online©ML Comm
-143- 대한두경부종양학회지
제 25 권 제 2 호 2009
A Case of Schwannoma of Nasal Cavity
Na Rae Kim, MD,1 Heung Eog Cha, MD,2 Dong Young Kim, MD,2 Seung Yeon Ha, MD,1 Dong Hae Chung, MD1
Departments of Pathology,1 Otolaryngology,2 Gachon University Gil Hospital, Incheon, Korea
비강에서 생긴 신경초종 1예
가천의과학대학교 길병원 병리과,1 이비인후과2
김나래1·차흥억2·김동영2·하승연1·정동해1
= 국 문 초 록 =
신경초종은 전신의 말이집신경 중 어디에서나 발생할 수 있는 말초신경집 양성종양이다. 이 종양이 비강에서 발생 하는 것은 흔하지 않다. 저자들은 뇌경색으로 입원하고 있던 55세 여자환자에서 다량의 비출혈을 동반한 비강 신경집 종 1예를 보고하는 바이다. 부비강 컴퓨터단층촬영사진상 좌측비강과 비인두를 채우는 비균질한 저음영의 거대 종양 이 관찰되었고 뼈의 재형성 역시 관찰되었다. 내시경 생검을 시행하였다. 병리검사상, 난원형의 경계가 좋은 병변이 편 평상피로 화생된 비강 점막 아래에서 관찰되었고, 종양은 물결모양의 핵을 가진 방추세포로 이루어져 있었고, 방추형 의 핵들이 밀집하게 모여있는 Antoni A 부분과 세포의 수가 적으며 허술하게 뭉쳐있는 Antoni B 부분으로 이루어져 있었으며 S-100 단백질 면역염색에 양성이었다. 비강의 신경초종으로 진단하였다. 따라서, 흔하지 않게 접하게 되 는 비강 신경초종의 임상양상, 감별진단, 및 치료에 대해 알아보고자 한다.
중심 단어:신경초종·비강.
Introduction
Schwannoma is a slowly growing nerve sheath tumor that can arise from any peripheral nerve that contains schwann cells.1) Schwannoma can grow in any nerve with Schwann cells, and can be found for all parts of the body.2) Yet it is rare for schwannoma to appear in the nasal cavity and pa- ranasal sinuses. To date, eight cases have been retrieved in Korean literature.1,3-8) Here, we report on an additional case of schwannoma that arose from the nasal cavity and the lesion was associated with massive nasal bleeding.
Case Report
A 55-year-old woman presented with an abrupt onset of
disarthria due to infarction of the basal ganglia and pons.
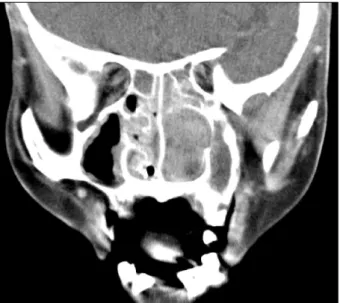
Nasal bleeding occurred on the 10th admission day. She had been suffering from frequent nasal obstruction and rhinor- rhea for the previous one year. No snore or mouth breathing was accompanied. The physical examination revealed that the left nasal mass slightly protruded into the nostril. Para- nasal sinus computed tomography revealed a space-occu- pying mass with heterogeneous low attenuation and this le- sion filled the left nasal cavity and nasopharynx along with bony remodeling(Fig. 1). We performed biopsy under the impression of lymphoma. Microscopically, a well-demarcated, but unencapsulated lesion was found beneath the squamous metaplastic mucosa(Fig. 2A). The lesion was composed of the spindle cells arranged in fascicles(Fig. 2B). The tumor cells had a wavy shape, poorly defined cytoplasm and oval nuclei with tapering ends. The nuclei displayed focally pal- isading with occasional nuclear atypism. Antoni A and B patterns with occasional Verocay bodies were seen. Thick- ened hyalinized vessels and mucosal erosion were also de- 교신저자:정동해, 405-760 인천광역시 남동구 구월1동 1198
가천의과학대학교 길병원 병리과
전화:(032) 460-3866·전송:(032) 460-3073 E-mail:[email protected]
-144- tected. Any mitotic activity was absent. The spindle cells were positive for S-100 protein(polyclonal, Zymed, San Firancisco, CA, USA, 1:1200 diution) and they were negative for cy- tokeratin(AE1/AE3;Dako, Glostrup, Denmark, prediluted) and smooth muscle actin(1A4;Dako, 1:100 dilution). De- spite nasal packing, a blood tinged nasal discharge continued for 2 weeks after the disappearance of the brisk nasal bleed- ing. Surgical excision was postponed until her status became neurologically stable. Later, she refused an operation and so complete excision was not undertaken. She has been well except for mild, but tolerable nasal bleeding during the 6 years of follow-up. There has been no change in the size of the tumor.
Discussion
Schwannoma, as a distinct pathological entity, was first
described as a benign peripheral nerve sheath tumor by Ve- rocay in 1908.9) Grossly, it appears as a gelatinous or cystic long encapsulated mass with occasional secondary changes such as cystic degeneration, hyalinized vessels and necrosis.
Pathologic diagnosis of schwannoma is not difficult. Micro- scopically, schwannoma shows a typical biphasic pattern of cellular Antoni A and paucicellular Antoni B areas;Antoni A areas are composed of spindle cells with twisted, buckled nuclei and occasional intranuclear vacuoles, and the spindle cells are arranged in short bundles or fascicles. The focal areas showing nuclear palisading and whirling of the cells with parallel fibers are named Verocay bodies. Degenerative fibrillar myxoid areas in the paucicellular Antoni B area and hyalinized vessels are the characteristic pathologic findings of schwannoma. Immunohistochemically, schwannoma typ- ically shows a strong, diffuse reactivity for S-100 protein, whereas malignant peripheral nerve sheath tumor shows focal S-100 protein- positivity. Malignant peripheral nerve sheath tumor displays fascicles of atypical spindle cells hav- ing buckled nuclei and are woven into herringbone pattern with varying degrees of mitosis and necrosis. The diagnostic dilemma of malignant peripheral nerve sheath tumor is like- ly to arise from the failure to recognize their nerve sheath differentiation in addition frequent complete absence of S- 100 protein-immunoreactivity.10) Albeit limitation caused by lacking thorough examination of a totally resected nasal mass in the present case, typical immunopathology and favorable prognosis was consistent with benign schwannoma.
Clinically, schwannoma occurs throughout the body. The most frequent site affected in the head and neck is the eighth cranial nerve(vestibular nerve). Other locations include the scalp, face, pharynx, parotid gland, middle ear and external auditory canal.11) However, sinonasal schwannoma is rare and it presents with nonspecific symptoms, including nasal
Fig. 1. Paranasal sinus CT shows a mass with heterogeneous low attenuation along with bony remodeling.
A B
Fig. 2. A:A relatively well marginated mass is composed of spindle shaped cells with buckling nuclei(H&E, ×40). Note the overlying metaplastic epithelium. B:The nuclear palisading patterns form occasional Verocay bodies(H&E, ×200).
-145- obstruction, epistaxis and anosmia.2,3-8) Rarely, schwannoma in the upper nasal cavity involving the olfactory cleft radio- logically mimicking an olfactory neuroblastoma caused head- ache and exophthalmos.4)
Schwannoma developing in the nasal septum is even rarer than schwannoma developing in the lateral wall.12) Unfortu- nately, the precise origin of the tumor could not determined in the present case because we didn’t perform an operation.
Schwannoma occurring in the nasal cavity shows minor pa- thologic differences from those of other locations such as their lack of a peripheral capsule and the frequent ulceration of the epithelial covering.13) Securing the diagnosis on the radiologic basis is also difficult because the appearances of schwannoma on CT is not specific enough to enable it to be firmly distinguished from other tumors in this region. On CT, paranasal schwannoma usually has mottled central hypo- dense foci with peripheral enhancement after contrast. The heterogeneous appearance is related to areas of increased vascularity with adjacent non-enhancing cystic or necrotic regions.
The pathogenesis and natural history of nasal schwanno- ma has not been properly characterized. Schwannoma is a tumor that arises from Schwann cells. The nerve sheath of origin has been regarded as the branches of the trigeminal nerve, which originates from the sphenopalatine ganglion, and the sympathetic nerve originating from the carotid nerve plexus.14) Furthermore, because schwannomas of the para- nasal sinuses are located in a cavity, they are able to grow silently over a long time, allowing them to reach a substan- tial size and thereby surround the nerve of origin.
Complete surgical excision is the treatment of choice for schwannoma.2) It is easily treated with surgery and the pro- gnosis is excellent.15) Radiation therapy may be selected as an adjuvant modality for the cases that complete resection is not possible. Therefore, partial surgery combined with ra- diotherapy would be a possible alternative first treatment for case that total excision might lead to severe sequelae. Remov- al by an endoscopic approach is superior to the external ap- proach because of the reduced morbidity.
References
1) Rhyoo C, Kim SW, Park CS, Cho KJ. A case of nasal cavity neu- rilemmoma diagnosed by S-100 protein. Korean J Otolaryngol- Head Neck Surg. 2002;45(4):412-415(Korean).
2) Buob D, Wacrenier A, Chevalier D, Aubert S, Quinchon JF, Goss- elin B. Schwannoma of the sinonasal tract: A clinicopathologic and immunohistochemical study of 5 cases. Arch Pathol Lab Med.
2003;127(9):1196-1199.
3) Boo SH, Hong JW, Heo MJ. A case of neurilemmoma in the nasal vestibule. J Rhinol. 2008;15(2):140-143(Korean).
4) Choe H, Jun YJ, Cho WS, Kim TH. A case of schwannoma of the nasal cavity mimicking olfactory neuroblastoma. Korean J Oto- laryngol-Head Neck Surg. 2007;50(6):548-551(Korean). 5) Ko DH, Kim KT, Yoon TJ. A case of neurilemmoma in the nasal
vestibule. Korean J Dermatol. 2006;44(6):769-771(Korean). 6) Yoo YS, Yun JW, Choi IK, Kim HS. A case of neurilemmoma of
the nasal vestibule. Korean J Otolaryngol. 1995;38(1):130-134 (Korean).
7) Lim YM, Won SY, Rha KS, Yoo JY, Park CI. A clinical analysis of neurilemmoma originated from the head and neck. Korean J Otolaryngol. 1991;34(4):769-774(Korean).
8) Na DK, Chung MK, Ahn HY, Cha CI. Neurilemmoma of the nasal cavity(Case report). Korean J Otolaryngol. 1986;29(2):240- 244(Korean).
9) Arneaud JD. Neurilemmoma(schwannoma) of the retrotonsillar region. J Laryngol Otol. 1956;70(1):40-43.
10) Weiss SW, Goldblum JR. Malignant tumors of the peripheral nerves. In: Weiss SW, Goldblum JR. Enzinger & Weiss’s soft tis- sue tumors, 5th ed. Philadelphia: Mosby Elsevier. 2008;903-944.
11) Rajagopal S, Kaushik V, Irion K, Herd ME, Bhatnagar RK. Sch- wannoma of the nasal septum. Br J Radiol. 2006;79(943):e16- e18.
12) Park EH, Lee SS, Byun SW. A schwannoma in the nasal septum.
Eur Arch Otorhinolaryngol. 2008;265(8):983-985.
13) Hasegawa SL, Mentzel T, Fletcher CD. Schwannomas of the si- nonasal tract and nasopharynx. Mod Pathol. 1997;10(8):777- 784.
14) Robitaille Y, Seemayer TA, El Deiry A. Peripheral nerve tumors involving paranasal sinuses: A case report and review of the lit- erature. Cancer 1975;35(4):1254-1258.
15) Donnelly MJ, Al-Sader MH, Blayney AW. Benign nasal schwan- noma. J Laryngol Otol. 1992;106(11):1011-1115.