Multiple Rice Body Formation in Subacromial and Subdeltoid Bursal Spaces
John Junghun Shin, Jun-Pyo Lee, Doo-Sup Kim
Department of Orthopedic Surgery, Wonju Severance Christian Hospital, Yonsei University Wonju College of Medicine, Wonju, Korea
We encountered a rare condition of rice body in subacromial and subdeltoid spaces in a patient with unremarkable medical history. Al- though it is uncommon, there have been continued reports on its formation in certain type of infective and inflammatory arthritis. How- ever, except for a traumatic event, evaluation yielded no known and conceivable cause for his chronic inflammatory bursitis. Relatively typical findings for rice body on magnetic resonance imaging have been described, and in our case the imaging prompted us to schedule early removal, which is generally accepted as the management of choice to prevent further progression of symptoms. The symptoms of the shoulder showed significant improvement, and a close follow-up schedule has been recommended for observation of recurrence and development of any foreseeable underlying cause.
(Clin Shoulder Elbow 2016;19(2):96-100)
Key Words: Shoulder joint; Subacromial bursitis; Rice bodies
Copyright © 2015 Korean Shoulder and Elbow Society. All Rights Reserved. pISSN 2383-8337
Clinics in Shoulder and elbow Vol. 19, No. 2, June, 2016 http://dx.doi.org/10.5397/cise.2016.19.2.96
Received June 29, 2015. Revised August 13, 2015. Accepted August 23, 2015.
Correspondence to: Doo-Sup Kim
Department of Orthopedic Surgery, Wonju Severance Christian Hospital, 20 Ilsan-ro, Wonju 26426, Korea Tel: +82-33-741-1343, Fax: +82-33-742-1362, E-mail: [email protected]
Financial support: None. Conflict of interests: None.
Rice body is a rare condition commonly arising from chronic inflammation of joint, bursa, or tendon sheath.1,2) Rice body formation from tuberculous arthritis was first described by Riese in 1895,3,4) and since then its association with other infective or inflammatory conditions such as rheumatoid arthritis, non-tu- berculous mycobacterial arthritis, adult-onset Still’s disease, non- specific arthritis, Candida arthritis, juvenile arthritis, seronegative rheumatoid arthritis, and osteoarthritis has been described.4-7) It usually develops as a consequence of chronic inflammation of the confirmed underlying diseases, however there were several cases that had preceded the diagnosis of an underlying cause and presented as initial manifestation.4) In addition, although its origin is generally connected with a nonspecific response to inflammatory synovitis of an underlying cause, several cases without evidence of any pathology have been reported.1,6,8,9) In this case report, we encountered a patient with pain and a mass in his right shoulder who had no previous or current inflamma- tory or infective condition. The patient, a 70-year-old male who had previously undergone arthroscopic rotator cuff repair in his right shoulder, had developed a cystic like mass after a trauma
to the shoulder several months before visiting our clinic, and despite having no underlying cause, rice body was confirmed by magnetic resonance imaging (MRI) and surgical drainage. The patient was explained about the study and agreed to provide informed consent.
Case Report
A 70-year-old male patient visited our outpatient clinic after suffering pain on his right shoulder for two months. He com- plained of pain on movement and a palpable mass in his shoul- der. Arthroscopic rotator cuff repair was performed with two suture anchors four years ago, and he had been lost to follow- up since his last surgery. The patient had a medium size tear on the suprasupinatus tendon, and he stated that had experienced no symptoms after the surgery until the onset of new symptoms two months ago. Except for being on hypertension medication, past history was unremarkable. He had suffered a fall down in- jury from a ladder to the right shoulder four months prior to the visit to our clinic, which was self-resolved within two weeks, and
he did not seek any medical help for the accident. The first two months were uneventful until the development of dull pain that became progressively more severe over the next two months.
In addition, he had noticed a palpable mass (8×8 cm). On physical examination, the mass was soft with some fluctuation and mild tenderness on touch; however, no redness or heating sensation was observed over the mass. He also had a severely limited range of motion due to pain.
At a local hospital, a physician attempted to perform aspira- tion of the mass, but without success, and physical therapy with anti-inflammatory medication was prescribed. This course of treatment did not improve his symptoms. Initial blood work-ups and urinalysis were within normal range except for erythrocyte sediment rate (48 mm/h) and C-reactive protein (3.29 mg/dl), suggesting some inflammatory condition. However, no redness or heating sensation that might indicate acute infection was detected. In addition, he was afebrile, and he did not recall any previous history of infection or joint pain.
Plain radiographic finding was insignificant. To rule out re- rupture of the repaired tendon and to assess the palpable mass, MRI was ordered. On MRI, innumerable delineated small nod- ules were observed in markedly distended subacromial and subdeltoid bursa with a large amount of bursal fluid. The signal showed isointense intensity on a T2-weighted image relative to the skeletal muscle. There was also a partial thickness tear of the rotator cuff on the bursal side, but it did not appear to be com- municating with the glenohumeral joint space. Synovial thicken- ing was also observed (Fig. 1).
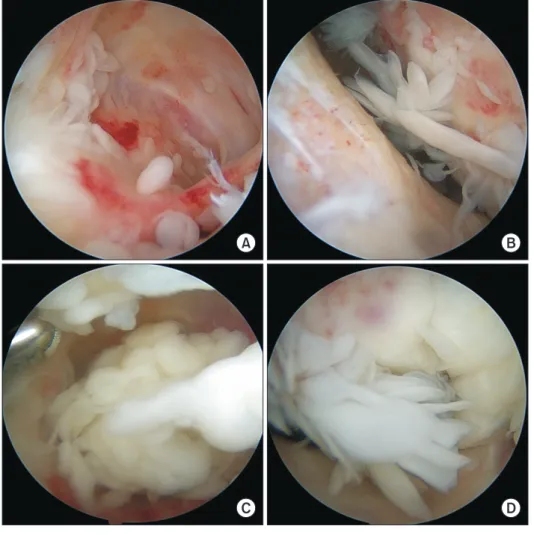
On diagnostic arthroscopy, the glenohumeral joint had minimal synovitis without rice bodies, but it was in a relatively normal state. The previously repaired rotator cuff tendon had healed. However, subacromial bursal space contained multiple rice bodies, some of which showed pedicles attached to the bursal synovium (Fig. 2). The synovium had papillary architec- ture. Arthroscopic debridement was performed for the loose
bodies and bursal surface, but, due to an overwhelming number of bodies and extensive bursitis, we made a small incision on the lateral aspect of the proximal humerus for complete removal of the bursa. Macroscopically, the size of rice bodies ranged from a few millimeters to as large as 15 mm, and they were in various shapes. Some rice bodies appeared to be aggregation of other smaller rice bodies (Fig. 3). Biopsied samples including bursal fluid were sent for pathologic evaluation, and cultures were obtained. His symptoms improved significantly after the surgery.
He recovered normal range of motion for the shoulder without pain on movement, and no palpable mass has been recognized for five months. In addition inflammatory markers were reduced to and stayed within normal range during the follow-ups. Imme- diately after surgery the patient was referred to a rheumatologist for evaluation of medical diseases including rheumatoid arthritis, which may have caused the current inflammatory condition.
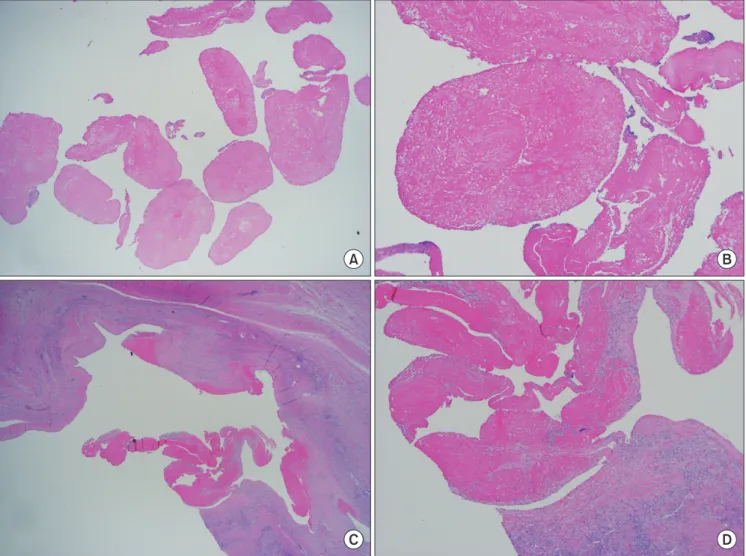
Histologically, small nodules were mainly composed of fibrin- ous materials, consistent with the finding of rice bodies. Bursal tissue showed active chronic inflammatory change without evidence of lymphocytic or mononuclear infiltrates that might suggest rheumatoid arthritis (Fig. 4). However, no granuloma was present in the bursal tissue. Cultures including bacteria, tuberculosis, and fungal infection for bursal tissue and drained serosanguinous fluid showed a negative result. Serologic tests were performed postoperatively for rheumatoid factor and anti- cyclic citrullinated peptide, and they yielded a negative finding.
Antinuclear antibody was positive in a 1:40 dilution. Although positive titer of antinuclear antibody suggests the presence of autoantibodies, positive in a much higher titer is required for the result to have any significance. In addition, since positive antinuclear antibody in a small titer is known to be present in some members of the healthy population, the finding was con- sidered insignificant. Thus, infective or rheumatologic cause of bursal inflammation and rice body formation was ruled out at the moment. However, the rheumatologist, after the review of
A B
Fig. 1. Coronal (A) and sagittal sections (B) of shoulder magnetic resonance imaging show numerous delineated small bodies, and subacromial and subdeltoid spaces are mark- edly swollen with a large amount of bursal fluid.
related articles suggested that presence of the bodies may be a precursor to any underlying systemic diseases. Although he had been closely monitored by the physician, after five months after the surgery he had not developed symptoms associated with the systemic diseases, and the follow-up studies on the serologic
markers were unremarkable. Therefore, the possibility of an un- derlying cause appears to be very low at present.
Discussion
The name ‘rice body’ was derived from its appearance, re- sembling grains of polished white rice.6,9) Although its pathogene- sis remains unclear, it is believed to be a product of a nonspecific reaction to chronic synovial inflammation, and particular infec- tive or inflammatory arthritic conditions were found to be the cause of the chronic inflammation that induces rice bodies.4,9) In addition to formation of rice bodies from joint arthropathy, bursa and tendon sheath are next common place where rice bodies have formed independently. Although rice bodies can form in any of the locations mentioned, some have proposed that rice bodies in joints are commonly related to infective arthritis such as tuberculosis while rice bodies formed in bursa and tendon sheathes are associated more with rheumatoid arthritis.10) Other rare conditions include Candida and osteoarthritis. Muirhead et al.9) reported that penetrating trauma by a date thorn induced synovitis with rice bodies. Popert et al.3) reported that up to 72%
of rheumatoid joints contained macro- or microscopic rice bod-
A B
C D
Fig. 2. Arthroscopy revealed bursitis (A) with many loose bodies in various shapes and sizes (B). There were aggregations of rice bodies (C), and some were still connected to bursal tissue through pedicles (D).
Fig. 3. Gross examination showed varied size and shapes of rice bodies. The size of rice body was as large as 1.5 cm in length, and some appeared to be ag- gregation of multiple smaller rice bodies.
ies after aspiration and lavage. Thus, it is considered a common product of established systemic inflammatory diseases. However, according to several reports, rice bodies had preceded or were the initial presenting sign before making the diagnosis of rheu- matoid arthritis.1,4) Even in a case report, no underlying cause was confirmed for chronic inflammation of bursa and containing rice bodies.8)
Although chronic inflammation of the synovium is generally accepted as the preceding cause of the formation of rice bodies, the actual mechanism of formation has not yet been elucidated.
There are two main theories for the formation.3,7) The first is shedding of microinfarcted synovium and subsequent encase- ment of these bodies with fibrin. The second proposed theory regarding the formation is de novo synthesis in synovial fluid independent of a synovial element that undergoes progressive enlargement with aggregation of fibrin. Its composition differs among studies, and proposed compositions of rice bodies are nodules made up of a fibrin only, collagen core covered by fibrin or a mixture of collagen, retinaculin, and elastin.1,3,6,9)
Symptoms and physical findings vary among reports in the literature. Commonly, patients visit clinics with a painless, non- tender mass on the affected region, but some complain of dull pain and tenderness. With the presence of pain, they may also complain of limitation of the joint’s range of motion. However, diversity in symptoms and signs does not appear to be related to duration or severity of underlying disease. These symptoms and physical findings are non-specific and are present in other diseases that need to be differentiated. In addition, many reports have described heterogeneous appearance of rice bodies having different sizes and shapes.2-4) Although the size ranges from a few millimeters to 2.0 cm, Sugano et al.2) reported on a case of a rice body measuring up to 6.5 cm in size. Again, all of the reports agreed that a larger size does not appear to reflect the duration of underlying disease, because even for the largest size rice body, clinical duration of the patient was only four months and for cases with rice bodies measuring less than 2.0 cm a much longer clinical duration of more than one year was recorded.2)
In addition, laboratory markers are nonspecific and do not
A B
C D
Fig. 4. Multiple loose nodules with fibrinous content consistent with the finding of rice bodies (A: ×1.25, B: ×40; H&E). Formation of fibrinous loose bodies at- tached to the synovium with chronic inflammation (C: ×1.25, D: ×40; H&E).
show correlation with severity or duration of underlying diseases.1) Laboratory work-ups are usually within normal range,5) but elevation of erythrocyte sediment rate, C-reactive protein, or both inflammatory markers may be evident.1) If the underlying cause is unknown, additional work-ups should be performed.
These include rheumatologic markers such as rheumatoid factor and anti-cyclic citrullinated peptide,4) cultures to differentiate an infectious origin. In addition, some cases analyzed cytology of the joint or bursal fluid to rule out tumor, but none of the cases were associated with rice body.1,2,5) Biopsy is also important to confirming the origin of an inflammatory condition. Observation of pannus or granuloma formation provides evidence to make a diagnosis of an underlying cause.
Differential diagnoses for rice body formation in joint include pigmented villonodular synovitis and particularly synovial osteo- chondromatosis,2,4,5) a chronic progressive disease occurring mainly in joints. It is idiopathic metaplasia of subsynovial con- nective tissue into cartilage nodules otherwise normal synovial lining of joint and bursa. Unlike rice bodies, it is not known to be related to inflammatory arthritis. Although the interpretation may not be specific, imaging studies are valuable for differentia- tion of contents and nature of loose bodies in joint and bursa.4,7) In synovial osteochondromatosis, approximately 80% contain mineralized metaplastic cartilage that is apparent on a plain ra- diograph while rice bodies rarely have an ossified component.
For those 20% with unmineralized cartilage containing synovial osteochondromatosis, MRI finding shows an iso- or slightly hyper-intense signal on T1-weighted and a hyper-intense signal on T2-weighted because of the presence of a cartilage com- ponent.8) For fibrin containing rice bodies, the signal intensity for both T1-weighted and T2-weighted is iso- or slightly hypo- intense relative to muscle. The bodies are well delineated on a T1-weighted image, but these may not be distinguishable from surrounding fluid on a T2-weighted image. On the contrary, pigmented villonodular synovitis shows a very low signal or void signal on both T1- and T2-weighted images due to synovial he- mosiderin content. It also has an effect of magnetic susceptibility that is not evident in synovial osteochondromatosis or rice body of inflammation.1,6)
There is scant information regarding established manage- ment of rice body. However, all the reported cases underwent synovectomy with drainage of rice body by arthroscopy or open excision. General agreement regarding treatment of rice body formation appears to be surgical excision and drainage since many previous authors believed that a fibrinous loose body may act as a stimulus for persistence and progression of the chronic inflammation.4-6) These authors reported marked improvement after surgical removal of rice body with synovectomy. Complete excision and drainage is imperative for symptom improvement and prevention of recurrence. No recurrence was reported in
previous literature. Thus, prompt attention and management can provide considerable symptom improvement and potential- ly contribute to a diagnosis of an underlying medical condition that was not known prior to the presentation.
Our case showed typical formation of rice body in chronic inflammatory bursitis. Although several diseases are reported to be associated with the formation, none of the diseases was iden- tified in our patient. Since trauma was the only preceding event, we consider that traumatic bursitis may have provoked the con- dition this time. In addition, we placed the patient under close follow-up because rice body is known to be the initial presenta- tion of underlying rheumatologic pathology.
References
1. Mutlu H, Silit E, Pekkafali Z, et al. Multiple rice body formation in the subacromial-subdeltoid bursa and knee joint. Skeletal Radiol. 2004;33(9):531-3.
2. Sugano I, Nagao T, Tajima Y, et al. Variation among giant rice bodies: report of four cases and their clinicopathological fea- tures. Skeletal Radiol. 2000;29(9):525-9.
3. Popert AJ, Scott DL, Wainwright AC, Walton KW, Williamson N, Chapman JH. Frequency of occurrence, mode of develop- ment, and significance or rice bodies in rheumatoid joints.
Ann Rheum Dis. 1982;41(2):109-17.
4. Subramaniam R, Tan JW, Chau CY, Lee KT. Subacromial bursi- tis with giant rice bodies as initial presentation of rheumatoid arthritis. J Clin Rheumatol. 2012;18(7):352-5.
5. Stein AJ, Case JL, Berman J, Levy H. Case report 770. Chronic subacromial bursitis with massive formation of rice bodies.
Skeletal Radiol. 1993;22(1):71-3.
6. Tan CH, Rai SB, Chandy J. MRI appearances of multiple rice body formation in chronic subacromial and subdeltoid bursi- tis, in association with synovial chondromatosis. Clin Radiol.
2004;59(8):753-7.
7. Jeong YM, Cho HY, Lee SW, Hwang YM, Kim YK. Candida sep- tic arthritis with rice body formation: a case report and review of literature. Korean J Radiol. 2013;14(3):465-9.
8. Chen A, Wong LY, Sheu CY, Chen BF. Distinguishing multiple rice body formation in chronic subacromial-subdeltoid bursitis from synovial chondromatosis. Skeletal Radiol. 2002;31(2):
119-21.
9. Muirhead DE, Johnson EH, Luis C. A light and ultrastructural study of rice bodies recovered from a case of date thorn-in- duced extra-articular synovitis. Ultrastruct Pathol. 1998;22(4):
341-7.
10. Nagasawa H, Okada K, Senma S, Chida S, Shimada Y. Tenosy- novitis with rice body formation in a non-tuberculosis patient:
a case report. Ups J Med Sci. 2009;114(3):184-8.