12
급성 합병성 담낭염의 치료에서 PTGBD의 유용성
을지대학교병원 외과
김정혁ㆍ박혜원ㆍ이문수ㆍ이민구ㆍ조병선ㆍ박주승
Impact of PTGBD on Patients with Acute Complicated Cholecystitis:
Consecutive 4,000 Cases of Laparoscopic Cholecystectomy
Jung Hyuk Kim, M.D., Hye Won Park, M.D., Mun Su Lee, M.D., Min Koo Lee, M.D., Byung Sun Cho, M.D., Joo Seung Park, M.D.
Department of Surgery, Eulji University Hospital, Daejeon, Korea
Purpose: The aim of this study was to determine the advantage of adequate PTGBD in acute complicated cholecystitis patients.
Methods: We performed a retrospective review of a collected database from September 2001 to July 2008. Acute cholecy- stitis with gangrene or perforation was defined as acute complicated cholecystitis. A PTGBD was performed for these patients immediately after the diagnosis using US or CT and then a tubogram was performed after 5∼7 days. After evaluating the gallbladder (GB) and common bile duct (CBD) with a tubogram, we removed the drainage tube and the patients underwent a LC after readmission.
Results: Three hundred seventy four of the 893 patients who were diagnosed with acute cholecystitis underwent PTGBD. While 19 (3.2%) of the total acute cholecystitis patients were converted to open cholecystectomy due to severe inflammation, 14 (3.7%) of the acute complicated patients were converted to open cholecystectomy. In 79
patients, the pre-operative tubogram showed the presence of CBD stone and so ERCP was performed. There were no post-operative deaths.
Conclusion: PTBGD in acute complicated cholecystitis patients allows the early relief of acute cholecystitis symptoms.
This allows sufficient evaluation and treatment for CBD during the PTGBD state. Furthermore, this decreases the mortality and morbidity in the high-risk patients due to sufficient evaluation and management of the underlying critical disease, which allows elective cholecystectomy when the patients is in better condition for surgery. Therefore, PTGBD can be useful for acute complicated cholecystitis.
Key words: Laparoscopic cholecystectomy, Complicated acute cholecystitis, Percutaneous transhepa- tic gallbladder drainage (PTGBD)
중심단어: 복강경 담낭절제술, 급성 합병성 담낭염, 경피간 담낭배액술
※ 통신저자:박주승, 대전시 서구 둔산동 우편번호:301-726
을지대학교병원 외과
Tel:042-611-3864, Fax:042-259-1116 E-mail:[email protected]
서 론
담낭염 환자에서 복강경 담낭절제술(laparoscopic cholecy- stectomy: LC)은 표준 치료로써 지난 십여년간 시행 되어오 고 있다. 복강경 담낭절제술이 담낭염의 표준 술식으로 인 정받은 이후로 급성 합병성 담낭염 환자에서도 진단 즉시 가능한 빠른 시기에 복강경 또는 개복 담낭절제술을 시행 하는 것이 표준 술식으로 그동안 많은 병원의 외과의들에 의해 시행되어왔으나 급성 합병성 담낭염 환자의 경우 담 낭 주변의 심한 염증 반응으로 인한 수술의 어려움으로 개 복술로의 높은 전환율과 수술 전후의 높은 합병증 발생 등 의 문제가 여전히 남아있다. 그래서 최근 급성 합병성 담낭
염 환자에서 급성 염증기에 경피간 담낭배액술(percutane- ous transhepatic gallbladder drainage: PTGBD)을 이용한 치료 의 유용성이 점차 제기되어 왔다.1-4 그러나 아직도 PTGBD 의 정확한 대상 및 시행 후 적절한 제거 시기와 수술 시기 에 대해서는 표준 술식이 없이 각 임상의들의 경험에 의지 해 시행되고 있다. 이에 우리는 본원에서 단일 외과의에 의 한 장기간의 많은 환자들에게서 시행된 PTGBD 후의 복강 경 담낭절제술의 결과를 통해 PTGBD를 이용한 치료 방침 과 유용성에 대해 보고하고자 한다.
대상 및 방법
본원 외과에서 1992년 1월부터 2009년 3월까지 시행된 복강경 담낭절제술 환자 4,700명 중 기록이 가능했던 2001 년 9월부터 2008년 6월까지의 2,067명의 환자를 대상으로 후향적인 분석을 시행하였다. 상기 기간 중 담낭염으로 수 술을 시행했던 환자들은 환자의 연령, 수술 기왕력, 타 질병 기왕력 등에 관계없이 모두 일차적으로 복강경 담낭절제술
Table 1. General feature of patients
Yes (n, %) No (n, %) Biliary colic Hx.
Previous abdominal op. Hx.
Past medical Hx.
DM
Acute cholecystitis Biliary scan PTGBD ERCP
Open cholecystectomy
1,316 (63.7) 672 (32.5) 812 (39.3) 238 (11.5) 893 (43.2) 106 (5.1) 374 (18.1) 427 (20.7) 67 (3.2)
751 (36.3) 1,395 (67.5) 1,255 (60.7) 1,829 (88.5) 1,174 (56.8) 1,956 (94.9) 1,693 (81.9) 1,640 (79.3) 2,000 (96.8) DM = diabetes mellitus; PTGBD = percutaneous transhepatic gallbladder drainage; ERCP = endoscopic retrograde cholangio- pancreatography.
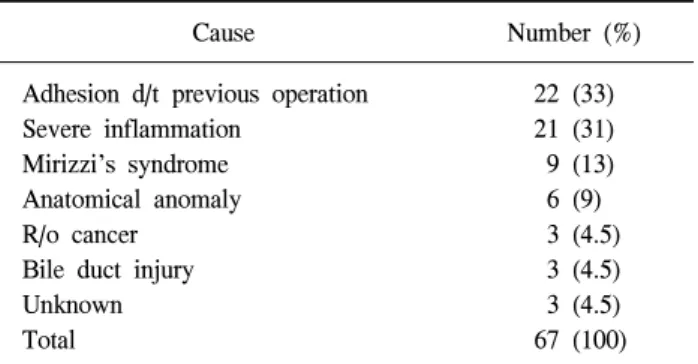
Table 2. Cause of conversion in cholecystitis patients
Cause Number (%)
Adhesion d/t previous operation Severe inflammation
Mirizzi’s syndrome Anatomical anomaly R/o cancer
Bile duct injury Unknown Total
22 (33) 21 (31) 9 (13) 6 (9) 3 (4.5) 3 (4.5) 3 (4.5) 67 (100) Total conversion rate: 67/2,067 = 3.24% → conversion rate d/t inflammation: 1.74%.
이 시도되었고 단일 외과의에 의해 집도되었다. 담낭 용종 및 종양으로 수술한 환자는 제외하였다.
급성 담낭염의 진단은 이학적 검사상 심한 우상복부 통 증과 압통을 동반한 Murphy sign 양성, 초음파 및 복부 컴퓨 터 단층 촬영(CT)상 담낭벽의 과도한 비후 및 팽창, 담낭 점막의 조영 증강, 담낭 주위의 수액 저류, 담낭 내 또는 담 낭 벽의 가스 형성, 담낭 주위의 농양 형성, 간담도 스캔 (DISIDA scan)상 양성 소견 등으로 진단하였고 초음파나 복 부 컴퓨터 단층 촬영상 천공성 담낭염이나 괴사성 담낭염 으로 진단된 경우나 의심되는 경우를 급성 합병성 담낭염 으로 정의하였다. 급성 담낭염 환자 중 입원 후 항생제 치료 에도 불구하고 담낭염의 증상이 24시간 이상 지속되는 경 우에 합병성 담낭염의 위험이 있는 것으로 보고, 급성 합병 성 담낭염으로 진단된 환자 또는 합병성 담낭염의 위험이 있는 환자는 즉시 PTGBD를 시행하였고, 환자의 증상이 소 실되고 배액관으로 나오는 담즙이 정상이 되면 PTGBD후 5∼7일 사이에 tubogram을 시행하여 총담관과 담낭관에 대한 평가 후 배액관을 제거하였다. 복강경 담낭절제술은 PTGBD 를 제거한 뒤 퇴원하였다가 평균 퇴원 후 10∼14일 사이에 재입원하여 시행하였다. 일부 담낭관에 담석이 막혀 염증 이 호전되지 않은 경우에서는 PTGBD를 제거하지 않고 바 로 수술을 시행하였다.
모든 환자에 대한 자료는 전향적으로 수집된 간담췌 데 이터베이스를 이용하였다. 환자의 과거력상 수술의 위험성 을 증가 시킬 수 있는 당뇨, 고혈압을 포함한 심혈관 질환, 뇌혈관 질환, 만성 폐쇄성 폐질환 중 2가지 이상의 질환을 동반한 환자를 합병성 내과적 병력을 지닌 환자로 분류하 였고, 70세 이상의 고연령군과 70세 미만 환자 중 합병성 내과적 병력을 가진 환자를 합쳐서 수술의 고위험군으로 정의하였다.
결 과 1) 환자의 일반적 특성
담낭염으로 수술을 시행한 2,067명의 환자의 평균 연령 은 52.5세(14∼89)였으며 여성이 1,157명(55.0%)으로 남성 (901명, 45.0%)보다 많았다. 1,174명(56.8%)이 만성 담낭염 환자였고, 893명(43.2%)이 급성 담낭염 환자였다. 급성 담 낭염 환자 중 103명(11.5%)의 환자는 비결석성 담낭염 환자 였다. 과거력상 복부 수술의 기왕력이 있는 환자는 672명 (32.5%)이었고, 급성 합병성 담낭염으로 진단되어 PTGBD 를 시행한 환자는 374명(18.1%)였다(Table 1).
평균 수술 시간은 25.8분(±11.6)이었으며 남성(27.9±12.6 분)이 여성(24.2±10.6분)에 비해 오래 걸렸으며(p=0.001), 급 성 합병성 담낭염 환자에서는 34.9분(±13.6)으로 급성 담낭 염(30.0±13.3분)이나 만성 담낭염(22.8±9.1)에 비해 유의하 게 길었다(p=0.001).
2) 개복술로의 전환율
2,067명의 환자 중 67명의 환자에서 수술 도중 개복술로 의 전환이 있어 전환율은 3.2%였다. 원인은 상복부 수술 기 왕력으로 인한 유착이 가장 많았으며(22명, 33.0%), 심한 염 증(21명, 31.0%), Mirizzi's syndrome을 포함한 해부학적 구 조 이상(15명, 22.0%), 악성 종양 의심(3명, 4.5%), 총담관 손 상(3명, 4.5%) 등이었다. 따라서 상복부 수술 기왕력으로 인 한 개복술이 아닌 심한 염증으로 인한 개복 전환율은 1.74%
였다(Table 2).
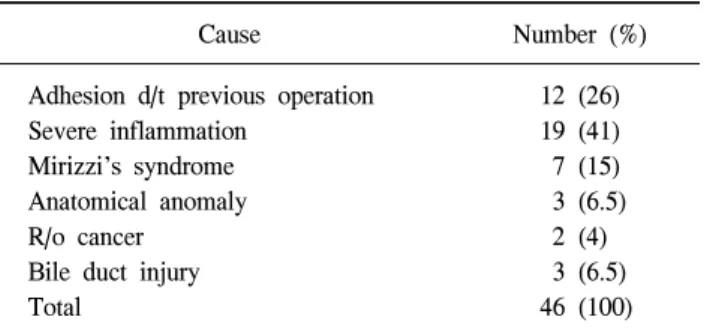
급성 담낭염 환자 893명 중 개복술로의 전환율은 5.2%
(46명)로 심한 염증으로 인한 경우가 41.0% (19명)으로 가장 많았으며, 상복부 수술 기왕력(12명, 26.0%), Mirizzi's synd- rome을 포함한 해부학적 구조 이상(10명, 21.5%), 악성 종양 의심(2명, 4.0%), 총담관 손상(3명, 6.5%) 등의 원인이 있어, 해부학적 구조 이상이 아닌 염증으로 인한 개복 전환율은 3.2%였다(Table 3).
Table 4. Cause of conversion in acute complicated cholecystitis
Cause Number (%)
Adhesion d/t previous operation Severe inflammation
Mirizzi’s syndrome R/o cancer Bile duct injury Total
7 (25) 14 (50) 3 (10.7)
1 (3.6) 3 (6.5) 28 (100) Total conversion rate: 28/374 = 7.5% → conversion rate d/t inflammation: 14/374 = 3.7%.
Table 3. Cause of conversion in acute cholecystitis
Cause Number (%)
Adhesion d/t previous operation Severe inflammation
Mirizzi’s syndrome Anatomical anomaly R/o cancer
Bile duct injury Total
12 (26) 19 (41) 7 (15) 3 (6.5)
2 (4) 3 (6.5) 46 (100) Total conversion rate: 46/893 = 5.2% → conversion rate d/t inflammation: 29/893 = 3.2%.
Table 5. Mortality rate
Hign risk patients
Total
No Yes
PTGBD No Yes
Chronic cholecystitis Acute cholecystitis Total
1,348 (85.4) 230 (14.6) 981 (62.2) 597 (37.8) 1,578
345 (70.6) 144 (29.4) 193 (39.5) 296 (60.5) 489
1,693 374 1,174 893 2,067 Operative mortality: 0%.
급성 합병성 담낭염으로 PTGBD 시행한 374명 중 개복한 환자는 28명으로 7.5%의 개복 전환율을 보였고 이 중 심한 염증으로 인한 경우는 3.7% (14명)였다(Table 4).
3) 수술 전 총담관에 대한 적절한 확인 및 치료
수술 전 총담관 담석이 의심되어 ERCP를 시행한 환자는 427명으로 그 중 임상적으로 담도염이나 담석 췌장염 증상 을 보이거나 혈액검사상 빌리루빈이나 ALP, LDH의 증가 또는 초음파나 복부 CT상 담석이나 담관의 확장이 보이는 348명의 환자에서 ERCP를 시행하여 244명(70.0%)의 환자 에서 총담관 담석을 발견하여 제거하였고, 임상적 또는 혈 액검사, 초음파, 컴퓨터 단층 촬영 상에서는 의심되지 않았 으나 PTGBD 후 시행한 tubogram 상에서 총담관 담석이 의 심이 되어 ERCP를 시행한 환자는 79명으로 이 중 59명 (74.7%)에서 총담관 담석이 발견되어 제거되었다.
4) 수술 사망율
2,067명의 환자 중 70세 미만이면서 합병성 내과적 병력 을 가진 환자 177명과 70세 이상의 환자 312명을 합친 수술 고위험군의 환자는 총 489명이었다. 수술 고위험군 환자 중 60.5%인 296명의 환자는 급성 담낭염 진단을 받은 환자이 고, 이중 144명에서는 급성 합병성 담낭염 진단을 받고 PTGBD를 시행을 받은 후 모든 환자에게서 복강경 담낭절
제술을 시행하였고 수술 후 이 기간 중 시행한 개복 담낭절 제술을 포함하여도 수술 사망은 없었다(Table 5).
고 찰
과거 급성 담낭염의 주 치료는 개복 담낭절제술이었으나 1987년 Mouret에 의해 도입된 이래 현재에는 복강경 담낭 절제술이 급성 담낭염의 표준적 치료법으로 인정받고 있 다.5-8
복강경 담낭절제술 시행 초기에는 급성 담낭염이나 상복 부 수술 병력 등이 금기증으로 여겨져 왔으나 외과의의 경 험의 축적과 수기의 발달에 따라 복강경 수술이 급성 담낭 염의 수술에서도 표준 술식이 되었다. 그러나 급성 담낭염 의 경우 과도한 담낭 팽만이나 담낭 주위의 염증과 주위 장기와의 유착, 불명확한 해부학적 구조(담낭관이나 총수 담관 등), 신생혈관의 발달 등으로 인해 수술 중 과다한 출 혈이나 담관 손상 등으로 개복 수술로 전환되는 경우가 많 았다.9
따라서 수술 사망률을 높이는 기왕증의 확인과 치료가 가능하고 총담관의 결석 유무와 처치가 가능하며 개복술로 의 전환이 최소화될 수 있는 치료방법으로 수술 전 담낭 배액술이 급성 합병성 담낭염의 치료에서 적극적으로 고려 되고 있다.10
본원에서는 급성 합병성 담낭염으로 진단 또는 의심되는 모든 환자에서 PTGBD를 시행하였는데 24시간 이내에 대 부분의 환자들에게서 통증을 포함한 증상의 호전을 보였 다. 이는 PTGBD를 통한 배액으로 급성 염증의 소실과 팽만 된 담낭의 감압으로 인해 증상을 호전 시킨 것으로 보인다.
또한 PTGBD 시행일 기준 약 3주 전후에 담낭절제술을 시 행하였는데, 이 시기가 조기에 수술을 시행하는 것보다 개 복 전환율이나 수술후의 합병증이 적기 때문이다.10 본 연구에서의 대상 환자의 개복술로의 전환율은 3.2%였 고, 이중 급성 담낭염 환자에서의 개복률은 5.2% (46/893)였 으나 상복부 수술 기왕증이 아닌 염증으로 인한 실질 개복
전환율은 3.2%이었으며, 급성 합병성 담낭염 환자에서 염 증으로 인한 개복율은 3.7% (14/374)로 급성 담낭염 환자에 서 보이는 개복 전환율과 비슷한 수치를 보이며, 다른 연구 들에서 보인 개복 전환율의 16∼32%에 비해 현저히 낮은 것을 볼 수 있다.6,7 이는 PTGBD에 의해 담낭과 주변의 염 증을 최소화했기 때문으로 생각된다.
급성 담낭염에서 조기에 복강경 담낭절제술을 시행함으 로써 개복 수술로의 전환과 이에 대한 합병증의 발생을 감 소시키고 있지만 개복술로의 전환이 필요한 경우가 여전히 6∼32% 남아있고 개복술시 수술에 따른 사망률도 3.4% 보 고되었다.11 특히 고령이나 동반질환이 있는 고위험군에서 는 6∼46% (평균 15%)의 수술 사망률이 보고되고 있다.1-3,12-17 이에 대해 최근에는 경피간 담낭 조루술을 시행하고 환 자의 상태가 호전된 후 안전하게 담낭 절제를 시행한 결과 가 보고되고 있고18 본원에서도 PTGBD를 시행한 급성 합 병성 담낭염을 포함한 급성 담낭염 환자에서 담낭 절제술 을 시행한 예와 이 기간 중 개복 담낭절제술을 시행한 전 예에서 현재까지 사망한 환자는 없어 0%의 사망률을 보이 고 있다.
담낭 결석으로 수술하는 환자에서 총담관 결석의 동반 비율은 5∼20% 정도로 알려져 있는데19,20 예측 인자로는 오 한, 발열, 황달의 증상, 확장된 총담관 직경, 간효소 및 빌리 루빈 상승, 담석의 크기가 작으면서 다발성인 경우, 췌장염 이 동반된 경우 등이 있다.21-24 이를 확인하기 위해서는 혈 액검사, 초음파, 담도 전산화 촬영, MRCP 등이 이루어지지 만 가장 좋은 방법은 ERCP이다. 하지만 ERCP는 침습적인 검사로서 모든 환자에게 시행하기는 어려워 혈액검사나 초 음파 검사 등에서 총담관 결석이 의심되는 상황에서만 MRCP와 같이 제한적으로 시행되고 있다.25
Son 등26의 연구에 의하면 PTGBD 후의 담낭 조영술로 담 도의 해부학적 구조를 알 수 있다는 장점과 함께 총담관 결석을 진단하는데 유용하게 사용될 수 있다고 했다. 본 연 구에서도 급성 합병성 담낭염 환자에서 US나 CT상에서는 정상 소견을 보였으나 PTGBD 시행 후 79명의 환자에서 담 낭 조영술에서 총담관 결석이 의심되거나 확진되어 ERCP 를 시행하였고, 이중 59명(74.7%)에서 결석이 발견되었는데 이는 전체 ERCP상 발견된 303명의 환자 중 19.5%에 해당되 는 수치로 PTGBD가 수술 전 총담관 결석의 진단에 도움을 준다는 것과 수술시 총담관 촬영이 필요치 않고 총담관 결 석이 발견된 경우 총담관에 대한 수술이 필요치 않아 환자 의 회복 및 예후에 큰 장점을 보인다는 것을 알 수 있다.
결 론
급성 합병성 담낭염 환자에서 PTGBD 시행 후 경과적 복 강경 담낭절제술을 시행함으로써 급성 담낭염의 증상을 조 기에 소실시키고 환자의 기왕증을 확인, 치료함으로써 수
술 합병증과 사망률을 낮출 수 있으며 총담관 결석에 대한 확인과 처치가 가능하여 치료의 적절성과 편의성이 확보되 며 담낭주위와의 유착을 최소화하여 개복 담낭절제술로의 전환을 최소화할 수 있어 PTGBD 시행 후 경과적 복강경 담낭절제술을 시행하는 것이 급성 합병성 담낭염 환자의 치료에 많은 도움이 되리라 생각된다.
참고문헌
1) Werbel GB, Narhrwold DL, Joehl RJ, Vogelzang RL, Rege RV. Percutaneous cholecystostomy in the diagnosis and treat- ment of acute cholecystitis in the high-risk patient. Arch Surg 1989;124:782-788.
2) Malone DE, Burhenne HJ. Advantages and disadvantages of the newer “interventional” procedures for the treatment of cholecystolithiasis. Hepatogastroenterology 1989;36:317-320.
3) Van Steenbergen W, Ponette E, Marchal G, Pelemans W, Aerts R, Fevery J, et al. Percutaneous transhepatic cholecysto- stomy for acute complicated cholecystitis in elderly patients.
Am J Gastroenterol 1990;85:1363-1366.
4) Masanori S, Makoto T, Yutaka A. Is percutaneous cholecysto- stomy the optimal treatment for acute cholecystitis in the very elderly? World J Surg 1998;22:459-463.
5) Zucker KA, Flowers JL, Bailey RW, Graham SM, Buell J, Imbembo AL. Laparoscopic management of acute cholecy- stitis. Am J Surg 1993;165:508-514.
6) Kiviluoto T, Siren J, Luukkonen P, Kivilaakso E. Randomised trial of laparoscopic versus open cholecystectomy for acute and gangrenous cholecystitis. Lancet 1998;351:321-325.
7) Habib FA, Kolachalam RB, Khilnani R, Preventza O, Mittal VK. Role of laparoscopic cholecystectomy in the management of gangrenous cholecystitis. Am J Surg 2001;181:71-75.
8) Kim HD, Kim HO, Shin JH. Comparison of early versus dela- yed laparoscopic cholecystectomy after percutaneous transhe- patic gallbladder drainage (PTGBD) for patient with compli- cated acute cholecystitis. J Korean Surg Soc 2007;73:329-333.
9) Kim JS, Cho BS, Kang YJ, Park JS. Effect of percutaneous cholecystostomy on laparoscopic cholecystectomy. J Korean Surg Soc 2001;60:78-82.
10) Kim HO, Son BH, Shin JH. Impact of delayed laparoscopic cholecystectomy after percutaneous transhepatic gallbladder drainage for patients with complicated acute cholecystitis.
Surg Laparosc Endosc Percutan Tech 2009;19:20-24.
11) Glenn F. Acute cholecystitis. Surg Gynecol Obstet 1976;143:
56-60.
12) Glenn F. Surgical management of acute cholecystitis in pati- ents 65 years of age and older. Ann Surg 1981;193:56-60.
13) Huber DF, Martin EW Jr, Cooperman M. Cholecystectomy in elderly patients. Am J Surg 1983;146:719-723.
14) Thorton JR, Heaton KW, Espiner HJ, Eltringham WK.
Empyema of the gallbladder: reappraisal of a neglected
disease. Gut 1983;24:1183-1188.
15) Houghton PW, Jenkinson LR, Donaldson LA. Cholecystec- tomy in the elderly: a prospective study. Br J Surg 1985;72:
220-223.
16) Markinen AM, Nordback I. Conventional cholecystectomy in elderly patients. Ann Chir Gynaecol 1993;82:241-245.
17) Prousailidis J, Fahadidis E, Apostolidis S, Katsohis C, Aletras H. Acute cholecystitis in aged patients. HPB Surg 1996;9:
129-133.
18) Klimberg S, Hawkins I, Vogel SB. Percutaneous cholecystos- tomy for acute cholecystitis in high-risk patients. Am J Surg 1987;153:125-129.
19) Thierry M, Simon M, Alain C, Claude R, Nathalie B, Jean-Marie H, et al. Diagnosis of asymptomatic common bile duct stones: preoperative endoscopic ultrasonography versus introperative cholangiography - a multicenter, prospective controlled study. Surgery 1988;124:6-13.
20) Rattner DW, Ferguson C, Warshaw AL. Factors associated with successful laparoscopic cholecystectomy for acute cholecystitis. Ann Surg 1993;217:233-236.
21) Matthew EC, Lori S, Crolyn K, Wells MA, Danna KA, Mark
T. Prediction of bile duct stone and complication in gallstone pancreatitis using early laboratory trends. Am J Gastroenterol 2001;96:3305-3311.
22) Kenny PK, William L. Do preoperative indicators predict the presence of common bile duct stones during laparoscopic cholecystectomy? Am J Surg 1996;171:495-499.
23) Réemi H, Thierry P, Bernadette D, Marcelo S, Jean-Françcois S. Predicting common bile duct lithiasis: determination and prospective validation of a model predicting low risk. Am J Surg 1995;170:38-43.
24) Majeed AW, Ross B, Johnson AG, Reed MWR. Common duct diameter as an independent predictor of choledocho- lithiasis: Is it useful? Clin Radiol 1999;54:170-172.
25) Eom KS, Kim YB, Song YL. Role of endoscopic retrograde cholangiopancreatography (ERCP) before and after LC rela- ting to prediction of CBD stone. Korean J Gastroenterol 2002;
39:40-44.
26) Son DH, Kim KS, Kim KH. Beneficial effect of cholecystography following PGBD for complicated acute cholecystitis: detection of unsuspected CBD stone. J Korean Surg Soc 2009;76:43-45.