대한치과교정학회 임상저널
대한치과교정학회
Volume 9 Number 3 July·August·September 2019 Kao.or.kr/cjkao
편집이사
채 종 문 (원광대학교)
편집위원
배 기 선 (선부부치과) 최 동 순 (강릉대학교) 홍 미 희 (경북대학교) 안 효 원 (경희대학교) 이 상 민 (단국대학교) 김 성 식 (부산대학교) 임 원 희 (서울대학교) 최 성 환 (연세대학교) 장 나 영 (원광대학교)
이 미 영 (관악서울대학교치과병원)
이 경 민 (전남대학교) 이 승 엽 (전북대학교) 임 성 훈 (조선대학교)
Editorial Board
Editor
Jong-Moon Chae (Wonkwang University)
Editorial Board
Gi-Sun Bae (Sun Orthodontic Clinic)
Dong-Soon Choi (Gangneung-Wonju National University) Mihee Hong (Kyungpook National University)
Hyo-Won Ahn (Kyung Hee University) Sang-Min Lee (Dankook University) Seong-Sik Kim (Pusan National University) Won-Hee Lim (Seoul National University) Sung-Hwan Choi (Yonsei University) Na-young Chang (Wonkwang University)
Mi-Young Lee (Seoul National University Gwanak Dental Hospital) Kyung-Min Lee (Chonnam National University)
Seung-Youb Lee (Chonbuk National University) Sung-Hoon Lim (Chosun University)
2019년 7•8•9월호 ORIGINAL ARTICLE
A Questionnaire Study of the Motive and Effectiveness of Treatment in Patients Treated with 2-Jaw Surgery
Seung-Yeon Lee, Sung-Seo Mo ··· 127
CASE REPORT
성장기 때 절충교정치료 경험이 있는 골격성 III급 부정교합 환자의 수술 교정 치험례
경효정, 이예슬, 박기호 ··· 138
전방부 분절골절단술로 인한 의원성 외상 치아의 교정적 이동
홍석윤, 김영호, 채화성 ··· 151
Low-Profile 맞춤형 교정장치를 이용한 교정치료
정서린, 임성훈 ··· 165
Combination Surgery (USSRO + UIVRO)를 이용한 비대칭을 동반한 골격성 III급 부정교합의 악교정수술 치험례
이상훈, 정동화, 차경석, 이진우, 이상민 ··· 178
상악 전치의 치체 이동과 압하 이동이 필요한 돌출입 증례에서 Antero-Posterior Lingual Retractor와 투명교정장치를 이용한 치료
강승구, Dafeng Qu, 권순용 ··· 189
SPECIAL ARTICLE - Digital Orthodontics-Part 1
디지털 교정의 이해: 실효성과 한계
김윤지, 김명수, 이동렬 ··· 202
투고안내 ··· 217
132 Questionnaire study;
2-jaw surgery
140 Orthosurgery after camouflage treatment
183 Virtual combination surgery
191 APLR (Antero-Posterior Lingual Retractor)
156 Iatrogenic trauma by ASO
171 Customized brackets and transfer jigs
206 Digital setup and
July•August•September, 2019 ORIGINAL ARTICLE
A Questionnaire Study of the Motive and Effectiveness of Treatment in Patients Treated with 2-Jaw Surgery
Seung-Yeon Lee, Sung-Seo Mo ··· 127
CASE REPORT
Surgical Orthodontic Treatment of Hyperdivergent Skeletal Class III Malocclusion Patient Experienced in Camouflaging Orthodontic Treatment: Case Report
Hyo-Jung Kyung, Ye-Seul Lee, Ki-Ho Park ··· 138
A Case Report: Orthodontic Treatment of Iatrogenic Trauma Teeth Caused by Anterior Segmental Osteotomy
Seok Yoon Hong, Young Ho Kim, Hwa Sung Chae ··· 151
Orthodontic Treatment Using Low-Profile Customized Orthodontic Brackets
Seo-Rin Jeong, Sung-Hoon Lim ··· 165
Orthognathic Treatment Using Combination Surgery (Unilateral Sagittal Ramus Osteotomy and Unilateral Intraoral Vertical Ramus Osteotomy) for Skeletal Class III Malocclusion Patient with Facial Asymmetry
Sang-Hoon Lee, Dong-Hwa Chung, Kyung-Suk Cha,
Jin-Woo Lee, Sang-Min Lee ··· 178
The Treatment of Lip Protrusion Which Demands Intrusion and Bodily Movement of Upper Anterior Tooth with Antero-Posterior Lingual Retractor Combined with Clear-Aligner
Seung Gu Kwon, Dafeng Qu, Soon Yong Kwon ··· 189
SPECIAL ARTICLE - Digital Orthodontics-Part 1
Clinical Effectiveness and Limitations of Digital Orthodontic Appliances
Yoon-Ji Kim, Myung-Su Kim, Dong-Yul Lee ··· 202
Information for Authors ··· 217
132 Questionnaire study;
2-jaw surgery
140 Orthosurgery after camouflage treatment
183 Virtual combination surgery
191 APLR (Antero-Posterior Lingual Retractor)
156 Iatrogenic trauma by ASO
171 Customized brackets and transfer jigs
206 Digital setup and
Dr. 모 성 서 Dr. 이 승 연
Corresponding author: Sung-Seo Mo Division of Orthodontics, Department of Dentistry, Yeouido St. Mary’s Hospital, College of Medicine,
The Catholic University of Korea, 10 63-ro, Yeongdeungpo-gu, Seoul 07345, Korea Tel: +82-2-3779-1319 E-mail: [email protected] Received: July 16, 2019 / Revised: August 12, 2019 / Accepted: August 13, 2019
ABSTRACT
Objective: To identify the effect of orthognathic surgery on patients’ self-esteem, effects of surgery, motivations, and perception of treatment methods. Methods: A survey was conducted in patients who received orthognathic surgery and orthodontic treatment, and the results of the survey were analyzed using the SAS System for Windows V 9.3 program.
Results: Of the 208 respondents (83 men, 125 women), the majority of patients selected overcoming inferiority complexes and recovering self-confidence as motivations and improvements after the surgery. The improvements in self-esteem and masticatory function after orthognathic surgery were statistically significant. More than half of the respondents answered that the possibility of post-surgical effects was the factor they were most worried about before surgery. Moreover, the number of patients that felt change in pronunciation after surgery was 1.5 times more than those that did not. As for treatment methods, the majority preferred a surgery-first approach, and regarding considerations, most answered that choosing between surgery-first/orthodontic correction-first was not a decisive factor. Conclusion:
The results could be used as a reference to explain treatment plans to patients requiring surgery. Subsequent studies about several variables related to the psychological effects caused by 2-jaw surgery are required. (Clin J Korean Assoc Orthod 2019;9(3):127-137)
Key words Orthognathic surgery, Motive
A Questionnaire Study of the Motive and Effectiveness of Treatment in Patients Treated with 2-Jaw Surgery
Seung-Yeon Lee,1 Sung-Seo Mo2
1Private Clinic, Seoul, Korea
2Division of Orthodontics, Department of Dentistry, Yeouido St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
INTRODUCTION
There has been a large increase of patients with malocclusion caused by skeletal disharmony of the upper and lower jaw, seeking orthognathic sur- gery or orthodontic treatment for functional and esthetic problems. Not only has the actual number of patients receiving surgery increased, the 2-jaw surgery has drawn people’s interest through the media such as television and the internet. There- fore, we planned this study on 2-jaw surgery.
The benefits of orthognathic surgery include improvements in masticatory function by correc- tion of malocclusion, and esthetic improvements through the balanced alignment of previously over- or under-developed upper and lower jaws.1 Moreover, the improvements in physical appear- ance and chewing can provide psychological satis- faction to the patient.2
The aim of our study was to investigate the ef- fects of surgical treatment on patients’ self-es- teem. The study subjects were patients that received 2-jaw orthognathic surgery. We also ana- lyzed the differences between the patient’s expec- tation before surgery and the actual post-surgical results (functional improvement and esthetic im- provement). Finally, we studied and contemplated various sociological and psychological aspects of the 2-jaw surgery using a questionnaire. The ques- tions included patient’s motives for 2-jaw surgery, their greatest worries prior to surgery, whether they would recommend the surgery to others, their awareness of surgical methods, such as ‘surgery first’ and ‘orthodontics first’ methods, and the fac- tors that influenced their decision to get the sur- gery. The null hypothesis of this study was that there is no difference in aesthetics, self-esteem, and chewing function before and after surgery for jaw surgery.
MATERIALS AND METHODS
Our survey was conducted in patients hospital- ized at a local dental clinic located in Gangnam- gu, Seoul between October 2014 and February 2015. We did not put out notices or recruit par- ticipants separately; at the hospital where the re- searcher worked, he/she handed out question- naires to patients who had spontaneously visited the hospital, undergone 2-jaw surgery, completed all postoperative orthodontic treatment, and had then been hospitalized for regular check-ups. Pa- tients who responded to the questionnaire were in- cluded in this study.
Although it might have been possible to limit the survey subjects to only male or female patients or only patients in their 20s to eliminate the factors related to sex and age, the study was conducted universally on patients who had received 2-jaw surgery due to concerns regarding the availability of suitable respondents. Aside from the conditions of 2-jaw surgery and completion of all treatment, we did not perform any particular sampling or ex- clusion of subjects, and gave the questionnaire to all hospitalized patients; however, patients who re- fused to participate were excluded and thus, all re- sponding patients were included in the sample. All patients received fixed orthodontic treatment both before and after the surgery.
The following strategy was used to quantify the survey results about the motives, or improve- ments after surgery. The questions were designed to let the patients score according to importance among each example which the total sum of the score would add to 100. To prevent errors caused by the patients subconsciously imitating the ex- amples, we provided two different examples for each item (Figure 1). We used the visual analogue scale (VAS) method to evaluate changes in self-es- teem, improvements in chewing function, and fa-
1. Please indicate your sex.
1 ) Male 2) Female
2. Please indicate your age.
1 ) 19-29 years old 2) 30-39 years old 3) 40-49 years old 4) Over 50 years old
3. Which do you prefer out of the “surgery first method” (receive 2-jaw surgery first, then start orthodontics immediately afterwards) and the “Orthodontics first method” (proceed with orthodontics for a certain period of time before 2-jaw surgery, and end with orthodontics after surgery)?
1 ) Surgery first 2) Orthodontics first
4. Please provide subjective scores according to the importance of the following motives in making you consider 2-jaw surgery. Make sure that the total is equal to 100.
1) To improve my appearance (I wanted a prettier, more attractive face) 2) To restore self-confidence or overcome a complex
3) To restore function (to chew better) Example 1> Example 2>
1) 20 1) 100
2) 30 2) 0
3) 50 3) 0
Response>
1) 2) 3)
5. Of the motives that made you consider the 2-jaw surgery, if there is something not included in the three options in Question 4, please write it here.
( )
6. What was your greatest concern before receiving the 2-jaw surgery?
1) That the operation would have little effect 2) I was scared of the operation itself
3) That there might be after-effects following the operation
4) That the discomfort or pain during the post-surgical recovery time might be severe 5) Other ( )
Figure 1. Questionnaire. (Continued to the next page)
7. Please provide a subjective score for the improvements following the 2-jaw surgery that are most significant to you. Make sure that the total is equal to 100.
1) My personal satisfaction has increased because my appearance has improved.
2) It has helped my social life, because I have overcome my complex and gained more confidence in interpersonal relations.
3) I had experienced difficulties with food intake due to malocclusion, but after treatment, I am now able to chew better.
Example 1> Example 2>
1) 15 1) 60
2) 15 2) 30
3) 70 3) 10
Response>
1) 2) 3)
8. Of the things that have improved following the 2-jaw surgery, if there is something not contained in the three examples in Question 7, please write it down here.
( )
9. Do you think your self-esteem has improved following the 2-jaw surgery? Please indicate the change in your personal self-esteem before surgery and after completing the surgery and orthodontic treatment, using the linear scales below.
Example> Response>
Before Before
After After
10. Do you think there has been any change in the way you speak since receibing the 2-jaw surgery?
1) Yes 2) No
11. Do you think that mastication (chewing food) has improved following the 2-jaw surgery? Please indicate the change in mastication before surgery and after completing the surgery and orthodontic treatment, using the linear scales below.
Example> Response>
Before Before
After After
12. If you knew someone who was considering receiving the 2-jaw surgery, would you recommend it to them?
1) Yes 2) No
Figure 1. (Continued) Questionnaire. (Continued to the next page)
13. This question is about the extent of change to your face following the 2-jaw surgery. Some people would expect their face to change dramatically following the 2-jaw surgery, and some would anticipate only a tiny, almost imperceptible effect. Please indicate a subjective score, on the linear scales below, of the extent that you expected your face to change before the surgery, and the amount that you feel your face has changed after completing the surgery and orthodontic treatment.
Example> Response>
Before Before
After After
14. How long was the period of time between when you first thought that you would like to receive the 2-jaw surgery and when you actually received the surgery?
1) Less than a month 2) 2-3 months 3) 4-6 months
4) 6 month-year 5) Over a year
15. In the “surgery first method”, you receive the 2-jaw surgery first before starting orthodontic treatment, and although the results can be achieved rapidly, the extent of the surgery is determined by prediction, and therefore, there may be some discomfort with biting immediately after surgery. In the “orthodontics first method”, orthodontics are performed for a certain length of time before the 2-jaw surgery, and the treatment ends with orthodontics after surgery; do to the preparations before surgery, there is comparatively less discomfort from biting after surgery and the outcomes can ge predicted more precisely. However, the period of time leading up to the surgery is longer.
Of the “surgery first method” and the “orthodontics first method”, which one do you prefer?
1) Surgery first 2) Orthodontics first
16. Please only reply if you received surgery with the “surgery first method” (starting orthodontics treatment after receiving the 2-jaw surgery). Do you answer this question if you received orthodontic treatment for more than a month before surgery.
1) I decided on surgery because the surgery first method was available (If I had to undergo orthodontics first, it would have been difficult for me to decide on the treatment).
2) I was glad that the surgery first method was available, but I would have decided on surgery, even if I had to do orthodontics first.
3) I had no interest in whether it was surgery first or orthodontics first, and I do not think it would have made a difference.
Figure 1. (Continued) Questionnaire.
cial change before surgery and after completing surgery and orthodontic treatment.3 The sub- jects indicated their subjective judgments direct- ly through a linear scale, and the numerical val- ue drawn from the VAS was used for statistical analysis. We made each of the examples for these items look as different as possible.
In order to investigate the patients’ awareness and preferences for the surgery first and the or- thodontics first methods, we inserted similar ques- tions into the first and second parts of the ques- tionnaire. In Question 3, we provided a simple definition of the two methods and had the subjects choose their preferred method, and in Question 15, we gave a more detailed explanation of the general strengths and weaknesses of the two methods and had the subjects choose again (Figure 1). We com- pared the two questions and calculated the number of each of the four types of possible answers (Q3
→ Q15): surgery first → surgery first, surgery first
→ orthodontics first, orthodontics first → surgery first, and orthodontics first → orthodontics first.
We used frequency analysis, Wilcoxon signed rank test, and McNemar’s test on a statistical soft- ware package program (SAS System for Windows V 9.3, SAS Institute Inc., Cary, NC, USA) to test for significance in change of self-esteem and mas- ticatory function before and after surgery, and treatment duration between surgery first and or- thodontics first methods, etc.
This study was submitted for assessment by the Catholic University of Korea Songeui Campus In- stitutional Review Board (IRB) at the planning stage, and was conducted after receiving approval along with an exemption from assessment.
RESULTS
The total number of survey subjects was 208, with 83 male (39.90%) and 125 female (60.10%).
In terms of age, 151 subjects were in their 20s (in- cluding 19-year-old) (72.60%), 50 were in their 30s (24.04%), and 7 were in their 40s (3.37%).
In the questions where the subjects assigned subjective scores to motives that made them con- sider the 2-jaw surgery, the average score for ‘2.
To restore self-confidence or overcome a complex’
was the highest, at 43.29 ± 23.61, followed by ‘1.
To improve my appearance’ at 28.85 ± 23.32, and
‘3. To restore function’ at 27.85 ± 26.27 (Figure 2). Among the questions about the subjects’ feel- ings after surgery, ‘2. It has helped my social life, because I have overcome my complex and gained more confidence in interpersonal relations’ had the highest average score at 40.64 ± 24.78, fol- lowed by ‘1. My personal satisfaction has in- creased because my appearance has improved’ at 31.08 ± 21.42, and ‘3. I had experienced difficul- ties with food intake due to malocclusion, but after treatment, I am now able to chew better’ at 28.24
± 27.38 (Figure 3).
The mean value for the patients’ self-esteem be- fore the 2-jaw surgery was 4.16 ± 2.10 out of 10, and 7.46 ± 1.72 after surgery. To evaluate changes in self-esteem before and after the 2-jaw surgery,
Figure 2. The motive for receiving 2-jaw surgery. The Y-axis values are presented as scores that total is equal to 100. Q4- 1: To improve my appearance, Q4-2: To restore self-confi- dence or overcome a complex, Q4-3: To restore function.
we performed a Wilcoxon signed rank test using the value obtained by subtracting the self-esteem values between before and after surgery (Table 1). Compared with the values before surgery, we found that individual self-esteem increased sig- nificantly after completing surgery and orthodon- tic treatment (p < 0.0001).
In the answers for Question 11, asking about changes in patients’ chewing function, the mean score for chewing function before the 2-jaw sur- gery was 5.26 ± 2.28, and after surgery was 7.18
± 1.90. We performed a Wilcoxon signed rank test to assess whether chewing function improved after surgery (Table 1). Compared with chewing func- tion scores before surgery, the scores after surgery were significantly higher (p < 0.0001).
In terms of the patients’ greatest concerns be- fore receiving the 2-jaw surgery, the majority of respondents (58.17%) replied ‘3. That there might be after-effects following the operation,’ fol- lowed by ‘4. That the discomfort or pain during the post-surgical recovery time might be severe’
at 17.79%, ‘2. I was scared of the operation itself’
at 16.35%, ‘1. That the operation would have little effect’ at 4.81%, and ‘5. Other’ at 2.88% (Figure 4). Of the 208 total subjects, 123 patients (59.13%) thought that their way of speaking had changed following surgery, while the other 85 (40.87%) thought it had not changed. When asked if they would recommend 2-jaw surgery to someone they knew, 67.3% of patients replied ‘Yes’ and the other 32.69% replied ‘No.’ More than half (51.44%) of
Figure 3. The effectiveness of 2-jaw surgery. The Y-ax- is values are presented as scores that total is equal to 100.
Q7-1: My personal satisfaction has increased because my appearance has improved, Q7-2: It has helped my social life, because I have overcome my complex and gained more confidence in interpersonal relations, Q7-3: I had experi- enced difficulties with food intake due to malocclusion, but after treatment, I am now able to chew better.
Figure 4. Reasons for hesitation in having a 2-jaw surgery.
The Y-axis values are presented as percentage. Q6-1: That the operation would have little effect, Q6-2: I was scared of the operation itself, Q6-3: That there might be after-effects following the operation, Q6-4: That the discomfort or pain during the post-surgical recovery time might be severe, Q6- 5: Other.
Table 1. The change in self-esteem (Q9) and masticatory function (Q11) of patients after 2-jaw surgery
Before After After-before p value
Q9 4.6 ± 2.1 7.43 ± 1.72 3.3 ± 2.45 <0.0001
Q11 5.26 ± 2.28 7.18 ± 1.9 1.92 ± 3.05 <0.0001
the patients replied that it had taken more than a year between first consideration to actual surgery, followed by 15.87% of patients responding ‘2-3 months,’ 12.98% responding ‘6 months-1 year,’
11.54% responding ‘less than 1 month,’ and the smallest percentage of patients, 8.17%, responding
‘4-6 months.’
Regarding the extent of changes facial changes, the mean score for the extent of change expect- ed by the patients before surgery was 6.50 ± 2.34 out of 10, and the change they actually felt after completing the surgery and treatment was 6.38 ± 1.95. When we compared the two values, we found that 45.63% of patients perceived smaller change after surgery than they had expected prior to sur- gery, and 38.83% of patients responded in oppo- site. Of all the patients, 15.53% stated that their facial change after surgery was the same as they had expected before surgery, demonstrating that the majority of patients obtained a different result than they had expected prior to surgery.
We next analyzed the patients’ preferences be- tween surgery first method and orthodontics first method. When we performed a comparative anal- ysis between the pair of questions (Q3 and Q15), the group that preferred the surgery first meth- od in both questions was 72.12%, irrespective to whether we provided an additional explanation of strengths and weakness (surgery first → surgery first). No patient selected the orthodontics first method in Q3, and then the surgery first method in Q15 (orthodontics first → surgery first) (0.00%) after an explanation of strengths and weakness- es; conversely, 9.62% of patients changed their response from surgery first to orthodontics first (surgery first → orthodontics first), and 18.27% of patients responded orthodontics first to both ques- tions (orthodontics first → orthodontics first) (Ta- ble 2).
For the last item, only the patients who received
the surgery first method were asked to respond, and of the 208 total subjects, only 163 respond- ed. The largest number of patients, at 54.40%, re- sponded with ‘2. I was glad that the surgery first method was available, but I would have decided on surgery, even if I had to do orthodontics first,’
followed by 28.22% responding with ‘1. I decided on surgery because the surgery first method was available,’ and 26.38% responding with ‘3. I had no interest in whether it was surgery first or ortho- dontics first, and I do not think it would have made a difference’.
DISCUSSION
Several studies have reported that surgery, or or- thodontic treatment, improves the face by making it more attractive, and the improvement in appear- ance increases patients’ self-esteem and self-con- fidence, and has a positive influence on social life.4,5 Similarly, in our study, a large number of patients who had received the 2-jaw surgery re- sponded that their self-esteem had improved after surgery. Moreover, we were able to confirm a sta- tistically significant increase in subjective self-es- teem scores.
When we analyzed the motives that caused pa- tients to consider surgery, overcoming complexes and restoring self-confidence made up a high pro- portion of responses. Additionally, in the question about actual positive effects of surgery, the largest
Table 2. Comparison of responses to Q3 followed by Q15
Q3
Q15
Surgery first Orthodontics first
Surgery first (170) 150 20
Orthodontics first (38) 0 38
Total (208) 150 58
proportion of respondents stated that it had helped interpersonal relations and social life. This can be interpreted that patients not only anticipate for sat- isfying improved appearance and mastication, but also social and psychological effects when plan- ning 2-jaw surgery, and place importance on these aspects in the results of the surgery.
One study reported that patients who had re- ceived orthodontic camouflage treatment showed the same level of satisfaction in treatment results as surgical patients.6 This makes it difficult to generalize that, among all treatment alternatives, only surgical methods have an effect on patients’
self-esteem. Meanwhile, other studies report that patients who perceive their own skeletal struc- ture or occlusion state to be outside of the nor- mal range prefer surgical treatment to orthodontic treatment alone.7
The correlation of temporomandibular joint dis- orders with orthognathic surgery or orthodontic treatment is debatable;8 We did not include infor- mation about temporomandibular joint disorders in our study. However, in reality, there are consid- erable amount of malocclusion patients with tem- poromandibular joint symptoms, hoping to receive 2-jaw surgery. Additionally, some of the patients who responded to our questionnaire had temporo- mandibular joint symptoms prior to surgery. A re- cent study showed that orthognathic surgery ac- companied by orthodontics yielded a significant decrease in temporomandibular joint symptoms.9 Together with a balanced facial appearance and improvements in chewing, improvement in tem- poromandibular joint symptoms, which are high- ly correlated with psychological factors such as stress, could be included in the factors contribut- ing to the improvement of patients’ self-esteem.
The majority of patients considering 2-jaw sur- gery is skeletal class II or III malocclusion pa- tients. In the planning stage of the surgery, the two
types of malocclusion show different directions of jaw movements. In our analysis, we did not dif- ferentiate between patients who were classified as class II or class III malocclusion. However, inter- estingly, a previous study found that class III pa- tients showed lower self-esteem related to person- al appearance than class II patients before surgery.
Additionally, after surgery, not only the patients, but also their family and friends reported a great- er sense of improvement in facial attractiveness.2 In a study involving only class III patients, 72%
of the patients were satisfied with the results of surgical treatment, about 50% said that their per- sonality and life were affected positively, and 71%
stated that masticatory function had improved.10 Although our study did not differentiate between types of malocclusion, the results were similar.
In the traditional method for orthodontic treat- ment with orthognathic surgery, orthodontics is performed before surgery for teeth alignment, de- compensation, and adjusting the arch shape. Af- ter surgery, the treatment is completed with ortho- dontics to settle occlusion. However, the method of performing surgery first without a preoperative course of orthodontic treatment can achieve fast- er improvements in facial appearance compared to the orthodontics first method, and shorten the overall treatment time.11 Since its introduction, the proportion of orthognathic surgery patients being treated by this surgery first method has increased considerably compared to the conventional ortho- dontics first method. However, contrary to these advantages, because the degree of surgery is de- termined by prediction, treatment simulation and the accuracy of the predicted tooth alignment and occlusal stability are important factors in the suc- cess of the surgery first treatment.12 In our study, we found that a high proportion of patients were aware of the advantages of the surgery first meth- od and preferred it; however, 71.78% of patients
replied that the possibility of using the surgery first method was not a decisive factor in planning the treatment. Accordingly, although the number of patients choosing the surgery first method to achieve a rapid improvement in appearance has increased, the majority of patients do not place great significance on the surgery first method.
This could imply that if pre-surgical orthodontic treatment were diagnosed to be necessary, there would be a high rate of cooperation.
For patients with skeletal disharmony, ortho- dontics with orthognathic surgery is an excellent choice for treatment; however, many patients have a vague fear or dislike of surgery under general anesthetic that causes them to delay the treatment decision. Accordingly, in our study, 58.17% of all respondents chose the possibility of post-surgical effects as their greatest worry prior to surgery.
The most common problems experienced by pa- tients after orthognathic surgery include numb- ness and edema, and more than half of patients complain of pain after surgery.10 Providing a suf- ficient explanation of surgical treatment methods and processes to patients and systematizing thor- ough post-surgical care could ease patients' vague fears of the 2-jaw surgery and increase post-surgi- cal satisfaction.
The main subject of our study was the evalua- tion of the sociological and psychological effects of 2-jaw surgery on patients, and our research was conducted under the assumption that the majority of patients were, to some extent, satisfied with the results of their treatment. In our survey, there is a possibility that the patients’ responses may have reflected their total treatment satisfaction because we did not investigate subjective satisfaction as the result of surgery. One limitation of our study is that we were unable to conduct our survey selec- tively on patients with the same high level of sat- isfaction, which could have produced results that
are more consistent.
CONCLUSION
The purpose of this study was to evaluate the preoperative and actual outcomes of the patients who underwent 2-jaw surgery through a survey method. The biggest motivation for receiving 2-jaw surgery was overcoming the complex or im- proving self-confidence, and the improvement of self-esteem and chewing function were statisti- cally confirmed. However, there were many cases where the expectations of the patients before the 2-jaw surgery and the actual results did not match.
REFERENCES
1. O’Brien K, Wright J, Conboy F, Appelbe P, Bearn D, Caldwell S, Harrison J, Hussain J, Lewis D, Littlewood S, Mandall N, Morris T, Murray A, Oskouei M, Rudge S, Sandler J, Thiruvenkatachari B, Walsh T, Turbill E.
Prospective, multi-center study of the effectiveness of orthodontic/orthognathic surgery care in the United Kingdom. Am J Orthod Dentofacial Orthop 2009;135:709-714.
2. Gerzanic L, Jagsch R, Watzke IM. Psychologic implications of orthognathic surgery in patients with skeletal Class II or Class Ⅲ malocclusion. Int J Adult Orthodon Orthognath Surg 2002;17:75-81.
3. Wewers ME, Lowe NK. A critical review of visual analogue scales in the measurement of clinical phenomena. Res Nurs Health 1990;13:227-236.
4. Garvill J, Garvill H, Kahnberg KE, Lundgren S.
Psychological factors in orthognathic surgery. J Craniomaxillofac Surg 1992;20:28-33.
5. Klages U, Bruckner A, Guld Y, Zentner A. Dental esthetics, orthodontic treatment, and oral-health attitudes in young adults. Am J Orthod Dentofacial Orthop 2005;128:442-449.
6. Mihalik CA, Proffit WR, Phillips C. Long-term follow-up of Class II adults treated with orthodontic camouflage: a comparison with orthognathic surgery outcomes. Am J Orthod Dentofacial Orthop 2003;123:266-278.
7. Phillips C, Proffit WR. The psychological effect of dentofacial deformity. In: Proffit WR, White RP, Sarver DM, editors. Contemporary treatment of dentofacial deformity. St Louis: Mosby; 2002.
8. Rodrigues-Garcia RC, Sakai S, Rugh JD, Hatch JP, Tiner BD, van Sickels JE, Clark GM, Nemeth DZ, Bays RA. Effects of major Class II occlusal corrections on temporomandibular signs and symptoms. J Orofac Pain 1998;12:185-192.
9. Pahkala RH, Kellokoski JK. Surgical-orthodontic treatment and patients’ functional and psychosocial well- being. Am J Orthod Dentofacial Orthop 2007;132:158- 164.
10. Zhou YH, Hägg U, Rabie AB. Patient satisfaction following orthognathic surgical correction of skeletal Class III malocclusion. Int J Adult Orthodon Orthognath Surg 2001;16:99-107.
11. Nagasaka H, Sugawara J, Kawamura H, Nanda R.
“Surgery first” skeletal Class III correction using the Skeletal Anchorage System. J Clin Orthod 2009;43:97- 105.
12. Baek SH, Ahn HW, Kwon YH, Choi JY. Surgery-first approach in skeletal class III malocclusion treated with 2-jaw surgery: evaluation of surgical movement and postoperative orthodontic treatment. J Craniofac Surg 2010;21:332-338.
ABSTRACT
The purpose of this case report is to describe the considerations in orthodontic treatment and orthognathic surgery in a patient with skeletal Class III malocclusion that had camouflage orthodontic treatment. A patient who had camouflage orthodontic treatment with four 1st premolars extraction showed hyperdivergent skeletal Class III malocclusion and asymmetry. Open coil springs were used to regain the extraction space of the mandibular first premolars and decompensate lower anterior teeth, and a criss-cross elastics was used to upright the lower right molars for posterior decompensation. Le Fort I and midpalatal segmental osteotomy were performed to achieve total impaction (2 mm), forward movement (2 mm) and expansion (3 mm) of the maxilla. Bilateral sagittal segmental osteotomy (BSSRO) was performed to achieve asymmetric set back of the mandible (right: 6 mm, left: 10 mm). The asymmetric and protruded mandible was corrected after orthognathic surgery and orthodontic treatment, resulting in an aesthetic facial appearance, and ideal overjet and overbite. After 1 year of orthodontic treatment, stable occlusal relationship, appropriate overjet and overbite were observed. (Clin J Korean Assoc Orthod 2019;9(3):138-150)
Key words Class III malocclusion, Asymmetry, Orthognathic surgery, Decompensation
성장기 때 절충교정치료 경험이 있는 골격성 III급 부정교합 환자의 수술 교정 치험례
경효정, 이예슬, 박기호
경희대학교 치과대학 치의학전문대학원 치과교정학교실
Surgical Orthodontic Treatment of Hyperdivergent Skeletal Class III Malocclusion Patient Experienced in Camouflaging Orthodontic
Treatment: Case Report
Hyo-Jung Kyung, Ye-Seul Lee, Ki-Ho Park
Department of Orthodontics, School of Dentistry, Kyung Hee University, Seoul, Korea
Dr. 이 예 슬 Dr. 경 효 정
Corresponding author: Ki-Ho Park Department of Orthodontics, School of Dentistry, Kyung Hee University,
23 Kyungheedae-ro, Dongdaemun-gu, Seoul 02447, Korea Tel: +82-2-958-9390 E-mail: [email protected] Received: May 10, 2019 / Revised: June 3, 2019 / Accepted: June 3, 2019
Dr. 박 기 호
서론
하악골 전돌은 아시아인에게서 발생 빈도가 높고 안 면 비대칭이 동반되는 경우가 흔하다. 심한 골격적 부조 화를 동반하는 골격성 III급 부정교합 환자의 경우 악교 정 수술을 동반한 교정치료를 통해 환자의 심미적 안모 및 기능적 교합을 향상시킬 수 있으나, 골격적 부조화 가 미약하거나 중등도인 경우에는 절충 교정치료도 대 안이 될 수 있다. 절충 교정치료 시에는 환자의 초진 상 태에 따라 비발치1나 하악 절치 발치,2 또는 소구치 발 치3,4 등을 동반한 치료를 선택할 수 있다.
그러나 골격적 부조화가 중등도 이상임에도 불구하 고 무리하게 절충 교정치료를 시도하거나 골격적 부조화 가 심하지 않았더라도 하악골의 만기 성장에 의해 악골 부조화가 심해진 경우에는 성장 종료 후 악교정 수술을 동반하는 재교정치료가 필요할 수도 있다. 이러한 경우 절충 치료를 진행하는 과정에서 더욱 심해진 치성 보상 을 어떻게 탈보상할 것인지에 대해 계획을 세우는 것이 중요하다.
본 증례에서는 성장기에 상·하악 양측 제1소구치 발 치를 동반한 절충 교정치료를 받은 경험이 있고 안면 비 대칭을 동반한 과발산형 골격성 III급 부정교합 환자에 서 악교정 수술을 통해 골격적 부조화를 해소하고, 심 미적이고 안정적인 치료 결과를 얻었기에 이를 보고하 고자 한다.
진단
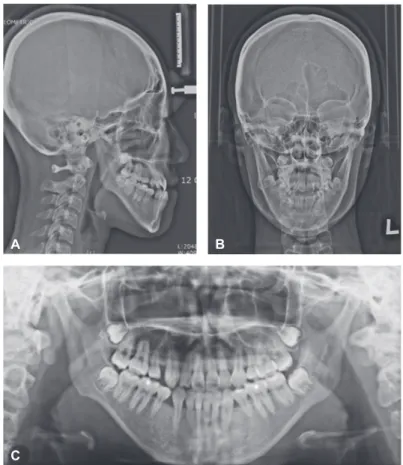
“주걱턱 때문에 악교정 수술 상담하러 왔어요.”라는 주소로 19세 여자 환자가 내원하였다. 환자는 12~15세 에 상·하악 양측 제1소구치 발치를 동반한 절충 교정치 료를 받은 경험이 있었다. 초진 시 정모에서 보았을 때 턱끝이 우측으로 편위되었으며, 미소 시에 상악 전치 노출도가 과도하였다. 측모에서는 안면이 수직적으로
길며 하안면부가 전방 돌출되어 보이고, 오목한 안모를 나타냈다(Figure 1A). 구내에서는 전치부의 절단 교합 을 보였고, 좌·우측 모두 III급 구치와 견치 관계가 관 찰되었으며, 안모 정중선에 비해 하악 전치의 중심선이 우측으로 2 mm 편위되어 있었다(Figure 1B).
측면 두부방사선계측사진에서 전후방적으로는 상악 골이 작고 하악골이 큰 골격성 III급 부정교합을, 수직 적으로는 과발산형 장안모 양상을 보였으며 다소 가파 른 교합평면을 보였다. 상악 전치의 각도는 프랑크포르 트 평면에 대해서는 정상 범주였으나 상악 교합 평면에 대해서는 순측 경사되어 있었다. 소구치 발치를 포함한 절충 교정치료로 인하여 하악 전치는 과도하게 설측 경 사되어 있었다. 파노라마상에서 4개의 제3대구치가 관 찰되었다. 콘빔 전산화단층촬영(CBCT)상에서 하악 전 치부의 얇은 치조골이 관찰되었으며, 상악 구치 폭경이 하악 구치에 비해 좁았다. 또한, 하악의 우측 편위에 의 한 횡적 보상으로, 우측 하악 대구치는 심한 설측 경사 를 보였다(Figures 2, 3, Table 1). 이를 종합하여 안 면 비대칭을 동반한 과발산형 골격성 III급 부정교합으 로 진단하였다.
치료계획
상·하악골의 전후방적인 부조화와 긴 안모 및 안면 비대칭을 개선하기 위해 악교정 수술을 동반한 교정치 료를 계획하였다. 성장기 동안의 상·하악 제1소구치 발 치를 동반한 절충 교정치료로 인해 하악 전치의 치축이 과도하게 설측 경사되어 있었기 때문에, 수술 시 하악 의 후방이동량을 충분히 확보하기 위해 술전 교정치료 시에 하악 양측 제1소구치의 발치 공간을 재획득하면서 하악 전치를 순측으로 탈보상하기로 계획하였다. 상악 의 교합 평면에 대해서 순측 경사되어 있는 상악 전치 를 설측으로 탈보상하기 위해서 상악 견치와 제2소구치 사이에 있는 발치 공간을 이용하여 상악 전치를 후방
Figure 1. Pretreatment facial (A) and intraoral (B) photographs.
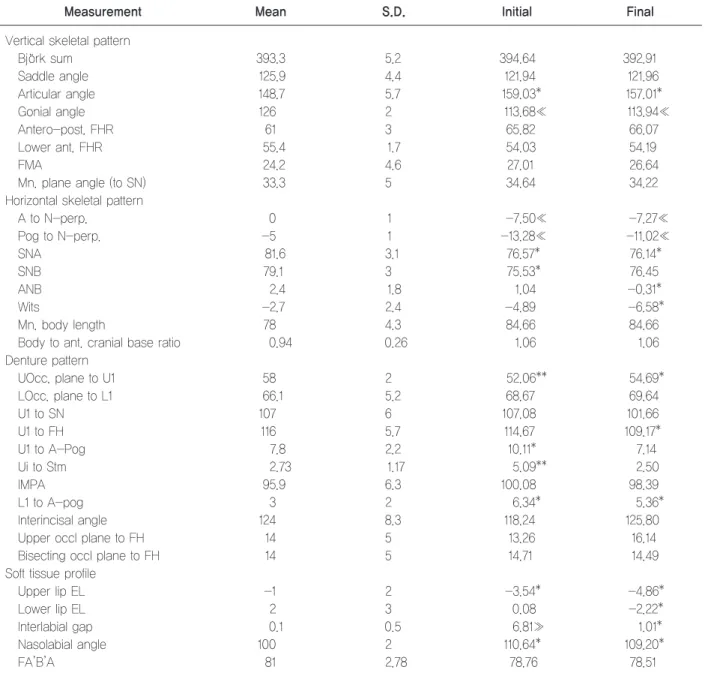
Table 1. Pretreatment and posttreatment cephalometric measurements
Mean Initial Final
SNA (°) 81.3 78.82 80.85
SNB (°) 79.2 80.46 76.95
ANB (°) 1.5 -1.64 3.90
N perp-Pt.A (mm) 1.0 -0.79 2.60
N perp-Pog (mm) 0.5 -1.04 -2.58
Sum (°) 391.8 411.80 412.16
FMA (°) 23.5 41.31 40.74
PFH/AFH (%) 70.0 53.58 52.38
OP-FH (°) 4.6 17.68 16.81
U1-FH (°) 116.6 114.09 114.20
U1-MxOp 55.0 51.50 51.50
IMPA (°) 89.7 61.29 76.90
Interincisal angle (°) 124.1 143.31 128.17
A
B
Figure 2. Pretreatment cephalogram and panoramic radiograph. A, Lateral cephalogram. B, PA cephalogram. C, Panorama.
A
C
B
Figure 3. Pretreatment CBCT images. A, Lower incisors #41 (left), #31 (right). B, Lover 1st molars.
A B
견인하기로 하였다. 하악골의 우측 편위에 따른 횡적 치 아치조성 보상은 술전 교정치료 과정에서 교차 고무줄 을 이용하여 해소하기로 하였다. 술전 교정치료 후 환자 의 심미적인 안모 달성을 목표로 양악 수술을 시행하기 로 하였으며 술후 교정치료 종료 후 하악 제1소구치 발 치 공간은 임플랜트 수복을 하기로 계획하였다.
치료경과 및 결과
치료경과
상·하악 제3대구치 발치 후 술전 교정치료를 시작하 였다. 0.022-inch 슬롯의 자가결찰 브라켓(Clippy-C, Roth)을 상·하악 치열에 부착하고 상·하악에 0.014- inch 나이티놀(Sentalloy) 와이어를 삽입하여 배열과 레벨링을 시작하였다. 배열 3개월부터 하악 양측 제1소
구치 위치에 오프 코일 스프링을 활성화하여 하악 전치 를 순측으로 탈보상하였으며, 상악 전치는 상악 제1소 구치의 발치 공간을 이용하여 후방으로 견인하였다. 하 악 우측 구치부의 설측에 버튼을 부착하고, 상악 우측 구치부의 협측 브라켓과 교차 고무줄을 사용하여 횡적 보상으로 경사된 치아의 협설 치축의 직립을 도모하였 다. 술전 교정치료 후 10개월째 측면 두부방사선계측사 진과 CBCT 자료를 통해 하악 전치가 순측으로 상당량 탈보상이 이루어지고, 상악 전치가 설측 탈보상이 이루 어진 것과 하악 우측 구치부가 협측으로 적절히 직립 된 것을 확인한 후 악교정 수술을 준비하였다(Figures 4-6).
Surgical treatment objective (STO)와 모형 수술 을 시행한 결과, 상악골은 르포르 I 골절단술을 통하여 상악골의 2 mm 상방 함입과 2 mm 전방 이동을 계획
Figure 4. Pre-surgical facial (A) and intraoral (B) photographs.
A
B
Figure 5. Pre-surgical cephalogram and panoramic radiograph and superimposition (pretreatment, pre-surgical). A, Lateral ceph- alogram. B, PA cephalogram. C, Panorama. D, Superimposition (pretreatment, pre-surgical).
Figure 6. Pre-surgical CBCT images. A, Lower incisors #41 (left), #31 (right). B, Lower 1st molars.
A
A B
C D
B
하였으며, 상악궁을 3 mm 확장하기 위해 정중구개봉 합 분절 절단술을 부가적으로 계획하였다. 하악골의 비 대칭과 전돌을 개선하기 위해 하악지 양측 시상분할골 절단술(BSSRO)을 통해 우측 원심 골편을 6 mm, 좌 측 원심 골편을 10 mm 후방 이동하기로 계획하였다 (Figure 7). 또한, 턱끝의 수직 고경을 줄이고 전방으 로 이동시키기 위해 턱끝 성형술을 부가적으로 시행하 기로 하였다. 계획한 교합대로 양악수술을 시행하여 하 악 전돌 및 비대칭이 개선되었다(Figures 8, 9).
악교정 수술 후 6주 경과 후 술후 교정치료를 시작하 였으며 소구치와 대구치 부위에 삼각형 III급 악간 고무 줄을 이용하여 교합을 안정화한 후 마무리하였다. 적절 한 치아 크기 비율(Bolton ratio) 형성을 위해 왜소치 인 상악 우측 측절치 부위에 약간의 공간을 남긴 채 교 정장치 제거 후 보철치료를 받기로 계획하였다. 총 치료
기간은 23개월이었다(Figure 10). Figure 7. Surgical treatment objective (STO).
Figure 8. Post-surgical facial (A) and intraoral (B) photographs (after 6 weeks).
A
B
Figure 10. Posttreatment facial (A) and intraoral (B) photographs.
Figure 9. Post-surgical cephalogram, panoramic radiograph and superimposition (pre-surgical, post-surgical). A, Lateral cephalo- gram. B, PA cephalogram. C, Panorama. D, Superimposition (pre-surgical, post-surgical).
A B
C D
A
B
치료결과
치료 후 사진에서 비대칭적인 안모와 전돌된 하악, 미 소 시 과도했던 상악 전치 노출도가 개선되어 심미적인 안모를 보였고, 이상적인 전치부 수직피개 및 수평피개 가 달성되었다(Figure 10). 측면 두부방사선계측사진에 서 하악 전치의 양호한 전후방 경사를 보였으며, 하악 제1소구치 임플랜트 공간이 재획득되었다. 파노라마방 사선사진에서 상악 우측 견치를 제외하고 양호한 치근 평행도를 보였다. 치료 전·후의 측면 두부방사선계측사 진의 중첩에서 상악골의 전방 및 상방 이동과 하악골의 후방 이동으로 인한 골격의 전후방적인 부조화 및 수직 고경의 심미적 개선을 보였으며, 정면 두부방사선계측사
진에서는 악골 비대칭의 개선을 보였다(Figure 11). 상 악골 중첩 시 치료 후 상악 제1대구치 간 거리는 초진 시보다 증가하였으며, 초진 때와 비교하여 하악 전치부 순측 치은 퇴축은 관찰되지 않았으나 CBCT에서 원래 얇았던 하악 전치부 순측 치조골이 더 소실된 것이 관 찰된다(Figure 12). 술전 교정치료 과정에서 설측으로 탈보상이 이루어졌던 상악 전치부는 술후 교정치료 과 정에서 다시 순측 경사되었다.
교정치료 종료 1년 후, 상악 좌측 측절치에 보철 치료, 하악 양측 제1소구치에 임플랜트 식립을 받은 상태로 안 정적인 교합 관계와 적절한 수직, 수평피개를 보이고 유 지상태가 양호한 것을 확인할 수 있다(Figure 13).
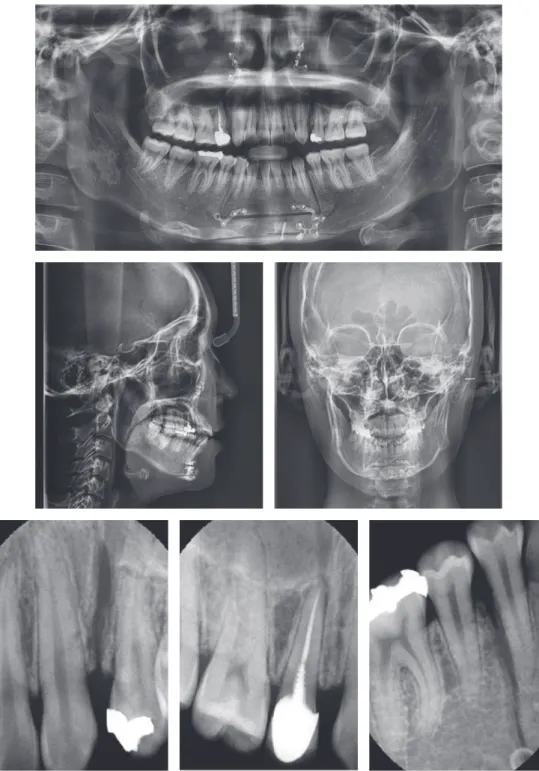
Figure 11. Posttreatment cephalogram, panoramic radiograph and superimposition (pretreatment, posttreatment). A, Lateral cephalo- gram. B, PA cephalogram. C, Panorama. D, Superimposition (pretreatment, posttreatment).
A B
C D
Figure 12. Posttreatment CBCT images. A, Lower incisors #41 (left), #31 (right). B, Distance between upper 1st molars.
A B
Figure 13. 1-year retention facial (A) and intraoral (B) photographs.
A
B
고찰
본 증례는 골격성 III급 부정교합 환자로 성장기에 상·하악 제1소구치 4개를 발치하고 절충 교정치료를 시 행하였으나, 성장이 진행됨에 따라 하악골의 전돌과 안 면비대칭이 심화되어 악교정 수술을 받기 위하여 내원 하여 치료한 경우이다. 내원 시 상악 전치부의 각도는 정상인 반면에 하악 전치부는 심하게 설측 경사되어 있 었으며 잇몸 보이는 웃음(gummy smile)을 보였다.
하악의 과잉 성장이 동반된 성장 중인 골격성 III급 부정교합 환자의 진단 및 치료계획을 수립함에 있어서 성장을 예측하는 것은 매우 중요하다. 특히 상악골이나 하악골에 악정형 치료가 예상되는 성장기 아동에 있어 서는 조기진단의 필요성이 강조되어 왔다. 그러나 지난 50년 동안 Bj¨ork 등을 비롯한 수많은 선학자들이 하악 골 성장 예측에 대해 연구를 해 왔지만5-8 아직까지 정 확한 성장 예측을 하는 것은 어려운 문제이다. 따라서 하악골 과잉 성장이 예상되는 경우에는 성장기 때 교정 치료를 시행하는 것에 신중해야 하며, 특히 하악 소구 치 발치를 동반한 교정치료의 경우 향후 하악골의 추가 성장에 의해 악교정 수술과 임플랜트를 필요로 할 수 있기 때문에 더욱 주의를 기울여야 할 것이다.
수술 전 교정치료는 골격적 부조화로 인해 야기된 치 아의 보상을 탈보상하여 현재의 교합관계를 고려하지 않고 각 기저골에 대하여 치아를 정상적으로 위치시키 는 과정이며, 이 과정을 통해 수술 후 안정적인 교합 형 성, 골격적 안정성을 증진시킬 수 있다. 이는 수술을 위 한 준비 단계로서, 수술 시 원하는 위치로 악골을 이동 시키는 것을 치아들이 방해하지 않게 하기 위하여 시행 하는 과정이다. 골격성 III급 부정교합 환자의 경우 골 격성 보상에 의해 하악 전치부가 설측 경사되는 경우가 많은데 절충 교정치료 시 전치부 반대교합을 개선하기 위해 하악 소구치 발치를 시행하면 하악 전치부의 설측 경사는 더욱 심해질 수 있다. 본 증례는 성장기에 상·
하악 제1소구치 4개를 발치하고 절충 교정치료를 시행 하였기 때문에 초진 시 하악 전치부의 설측 경사가 과도 하였고 이를 탈보상하는 과정이 필요하였다. 설측 경사 된 하악 전치를 순측 경사시키고 제1소구치 발치 공간 을 재획득하기 위해 오픈 코일 스프링을 사용하였다.
Zhang과 Lee9은 일반적으로 골격성 III급 부정교합 환자의 전치부 치조골 두께가 일반인에 비해 얇다고 하 였는데, 이 환자의 경우에도 초진 시에 하악 전치의 순 측 치조골의 두께가 얇았으며, Choi 등10은 술전 교정 치료 과정에서 하악 전치부 순측 치조골이 더 얇아지 거나 치은 퇴축이 발생할 수 있다고 하였다. 여러 임상 가들이 하악 전치부의 치조골이 얇은 골격성 III급 부 정교합 환자에서 골이식과 피질골 절제술(augmented corticotomy)을 동반한 술전 교정을 시행하여 치조 골 흡수나 치은 퇴축과 같은 치주 조직의 부작용을 최 소화하고 탈보상의 양을 충분히 하고자 하였다.11-13 본 증례의 환자에서도 술전 교정치료 과정에서 치 주 조직의 부작용을 관찰하면서 필요시 augmented corticotomy를 시행하기로 하였으나 술전 교정을 통 해 하악 전치의 순측 탈보상이 상당히 진행되었음에도 임상적으로 치은 퇴축과 같은 부작용이 관찰되지 않 아 이를 시행하지 않았으나 CBCT에서는 순측 치조골 의 소실이 관찰되었다. 초진 시부터 하악 전치부 순측 치조골이 얇았던 환자였기 때문에 초반에 augmented corticotomy를 시행하였더라면 최종적으로 하악 전치 부가 더 많은 양의 치조골의 지지를 받았을 것으로 판 단되며 본 교정치료 과정에서 아쉬운 부분이다.
상악 교합평면에 대해서 순측 경사된 상악 전치부가 술전 교정치료 과정에서 설측 탈보상이 이루어졌으나 술후 교정치료 과정에서 다시 순측 경사가 발생하였다.
아마도 술후 교정 과정에서 사용한 III급 악간 고무줄 때문에 발생한 것으로 판단되며 교정치료 시 상악 구치 부 사이에 골격성 고정원을 식립하고 이를 고정원으로 이용하여 III급 악간 고무줄을 걸거나 전 치열 후방 이