미한 빈혈 소견을 보였으나 혈청 검사와 암태성 항원은 정상이었다.
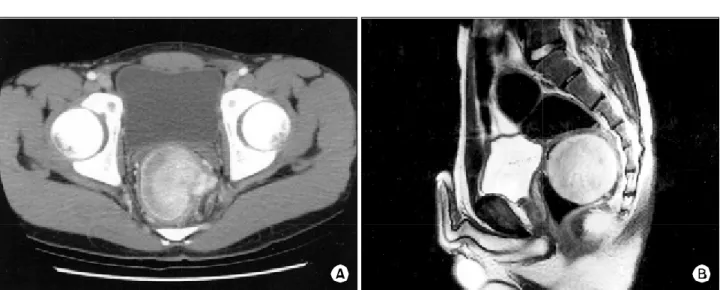
입원 당시 복부 전산화 단층 촬영에서 직장의 좌측 측면 점막하에서 기원하는 6×5.8 cm 크기의 두개의 엽으로 구 성된 연조직 종양이 항문연으로부터 5 cm 상부에서 관찰되 었으며 주위에 커져있는 림프절은 없었다(Fig. 1A). 주위 구 조물과의 관계를 알기 위해 시행한 골반 자기공명 사진에 서 복부 전산화단층 촬영과 같은 소견으로 주위 구조물로 의 침범소견은 보이지 않았으며 다른 기관으로 전이된 소 견도 없었다(Fig. 1B).
소아의 직장 위장관 간질종양
인하대학교 의과대학 외과학교실
윤민영․최선근․허윤석․이건영․김세중․조영업․안승익․홍기천․신석환․김경래․우제홍
Gastrointestinal Stromal Tumor of the Rectum in a Pediatric
Min Young Yun, M.D., Sun Keun Choi, M.D., Yun Suk Hur, M.D., Kun Young Lee, M.D., Sei Joong Kim, M.D., Young Up Cho, M.D., Seung Ick Ahn, M.D., Kee Chun Hong, M.D., Suk Hwan Shin, M.D., Kyung Rae Kim, M.D.
and Ze Hong Woo, M.D.
Gastrointestinal stromal tumors are the most common subset of mesenchymal tumors that arise from the gastrointestinal tract. They most commonly arise in the stomach, followed by the small bowel and, rarely, the rectum, esophagus and colon. Gastrointestinal stromal tumors and the specific c-kit protein (CD117)-positive mesenchymal tumors, have been sporadically reported in the rectum. We report here on a 12-year-old boy who underwent low anterior resection of huge gastrointestinal stromal tumor of the rectum. The diagnosis was confirmed by immunohistochemical staining of the tumor. The specimen was revealed to be a polypoid fungating tumor that, measured 6.0×6.0 cm in size, which consisted histologically of spindle-shaped cells. The tumor cells were positive for c-kit, vimentin, S-100, desmin, and SMA, although the results of the CD34 test were negative.
In general, Gastrointestinal stromal tumors of the rectum predominantly occur between the sixth and seventh decades and they are rarely seen in individuals less than 40 years of age. To the best of our knowledge, our case is the youngest reported patient in the English literature who had as gastrointestinal stromal tumor of the rectum. (J Korean Surg Soc 2006;71:161-165)
Key Words: Gastrointestinal stromal tumor (GIST), Rec- tum, Pediatric patient
중심 단어: 위장관 간질 종양, 직장, 소아
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Department of Surgery, Inha University College of Medicine, Incheon, Korea
책임저자:우제홍, 인천시 중구 신흥동 3가 7-206 ꂕ 400-013, 인하대학교병원 외과 Tel: 032-890-3143, Fax: 032-890-3097 E-maill: [email protected]
접수일:2005년 12월 30일, 게재승인일:2006년 2월 20일
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
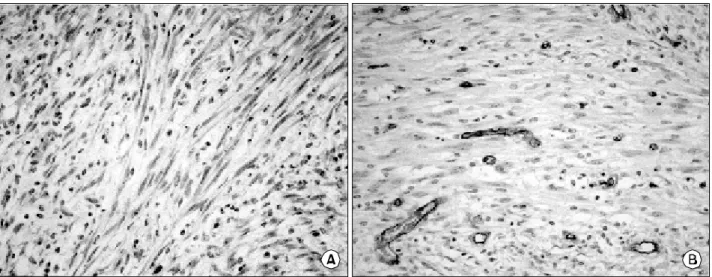
환자는 직장의 GIST 혹은 횡문근종양 진단하에 저위전방 절제술 및 횡행결장루를 시행 받았다. 개복시 복강 내에는 특이 소견이 없었으며 다른 기관도 정상소견이었다. 종양 은 복막반전 아래의 좌측 하부 직장벽에 있었으며 주위 구 조물로의 침습소견은 없었다. 육안적 소견으로 부분적 궤 양을 동반한 점막으로 덮인 6×6 cm 크기의 점막하 종양이 관찰되었다(Fig. 2A). 종양의 절단면은 점막과의 구분이 명 확하고 회백색의 탄력적인 연조직으로 구성되어 있으며 출 혈과 괴사는 관찰되지 않았다(Fig. 2B). 조직학적 소견에서 종양은 높은 세포의 밀집을 보였으며 과형성된 방추형세포 (Fig. 3A)와 유사분열(Fig. 3B)이 관찰되었다. 유사분열의 수 는 50개의 400배 시야당 평균 6개가 관찰되었다. 장간막 림 프절로의 전이는 없었다. 면역화학조직검사에서 c-kit에는
양성반응을 보였으나(Fig. 4A) CD34 에는 음성반응을 보였 다(Fig. 4B). 위의 조직학과 면역화학조직학적 소견으로 직 장의 GIST로 진단하였으며 환자 수술 후 19개월 동안 재발 과 전이 소견 보이지 않고 현재 외래 추적관찰 중이다.
고 찰
GIST는 c-kit (CD117)에 양성반응을 보이는 방추형세포 또는 상피형세포로 구성된 위장관 간엽 종양으로 정의할 수 있다. 이와 같은 정의에 의해 GIST는 이전에 혼용되어 사용되었던 평활근 종양 및 쉬반종과 분리되어 위장관 간 엽종양 중 가장 많은 빈도를 차지하고 있다.(1,3,4) GIST는 위장관의 Cajal 간질세포(interstitial cell of Cajal, Fig. 1. (A) Axial CT scan shows a heterogeneous mildly contrast-enhancing soft tissue mass. (B) MRI clearly demonstrated a well defined
oval mass arising from the submucosa layer of the left anterolateral rectal wall.
Fig. 2. (A) A gross finding showing a submucosal tumor with mucosal uleration, measuring 6×6×5.8 cm size, located lower rectum. (B) The cut surface of the tumor was uniformly elastic soft, greyish without hemorrhage or necrosis.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
ICC) 또는 Cajal세포나 평활근세포로 분화되는 원시세포에 서 기원하여 위장관 전체에서 발생할 수 있는 점막하 간엽 종양이나 위(65%)와 소장(30∼35%)에서 대부분이 발생하 며 직장, 식도, 대장에서는 매우 드물다. 또한 직장 GIST의 호발연령은 50대에서 60대이며 40세 이전에는 드물고(1) 특 히 소아에서 극히 드문 질환으로 알려져 있다.(5-7) 소아에서의 GIST는 산발적, 가족성 또는 Carney 삼징후 (GIST, 폐 연골종, 부신외의 부신경절종)의 형태로 나타나 는데 대부분은 산발적으로 나타나고 젊은 여성에서 호발하 는 Carney의 삼징후로 나타나는 경우는 드물다고 한다.(8) 소아 GIST도 성인과 같이 위에서 가장 많이 발생하며 소장, 대장, 직장과 식도 등에서는 드물다. 따라서 대부분의 소아 GIST 환자의 주요증상으로 비특이적인 복통과 종괴로 병
원에 내원한다.(6,7) 성별에 있어 성인 GIST는 남녀 같은 분 포를 나타내나(1-4,9) 소아에서는 여아가 대부분을 차지한 다.(5-7) 최근 Cypriano 등(6)은1986년부터 2002년까지 발표 된 소아 GIST 16 증례를 모아 발표하였는데 이 중 11예가 위에서 발생하였으며 소장 3예, 대장 2예의 분포를 보였고 여아 12예, 남아 4예로 나타났다. 본 증례는 직장 GIST로서 가장 어린 나이에 발생한 경우라고 생각한다.
성인 GIST는 15∼50%에서 발견 당시 전이가 되어 있으 며 가장 많은 전이 부위는 복강 내와 간으로 알려져 있다.
그러나 림프선 전이는 매우 드물다.(9,10) Cypriano 등이 발 표한 16예에서는 3예가 간이나 복강 내로 전이된 양상을 보 여 성인과 비슷함을 알 수 있다. 본 증례의 경우 원격전이와 림프절 전이 모두 없었다.
Fig. 3. (A) Hematoxylin and erosin staining of the tumor showed facicular and interlacing proliferation of spindle-shaped cell and (B) mitosis (H&E stain, ×400).
Fig. 4. (A) The tumor cell are diffuse positive staining for c-kit protein but (B) negative staining for CD34 (immunohistochemical stain,
×400).
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 면역조직화학 검사적으로 GIST는 c-kit protein (CD117)에
대하여 특이적 양성반응을 보여 c-kit protein은 GIST 진단의 가장 중요한 면역조직화학 검사 표지이다. 각각 CD34 (the haematopoietic progenitor cell antigen) (70%), SMA (smooth muscle actine)(20∼30%), desmin (<5%), S-100 protein (10%) 로 나타난다.(1,9) Wang 등(10)은 CD34의 양성률이 70%에 미치는 이유를 다음과 같이 설명하고 있다. CD34에 양성인 GIST는 c-kit양성인 GIST과 구분되며 CD34와 c-kit에 모두 양성인 GIST가 점차 CD34에 음성과 c-kit에 양성인 GIST로 변한다고 발표하였다. 그러나 이는 GIST의 세포의 변이를 나타내나 임상양상 또는 예후에 큰 영향을 미치지 않는다 고 한다. 본 증례의 경우 c-kit 양성, CD34에 음성을 보였다.
성인 GIST의 대부분에서 나타나는 염색체 이상은 14번 과 22번의 단배체(monosomy)이다. GIST의 가장 중요한 유 전자 돌연변이는 KIT 유전자의 엑손 11의 돌연변이이며 그 밖에 드물게 엑손 9와 13의 돌연변이를 나타내는 경우도 있 다.(6,11) 그러나 소아의 경우 엑손 9, 11, 13 모두에서 돌연 변이가 있지 않으며 어떤 유전자 돌연변이도 관찰되지 않 는다고 한다.(5,6,12) Li 등(5)이 발표한 논문에서 성인과 달 리 소아의 GIST는 다른 분자적 단계를 거쳐 악성으로 변할 것이라 가정한다고 발표했지만 현재까지 증명된 근거는 없다.
GIST의 치료는 외과적 완전 절제이다. 직장 GIST는 직장 상부, 중부, 하부의 발현 빈도 차이가 없으나 Khalifa 등(13) 은 국소 절제 후의 재발률을 예방하기 위해 크기가 클 경우 복회음절제술을 시행할 것을 권유하였다. Aparicio 등(14)은 수술 방법이 전체 예후나 생존율에 영향을 미치지 않으나 현미경적으로 절제면이 음성이어도 종양 절제만을 시행하 였을 경우 국소재발이 잘 일어나므로 쐐기형 절제 또는 경 항문절제는 피하고 분절절제를 권유하고 있다. 그러나 소 아의 경우 복회음 절제술은 생활의 질이 감소하므로 본 증 례에서는 현미경적으로 하부 절제면 2 cm를 포함한 저위전 방절제술과 횡행 결장루를 시행하였으며 술 후 3개월에 횡 행루 복원술을 시행하였다.
GIST의 악성여부를 예측하기는 어렵다. 현재 악성여부 진단에 가장 많이 받아들여지는 기준은 종양의 크기와 유 사분열 수이다. 많은 논문에서 두 요인이 악성여부를 예측 할 수 있으며 크기가 5 cm 이상일 경우와 유사분열 수 5/50 HFP 이상일 경우 재발 및 복강내 전이와 간 전이가 일어날 가능성이 높다고 하였다.(1)아직 소아의 악성기준이 따로 정립되어 있지 않아 위의 기준에 의해 분리되고 있다. 크기 가 크거나 유사분열 수가 많을 경우 근치적 절제 및 항암제 등의 추가 치료와 지속적인 추적관찰이 필요하다. 이는 전 체 위장관 GIST의 특성이나 직장 GIST의 경우 근위부에 해 당하는 위, 소장 GIST보다 예후가 더 좋지 않아 더 유의해 야 하겠다. 본 증례의 경우 크기 5 cm이었으며 유사분열 6/50 HFP으로 악성에 해당된다. 현재 19개월 추적기간 동안 재발이 없었으나 짧은 추적관찰 기간으로 재발 여부 판단
이 어렵다. 그 밖의 조직학적 예후인자로 종양의 출혈, 괴 사, 세포 밀집도 등이 있다.
GIST의 전이는 직접적 침습 또는 혈액성전이가 많은 반 면 림프절과 폐전이는 드물다. 또한 GIST의 재발은 특이하 게 단독적으로 복강에서 일어난다. 가장 많은 재발 양상은 직접 침습에 의한 복강내 파종과 간문맥을 통한 혈액성 파 종이다.(15,16)GIST는 재발한 경우의 40%가 2차적 완전절 제가 가능하다. Mudan 등(16)은 수술 후 15개월 이상의 생 존기간을 가진 경우의 1/3만이 재발 후에 완전절제가 가능 하였으며 재발된 경우 완전절제 여부를 결정하는 주된 요 인은 1차 수술 후 재발까지의 무병 생존 기간이라 하였다.
일반적으로 근치적으로 절제된 직장 GIST는 추가적인 항암치료와 방사선 치료가 필요 없다. 그러나 절제 불가능 하거나 전이된 GIST는 치명적이며 보조적인 항암치료에도 치료되지 않는다. 전이된 GIST 환자의 중앙 생존율은 20개 월 정도이며 국소재발 환자의 생존율은 약 9∼12개월이다.
최근에는 전이 또는 절제 불가능한 GIST 치료에 Imatinib mesylate가 사용하고 있으며 Demertri 등(16,17)은 Imatinib mesylate가 전이 또는 재발된 GIST 환자의 50% 이상에서 치료적 반응을 보이고 있다고 발표하였다. 그러나 완전 관 해는 극히 드물어 초기 치료로 적당하지 않다. 직장 GIST의 치료적 원칙은 외과적 절제 후 보조적으로 치료하는 것이 적당하며 Imanitib의 투여 적응증은 크기가 크거나 C-kit 양 성 또는 재발 혹은 전이된 환자이다.
소아의 GIST는 드물며 특히 소아 직장 GIST는 극히 드물 다. 저자들은 12세의 소아에서 직장의 악성 GIST를 진단하 여 외과적 절제술을 시행하였던 1예를 경험하였기에 문헌 고찰과 함께 보고하는 바이다.
REFERENCES
1) Miettinen M, Lasota J. Gastointestinal stromal tumors-defini- tion, clinical, immunohistochemical, and molecular genetic feature and differential diagnosis. Virchows Arch 2001;438:
1-12.
2) Miettinen M, Sarlomo-Rikala M, Lasota J. Gastrointestinal stromal tumors. Ann Chir Gynecol 1998;87:278-81.
3) Kindblom L, Remotti HE, Aldenborg F, Meis-Kindblom JM.
Gastrointestinal pacemaker cell tumor (GIPACT): gastrointes- tinal stromal tumors show phenotypic characteristics of the intestinal cells of Cajal. Am J Pathol 1998;152:1259-69.
4) Sarlomo-Rikala M, Kovatich AJ, Barusevicius A, Miettinen M.
CD 117: a sensitive maker for gastrointestinal stromal tumors that is more specific than CD34. Mod Pathol 1998;11:728-34.
5) Li P, Wei J, A. West AB, Perle M, Greco MA, Yang GC.
Epitheloid gastrointestinal stromal tumor of the stomach with liver metastasis in a 12-year-old girl: aspiration cytology and molecular study. Pedia Dev Pathol 2002;5:386-94.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 6) Cypriano MS, Jenkins JJ, Pappo AS, Rao BN, Daw NC.
Pediatric gastrointestinal stromal tumors and leiomyosarcoma.
Cancer 2004;101:39-50.
7) Prakash S, Sarron L, Socci N, DeMatteo RP, Eisenstat J, Grego AM, et al. Gastrointestinal stromal tumor in children and young adults. J Pediatr Hematol Oncol 2005;27:179-87.
8) Perez-Atayde AR, Shamberger RC, Kozakewich HW. Leuroec- todermal differntiation of gastrointestinal tumors on the Carney triad. An ultrastructural and immunohistochemical study. Am J Surg Pathol 1993;17:706-14.
9) Miettinen M, Lasota J. Gastrointestinal stromal tumors (GISTs):
definition, occurrence, pathology, differential diagnosis and molecular genetics. Pol J pathol 2003;54:3-24.
10) Wang L, Vargas H, French SW. Cellular origin of gastro- intestinal stromal tunors: a study of 27 cases. Arch Patholo Lab Med 2000;124:1471-5.
11) Ryu SW, Jeong CW, Hwang JH, Kim IH, Jeong HS, Kang YN, et al. Mutation analysis of genes related to gastrointes- tinal stromal tumors. J Korean Soc 2005;68:107-16.
12) Kerr JZ, Hicks MJ, Nuchtern JG, Saldivar V, Heim-Hall J, Shah S, et al. Gastrointestinal autonomic nerve tumors in the
pediatric population: a case report of four cases and a review of the literature. Cancer 1999;85:220-30.
13) Khalifa AA, Bong WL, Rao VK, Williams MJ. Leiomyosar- coma of the rectum. Report of a case and review of the litera- ture. Dis Colon Rectum 1986;29:427-32.
14) Aparicio T, Boige V, Sabourin J, Crenn P, Ducreux M, Le cesne A, et al. Prognostic factors after surgery of primary resectable gastrointestinal stromal tumors. Eur J Surg Oncol 2004;30:1098-103.
15) Demateo RP, Lewis J, Leung D, Mudan SS, Woodruff JM, Brennan MF. Two hundred gastrointestinal stromal tumors:
recurrence patterns and prognostic factors for survival. Ann Surg 2000;231:51-8.
16) Mudan SS, Conlon KC, Woodruff JM, Lewis JJ, Brennan MF.
Salvage surgery for patients with recurrent gastrointestinal sarcoma: prognostic factors to guide patient selection. Cancer 2000;88:66-74.
17) Demetri GD, von Meheren M, Blanke CD, Van den Abbeele, Eisenberg B, Roberts PJ, et al. Efficacy and safety of imanitib mesylate in advanced gastrointestinal stromal tumors. N Engl J Med 2002;347:472-80.